Article Text

Statistics from Altmetric.com
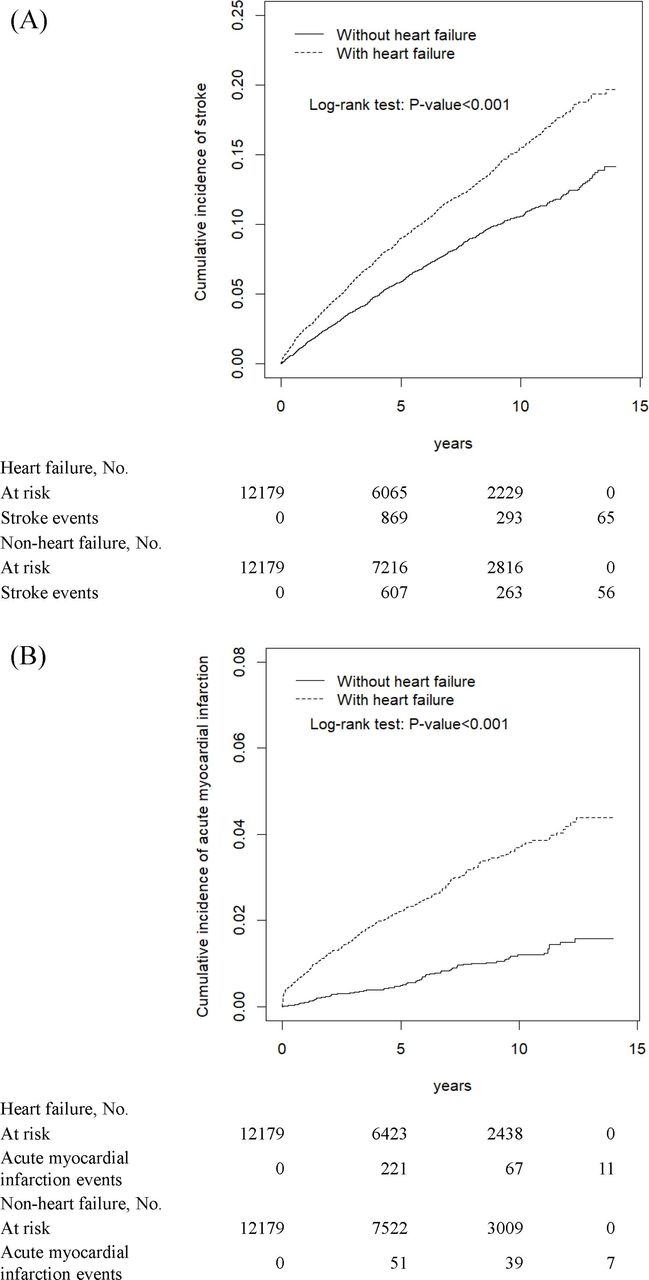
In patients with heart failure (HF), the increased risk of ischaemic stroke often is attributed to coexisting atrial fibrillation (AF). To test the hypothesis that there is a higher risk of ischaemic stroke in patients with HF, even in the absence of AF, Chou and colleagues1 used data from the Taiwan National Health Insurance programme. Over 12 000 patients with newly diagnosed HF were matched by propensity score to the same number of patients without HF, after excluding patients with AF or atrial flutter at baseline or during the follow-up period, as well as patients with previous stroke or acute myocardial infarction. The risk of stroke over a mean follow-up of about 6 years in those with HF was higher than in those without HF (subdistribution HR (SHR)=1.51, 95% CI: 1.37 to 1.66). There also was a higher cumulative risk of stroke and acute myocardial infarction in those with HF (figure 1). In those with HF, multivariable risk factors for stroke were older age, male sex, diabetes and hypertension. These data support the author’s hypothesis that HF itself is associated with a higher risk of stroke in the absence of AF.

Cumulative incidence of ischaemic stroke (A) and acute myocardial infarction (B) in individuals with HF or without HF by propensity score matching. HF, heart failure.
In an editorial, Nelson and Patel2 comment ‘This is one of the larger studies that has attempted to exclude the effect of baseline or subsequent AF on the risk of stroke and myocardial infarction in a contemporary HF population. A key strength of the study is the significant representation of females and those of Asian race—two characteristics often featured as minorities or subgroups in larger studies.’ In addition, they suggest ‘patients deemed at high risk for AF (and/or ischaemic stroke) may be a cohort worthy of upstream intervention—not only do patients with HF have AF more often than not, up to 40% of AF is silent and a large proportion present for the first time with a stroke. Therefore waiting for either stroke to occur or AF to be detected conceivably misses an important window for intervention in a group of patients likely to sustain high rates of morbidity or mortality.’
In patients with AF on oral anticoagulation who are undergoing percutaneous coronary intervention (PCI), the optimal antiplatelet strategy remains controversial. Lupercio and colleagues3 performed a systemic review of both prospective and retrospective studies of patients with AF undergoing PCI that compared dual and triple antithrombotic regimens with endpoints of bleeding and major adverse cardiac events. Overall, based on data from over 22 000 patients with AF on oral anticipation, added treatment with clopidogrel was associated with a lower bleeding risk compared with ticagrelor or prasugrel with no difference in adverse cardiac events (figure 2). However, only 8% were treated with ticagrelor and 2% with prasugrel, whereas 90% received clopidogrel.

Forest plot for the comparative risk of bleeding with ticagrelor versus clopidogrel in combination with oral anticoagulation. AUGUSTUS, antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation; PIONEER AF-PCI, prevention of bleeding in patients with atrial fibrillation undergoing PCI; RCTs, randomised controlled trials; RE-DUAL PCI, dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation.
Thomas et al 4 put this study in context in a thoughtful editorial. ‘Patients with acute coronary syndromes undergoing PCI present a frequent clinical dilemma if they also have AF. They require antiplatelet therapy to prevent stent thrombosis and recurrent myocardial infarction, but also require anticoagulation as stroke prophylaxis for AF.’ The study by Lupercio and colleagues3 ‘is an important study, as data regarding choice of P2Y12 inhibitor in this context are scarce and more information helps enrich the debate.’ However, caution is needed. ‘Observational studies provide some insights but due to the risk of confounding discussed above, they cannot provide the level of confidence needed to change management and guidelines.’
The increased availability of high-output genetic sequencing is providing new insights into the genetic causes of several types of cardiovascular disease. Based on phenotypic and genetic studies of an index patient with cardiomyopathy and 10 of her relatives, Valtola and colleagues5 were able to determine that the Ala143Thr variant of the α-galactosidase A gene (A143T/GLA) is a pathogenic variant with variable penetrance that results in late-onset Fabry cardiomyopathy. Cardiac MRI was useful for detection of early cardiomyopathy in family members carrying this mutation (figure 3).

Cardiac MRI of a man in his 20s with mild cardiomyopathy (A). Left ventricular (LV) was slightly enlarged (left ventricular end-diastolic volume index/end-systolic volume index 115/52 mL/m2) (B, C). T1 time was low 857 ms in the basal inferolateral wall of the LV (arrow and red circle).
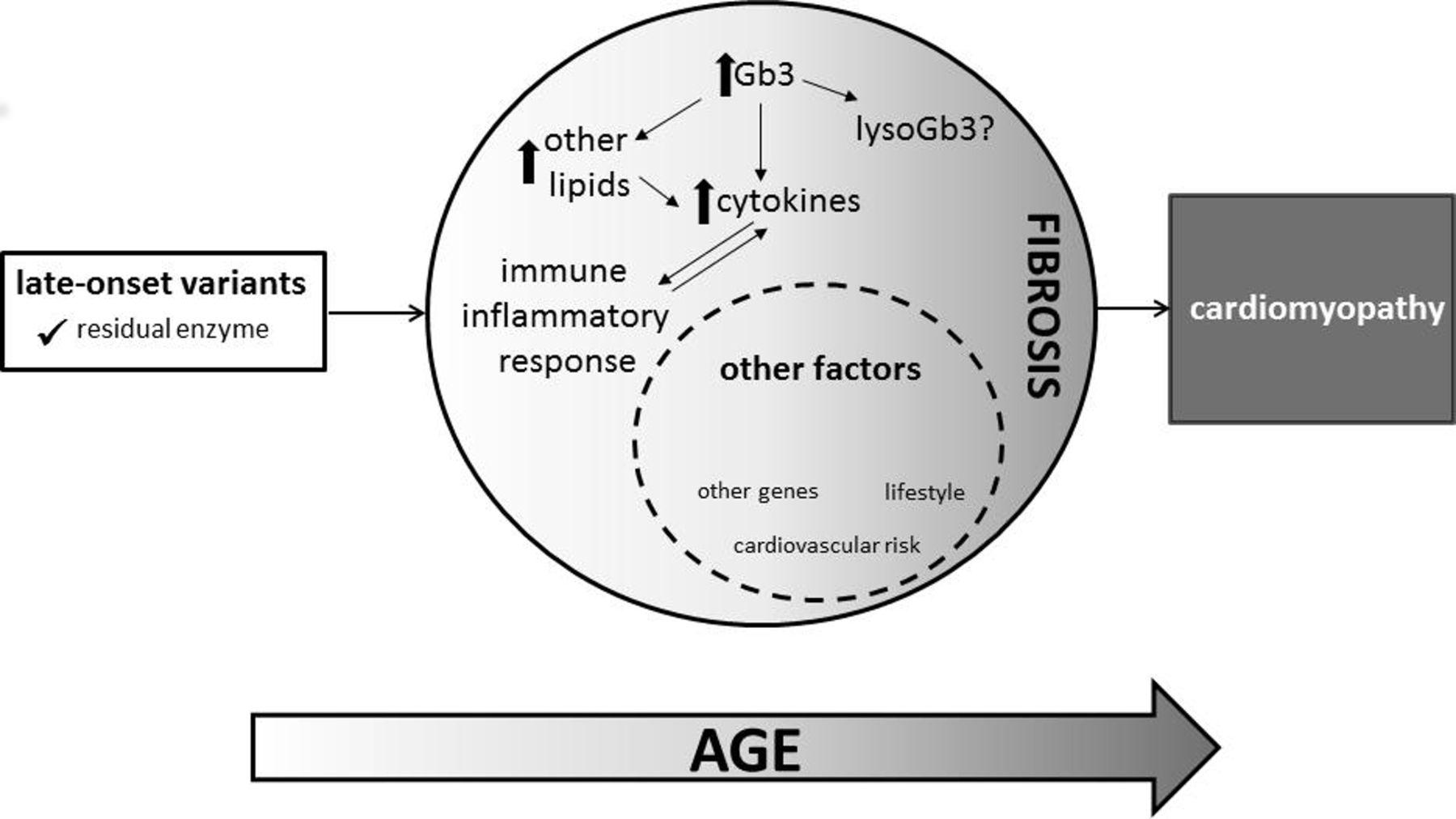
Why should we be interested in studies of rare pathogenic variants that affect only a very small number of patients? One of the most challenging issues in counselling patients with a condition that might be inherited is the finding of a ‘variant of uncertain significance’ (VUS), in contrast to gene variations that are known to be either pathogenic or benign. As genetic testing becomes more common, we need to be able to determine when a VUS is causative in patients (and families) with a phenotype that results in adverse cardiovascular outcomes. The study by Valtola and colleagues5 shows that a careful family history and detailed phenotyping, including imaging, is a reasonable approach to reclassifying a VUS as pathogenic, even when only a small number of people are studied. As Fuller and Mehta6 comment in an editorial: ‘These large pedigrees pose a daunting challenge to healthcare providers across the globe charged with funding care for patients with Fabry disease. The pedigrees also offer an exciting opportunity to study genetic—and environmental—factors influencing phenotypic expression in subjects with the same primary mutation. Prospective studies of cardiac imaging and putative biomarkers will yield important insights into the pathogenesis of cardiomyopathy generally and that associated with Fabry disease in particular’ (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic of cardiomyopathy arising from c.472G>A and other late-onset GLA variants.
Also in this issue of Heart is an outstanding review article on pericardial disease in patients with cancer.7 Our Cardiology in Focus article provides concise guidance on achieving success in consultant applications.8
Footnotes
Contributors All authors contributed.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.