Article Text

Abstract
Introduction Cardiovascular Disease (CVD) is the leading cause of morbidity and mortality in England. There are 130,00 people living with CVD across North East London (NEL), claiming 220 deaths each year.
The relationship of hypercholesterolaemia to CVD is well established, with every 1 mmol/L reduction in Low Density Lipoprotein (LDL) sustained for 5 years, provides a 22% reduction in CVD events.
The national primary care audit has shown only 26% of people with CVD across NEL are on optimal statin with a non-HDL < 2.5mmol/L (LDL <1.8mmol/L) and 16% are not on any lipid modification therapy.
NEL integrated care board is focused on working in partnership to streamline services across secondary and primary care to address health inequalities, improve outcome and deliver high-quality service.
Through the NEL CVD prevention (ELoPE) programme, a new multidisciplinary Clinical Pathway Initiative (CPI) was developed to test innovative integrated services that utilises specialist hospital teams working with primary care teams to optimise CVD prevention across the local population.
Method Redbridge was defined as the first borough to test the CPI. The cohort of people were identified using the UCLPartners Lipid Management Proactive Care Frameworks across 42 practices over a 12-month period, from September 2022.
Specialist cardiovascular pharmacists working with primary care clinicians to identify, review and optimise secondary prevention in high-risk people living with CVD and not receiving a lipid modification therapy.
Clinical notes were reviewed to confirm CVD diagnosis, history of treatment, bloods results and CVD risk factors. Complex cases were reviewed by a virtual lipid specialist multidisciplinary team to agree a treatment plan. Patients were contacted for a virtual consultation to discuss and initiate tailored lipid modification therapy.
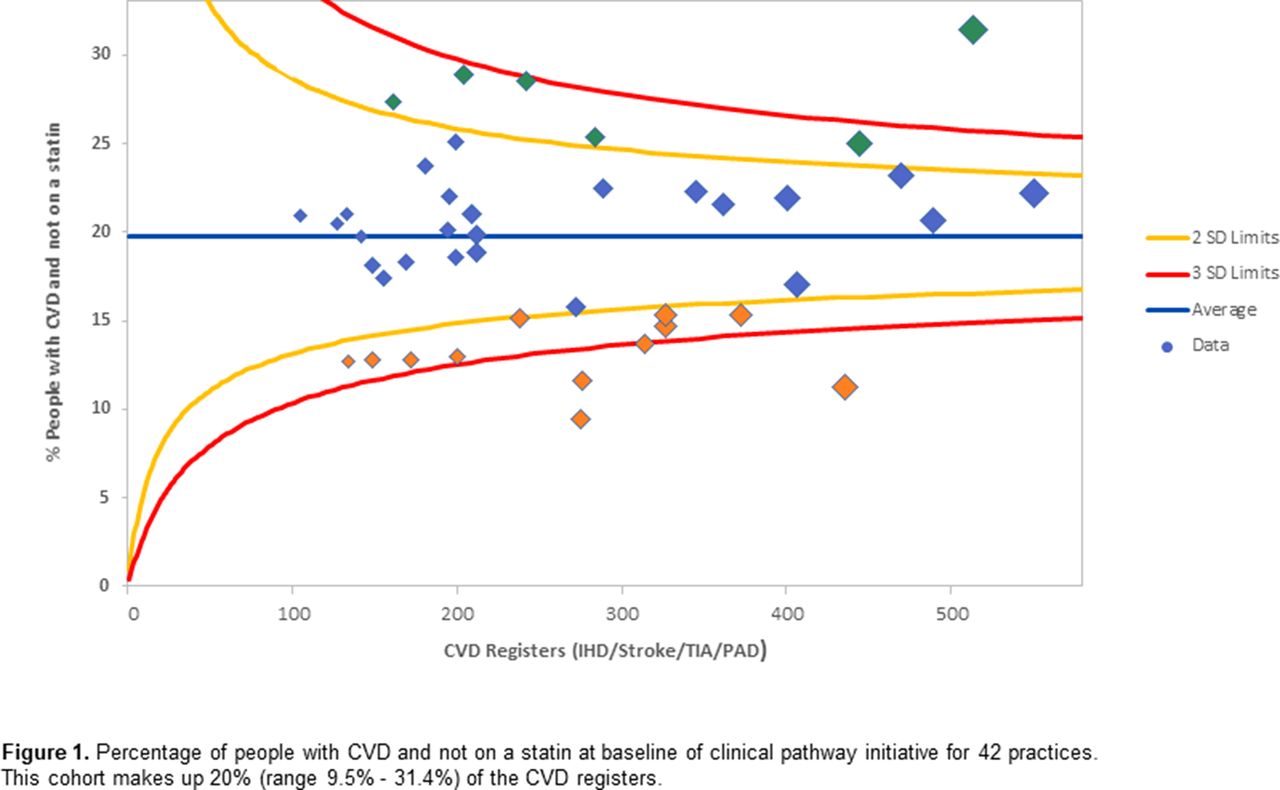
Results A review of GP practices list showed that 20% (2,220/11,233) of people living with CVD in Redbridge were not receiving any lipid modification therapy (see figure 1). Of this group, 60% (1,335/2,220) were previously prescribed one or more statins. This cohort was reduced to 13.4% as shown in figure 2.
By the end of 12 months, 22% (495/2,220) people were rechallenged and (re)initiated on a statin with 2% (51/2,220) receiving a non-statin lipid lowering therapy. Personalise care adjustments were coded for 10% (220/2,220), 5% (110/2,220) declined treatment and 22% (480/2,220) removed from the CVD registers or practice list.
Conclusion A new CPI has established a new service model with a collaborative patient centred approach of secondary care specialist and primary care workforce working together in improving lipid lowering therapy by 24% for people living with CVD and not on a statin. This will prevent 49 CVD events in Redbridge in the next five years. Extrapolating these results for NEL would prevent 458 CVD events over a 5-year period, addressing the NHS long term plan ambition for reducing 150,00 premature CVD deaths by 2029.

Percentage of people with CVD and not on a statin at baseline of clinical pathway initiative for 42 practices. The cohort 20% range 9.5% - 31.4%) to 13.4% (range 7% to 24.7%).

{kind=link}
{kind=link}
Percentage of people with CVD and not on a statin at 12 months of clinical pathway initiative for 42 practices. The has been reduced from 20% range 9.5% - 31.4%) to 13.4% (range 7% to 24.7%).
Conflict of Interest None