Article Text

Abstract
Background Malnutrition is common in patients with heart failure (HF) and is associated with adverse outcome. However, it is uncertain whether changes in nutrition status over time relate to clinical outcomes and quality of life (QoL) in patients with HF.
Objectives To evaluate the change in nutrition status between baseline visit and 6-month follow up and its impact on all-cause mortality, HF hospitalisation and QoL in patients with HF.
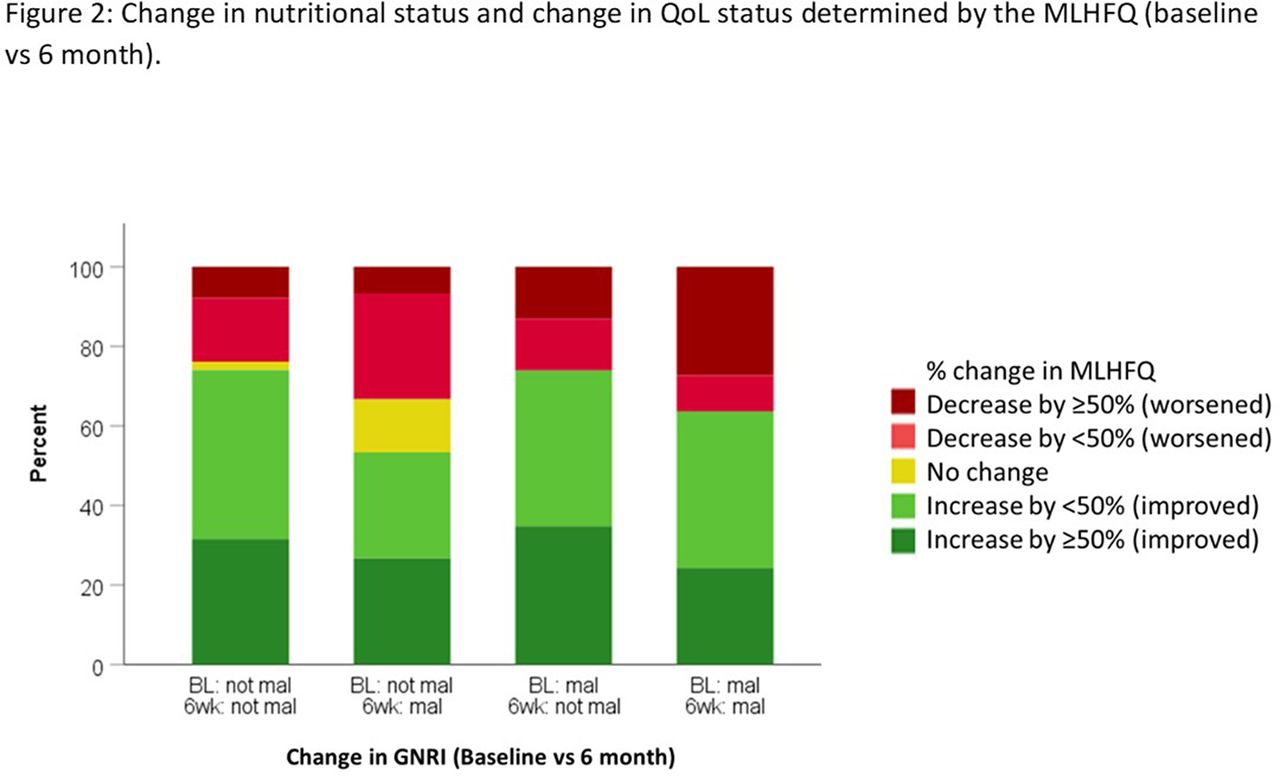
Methods This is a prospective longitudinal study of adults with HF from New Zealand. Patients were recruited either during a HF hospitalisation following stabilisation or from an outpatient setting within 6 months of an episode of decompensated HF. Malnutrition was determined using the geriatric nutritional risk index (GNRI) = [1.489 x albumin (g/L)] + [41.7 x current weight/ ideal weight]. Patients were malnourished if GNRI was ≤ 98. To evaluate the change in nutritional status, we stratified patients into 4 groups: Normal nutritional status at baseline & 6 month (A); normal at baseline, malnourished at 6 month (B); malnourished at baseline, normal at 6 month (C); malnourished at baseline and 6 month (D). The primary outcome was all-cause death. Secondary outcomes were death/ HF hospitalisation and QoL determined using the Minnesota living with HF questionnaire (MLHFQ).
Results 654 patients (72% male, median age 71 years, median NT-proBNP 1641 ng/L, 49% LVEF<40%) were enrolled. 53 (8%) patients were malnourished at baseline and 48 (7%) patients were malnourished at 6 months. Regarding change in nutritional status at baseline & 6 months, 89% (N=584) were stratified into A, 3% (N=17) B, 3% (N=22) C and 5% (N=31) D. Amongst the 4 groups, patients in D were the oldest (median age 84 years), with worst HF (median NTproBNP 3628 ng/L).
During 4 years of follow up, 198 (30%) patients died and 419 (64%) patients had either a HF hospitalization or died. Compared to patients in A, those in B and D had a two-fold increased risk of death and combined outcome (Figure 1) with worse QoL (Figure 2).
A base model for predicting mortality at 1 year including age, NYHA class, log [NT-proBNP], ischaemic aetiology and systolic blood pressure had a C-statistic of 0.80. Addition of change in nutritional status at baseline and 6 months improved the performance of the base model in predicting mortality (C-stat = 0.83, p=0.01).
Conclusion Persistent malnutrition or subsequent development of malnutrition during follow up was associated with increased risk of mortality, HF hospitalisation as well as worse QoL in patients with HF. Future studies should evaluate the effectiveness of interventions targeting nutritional status in improving clinical outcomes in patients with HF.

Kaplan Meier curve showing the relation between change in nutrition status and all-cause death and combined outcome

{kind=link}
{kind=link}
Change in nutritional status and change in QoL status determined by the MLHFQ (baseline vs 6 month)
Conflict of Interest none