Article Text

Abstract
Objective: To define the scope of injury due to interpersonal violence in a medium-sized town in Western Kenya.
Design: Prospective, cross-sectional data collection and analysis.
Setting/subjects: Data were prospectively collected on all injured patients (n = 562) presenting to a health center in Western Kenya, 2002–2004. Age, gender, type, and severity of injury, relationship to assailant, disposition, and clinician’s suspicion of alcohol use were recorded.
Main outcome measures: Number of injuries due to interpersonal violence; correlation of gender, alcohol use, relationship to assailant, and type of injury.
Results: Interpersonal violence caused 43% of all injuries. Men and women were equally likely to suffer violent injuries (42% vs 45%); however, women were more likely to suffer injury from domestic violence (4.7% vs 7.0%) and sexual assault (0% vs 3.5%). Men and women were equally likely to know their assailant. Women were more likely to be injured by a spouse/partner (19% vs 1.3%), whereas men were more likely to be injured by an acquaintance (29% vs 16%). Alcohol use was more often suspected for victims of violent, as opposed to unintentional, injury (45% vs 16%). Men with violent injuries were more likely than women to be suspected of having used alcohol (51% vs 35%).
Conclusions: Interpersonal violence is a leading cause of injury in Western Kenya. Although men and women are equally likely to be assaulted, women are more likely to be injured by a spouse, and men by an acquaintance. Alcohol use is common among those who suffer violent injuries in this population.
Statistics from Altmetric.com
Injury is a major cause of morbidity and mortality in the developing world.1 Interpersonal violence, in particular, is a growing problem.2 Defined as violence occurring between individuals, it is usually subdivided into intimate partner, acquaintance, and stranger violence. The World Health Organization estimates that 90% of all interpersonal violence occurs in low-income and middle-income countries.3
A major limitation in the effort to characterize injury due to violence and, thereby, plan injury prevention efforts is the lack of accurate data on interpersonal violence in low-income and middle-income countries.4–6 Multiple studies highlight the difficulty of obtaining accurate data on all categories of trauma and injury in sub-Saharan Africa, with resultant hindrance of prevention efforts.7–10 Interpersonal violence is particularly difficult to assess, because of stigma related to its reporting and lack of accuracy of non-healthcare epidemiological sources.11 One study in South Africa suggested that at least two interpersonal violence victims present to healthcare facilities for every one victim who reports to the police.12 This highlights the importance of using healthcare-based research in describing violent injuries and their risk factors.
Data are especially scant on risk factors and correlates of interpersonal violence in sub-Saharan Africa. There is copious international evidence that alcohol is strongly associated with interpersonal violence, as a risk factor for both commission and injury.1314 International literature on interpersonal violence also suggests distinct gender trends in violent injury: more men are victims of violence; women are more likely to be injured by friends and family members; and men are more likely to be injured by strangers.15–17 Few such studies have been published in resource-poor countries. In South Africa, for instance, reports indicate that interpersonal violence is highly associated with alcohol use, especially for men,18 and that women’s injuries are most often due to intimate partner violence.19 However, South Africa is struggling with unique social, political, and economic stressors, and its data may not be generalizable to other African countries.20 In contrast, a study from an urban city in Nigeria reports high percentages of violent injury being caused by strangers for both men and women victims, as well as low percentages of suspected alcohol use by victims or assailants.21 According to a hospital-based study from Lesotho, 40% of women (vs 17% of men) were assaulted by family members, and 30% of victims admitted to alcohol use.22 Because of the lack of literature, the disparities in these few studies’ results are difficult to interpret.
In Kenya, high injury-related morbidity and mortality have been reported. However, most Kenyan research focuses on road traffic crashes, which have been reported to comprise 18–52% of the injury burden seen at many hospitals throughout the country.892324 Sexual assault, but not the larger category of interpersonal violence, has been studied in Nairobi; these studies show high rates of assault of young women, particularly by known assailants.25–27 One study in Eldoret, a city in Western Kenya, noted that the leading cause of injury was assault (40%) among a population of 1304 patients presenting to the district hospital with a chief complaint of “injury.”28
To address the lack of information on frequency and correlates of interpersonal violence in sub-Saharan Africa, this study examines interpersonal violence and its associations, using a prospectively gathered, cross-sectional database on injury patterns in a rural setting in Western Kenya. To our knowledge, this is the first study of its kind in Eastern Africa.
MATERIALS AND METHODS
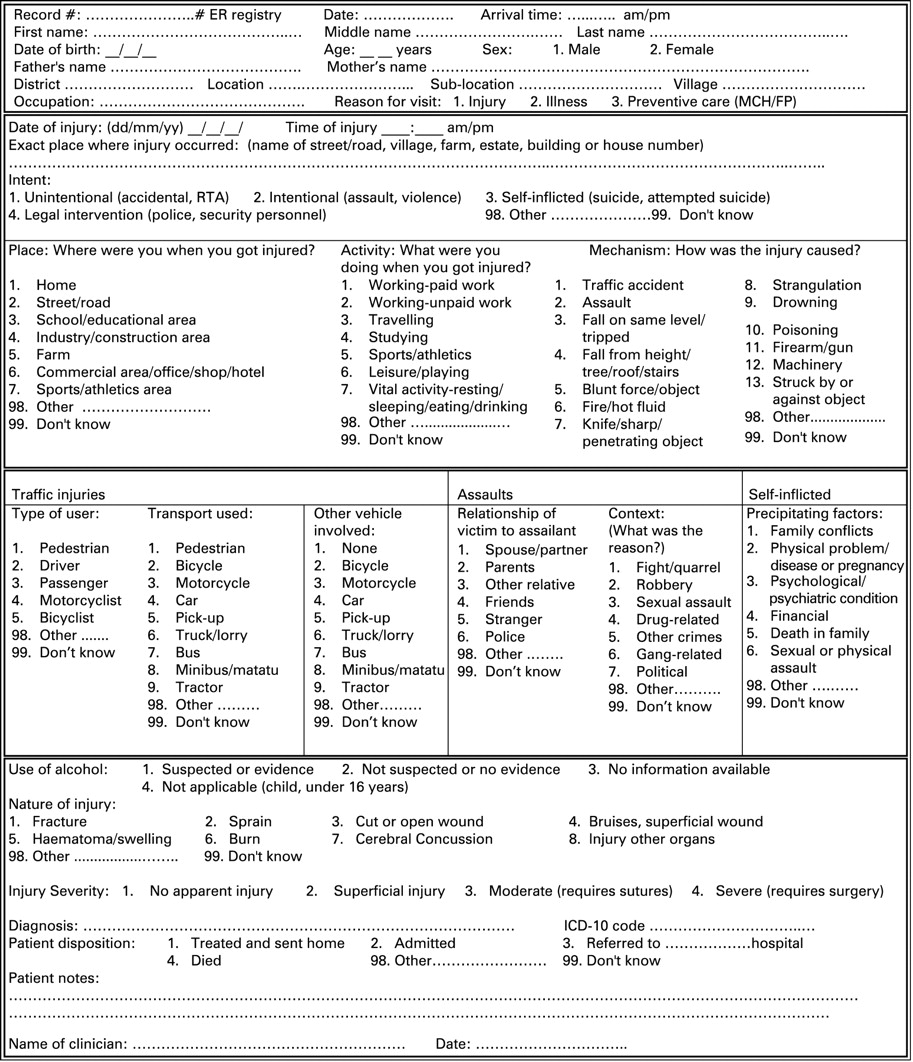
Mosoriot is a medium-sized town in Western Kenya located just west of Eldoret. The Mosoriot Rural Health Centre, funded by the Kenyan Ministry of Health, is the sole health center serving a population of ∼40 000. There is no other source of healthcare in the town or its surrounding villages. The Mosoriot Medical Record System was instituted at the Mosoriot Rural Health Centre in 2001 and was the first electronic medical record system of its kind in sub-Saharan Africa.29 In 2002, an injury-surveillance encounter form was designed, with substantial community input and piloting, following World Health Organization and International Classification of External Causes of Injuries guidelines.30 This instrument was electronically incorporated into Mosoriot Medical Record System as a required data entry form for all injured patients presenting to the health center (fig 1). The resulting database of injured patients was labeled the Mosoriot Electronic Injury Surveillance System (MEISS).

{kind=link}
Through MEISS, injury-specific data were collected on 562 consecutive, acutely injured patients over a 14-month period from November 2002 to January 2004. No injured patients were excluded from the database, and no sampling techniques were used.
The surveillance forms were completed by the clinical officers (mid-level providers) treating the patients, and data were entered into the electronic medical record by nurses and medical clerks. All clinic staff received extensive training on how to use the data form and definitions of injury-specific fields. To complete the data fields, patients were queried about time, location, and type of injury; if applicable, they were also asked about their relationship to the perpetrator. The treating healthcare provider’s impression of injury severity and the patient’s final disposition were recorded. Data collection and entry were regularly supervised and quality controlled by one of the authors (WO). Research assistants also conducted Geographic Information Systems studies on injury locations; this component of MEISS is more fully described in a previous publication.31
As no breathalyzer or reliable blood alcohol tests were available, healthcare providers’ impressions on alcohol use by the victim were recorded. Although this means of assessing alcohol use would not be considered standard in high-income countries, it is the only method available in many low-income and middle-income countries, and clinical impression often serves as the only marker of alcohol use in injury research in the developing world.14213233 In addition, self-reports of alcohol consumption among patients visiting an emergency department have been found to accurately correlate with positive blood alcohol concentrations.34 We therefore consider clinical suspicion to be a marker of alcohol use by the injured patient for the purposes of this study.
We analyzed this database to examine the distribution of injuries due to interpersonal violence in this rural community. In accordance with the research cited in the introduction, we hypothesized that alcohol use would be more strongly related to such injuries (compared with unintentional or self-inflicted injury), and that men with injuries from interpersonal violence would be significantly more likely to have clinical signs of alcohol use than women. We also hypothesized that women would be more likely to be injured by a known assailant, particularly by spouses and family members, as compared with men.
Results were analyzed using descriptive statistics and χ2 tests for significance of associations (Stata V9). Data analysis was approved by the institutional research and ethics committee of Moi University and institutional review boards of Brown University and Indiana University in the USA.
RESULTS
Of the 562 patients presenting to the health center with a chief complaint of injury, 361 (64%) were men and 201 (36%) were women. The mean age was 28.3 years; 125 subjects (22%) were less than 18 years of age. Most injuries were “superficial,” ie, requiring no intervention (406 patients, 72%). Seventeen (3%) had no obvious injury, 42 (7%) required sutures, 13 (2%) had severe injuries requiring transfer and/or surgery, and for 84 (15%) the severity of the injury was not recorded. Correspondingly, 481 of the patients (96% of those for whom disposition was recorded) were discharged home.
Unintentional injuries accounted for 258 patients (45%) in the study. Cause of injury was not reported or was unknown for 57 patients (10% of all patients) in the registry and was inconsistent among categories on the data sheet for six patients (1.6%) (table 1).
A violent cause of injury was listed for 241 patients (43%; 71 women, 125 men) (table 1). Of these violent injuries, 146 (74%) were “fights/quarrels,” 31 (16%) were domestic violence (defined as violent injury caused by an intimate partner, excluding sexual assault), 12 (6%) were robbery, seven (3.6%) were sexual assault, and 45 (32%) were “other.” Of subjects who sustained injury due to fights/quarrels, domestic violence, or sexual assault (n = 184), 70 (38%) were women and 114 (62%) were men.
The relationship with the assailant was listed for 226 patients. The assailant was known to the patient in 91 fights/quarrels (62% of total fights/quarrels), 27 episodes of domestic violence (87% of total domestic violence), three sexual assaults (43% of total sexual assaults), and three robberies (33% of total robberies). Intentional injury was perpetrated by a stranger in only 67 (29%) of these 226 cases. Of the cases of domestic violence that were not due to an assailant known to the victim, the identity of two perpetrators was unknown, and two cases were due to “legal authorities” (police or military). We were unable to determine why these cases were coded as domestic violence.
When relationship with the assailant was analyzed by gender, 64% of women reporting an injury due to interpersonal violence knew their assailant. This accounted for 27% of all injuries (intentional or unintentional) of women in the registry. Similarly, 60% of men who reported a violent injury knew their assailant (23% of all male injuries). However, women were significantly more likely to be injured by a spouse/intimate partner, and men were significantly more likely to be injured by an acquaintance (table 2.) Moreover, women were more likely than men, albeit not significantly so, to be injured by someone known to them in the context of assault, sexual assault, or domestic violence, as opposed to in the context of robbery.
Alcohol use by the victim was suspected for 110 patients (20%), not suspected for 255 (45%), and not recorded or “not applicable” for 197 (35%). Of those patients in whom alcohol use was recorded, men were over-represented (84 of 255 men (32%, 95% CI = 27% to 39%) vs 26 of 110 women (24%, 95% CI = 16% to 33%), OR 1.6 (95% CI 0.95 to 2.6)). Alcohol use was also more likely among male (51%, 95% CI = 42% to 61%) than female (35%, 95% CI = 23% to 47%) interpersonal violence victims (OR 1.9 (95% CI 1.0 to 3.7)). Overall, there was a significant association between intentional injury and clinical evidence of alcohol use (45% of victims of violent injuries used alcohol (95% CI = 38% to 53%) vs 16% of unintentional injuries (95% CI 11% to 22%), OR 4.3 (95% CI 2.2 to 8.3)). There was no association between suspected alcohol use by the victim and severity of injury.
DISCUSSION
This analysis reveals some important points about intentionally injured patients presenting to a rural health center in Western Kenya.
Firstly, there was a high percentage (71%) of violent injury caused by an assailant known to the victim. This association is significantly higher than that reported in a cross-sectional study of police-reported assault in Nigeria.21 The healthcare-based setting of our study may explain the difference: people injured by friends and relatives may be more likely to report minor injuries to healthcare providers than to the police. Our finding lends credence to the growing belief that most interpersonal violence and violent crime occurs between people who know each other. It also suggests that injury prevention and policing efforts in this community should focus on preventing violence between known parties, rather than targeting stranger violence as per current policing guidelines.
Key points
Interpersonal violence is a major problem in low-income and middle-income countries.
The epidemiology and characteristics of interpersonal violence in rural Africa is poorly characterized in the literature.
In a medium-sized town in Western Kenya:
Interpersonal violence is a leading cause of injury.
Most interpersonal violence is committed by perpetrators known to the victim.
Women are significantly more likely to be injured by spouses, and men are significantly more likely to be injured by acquaintances.
Injuries from interpersonal violence are significantly associated with clinical suspicion of alcohol use by the victim.
Secondly, in this group of injured patients, men and women were almost equally likely to be injured due to an assault (42% of injured men versus 45% of injured women). These results differ from WHO data, which report men being more likely to suffer interpersonal violence.3 However, our study examines morbidity only (as none of the patients in the registry was known to have died from his/her wounds), as opposed to WHO data, which primarily reports on mortality. In our population, men and women should be equally targeted for violence prevention efforts if the goal is reduction of morbidity.
Thirdly, the women in this population were significantly more likely to be injured by spouses (and significantly less likely to be injured by acquaintances). This result may have several potential causes. Some studies suggest that Kenyan women (especially rural women) are expected to assume a submissive role to men.35 Other studies have shown associations between traditional gender roles, social inequalities, and risk of interpersonal—and especially intimate partner—violence.536–39
Of note, 57% of reported sexual assaults were perpetrated by strangers. This may be due to a true predominance of sexual assault by strangers.25 However, it may also reflect a lack of reporting of sexual assault by known assailants in Kenya, perhaps because of the country’s legal definition of sexual assault (which exempts marital rape),40 or it may be due to the format in which patients were asked about their cause of injury. Future studies should further examine the reproducibility and etiology of this finding.
Finally, alcohol use was suspected among 45% of intentionally injured victims (and 48% of victims of known assailants) versus only 16% of unintentionally injured victims, with an OR of 4.3. Male victims of interpersonal violence were even more likely to have suspected alcohol use, compared with women. These results suggest that, as in other countries,131418 alcohol is significantly associated with interpersonal violence, especially for men. Although this finding is not surprising, it lends credence to efforts to decrease alcohol use in this region of the world.
Limitations
There are a few major limitations to this study. This is a cross-sectional study in which information was collected at a single rural health clinic in Western Kenya. The results may not be generalizable to the rest of Kenya, in particular to urban centers. The health center is 40 km from a major teaching and referral hospital, so it is possible that more severely injured patients may have preferentially presented to the referral hospital, thereby altering the number and severity of injuries reported in Mosoriot. Approximately 6% of the data were missing from the database, which may have skewed the results; in addition, some categories of injury (eg, sexual assault) were very small. Finally, the reliance on self-report of interpersonal violence, especially domestic violence, and clinician suspicion for assessment of alcohol use may have biased the results.
CONCLUSIONS
Among a population presenting to a rural health center in Western Kenya for treatment of injuries, interpersonal violence was found to be as common as unintentional injury. Although men and women were equally likely to be assaulted, women were more likely to suffer violent injury at the hands of a spouse, and men were more likely to be injured by an acquaintance. A suspicion of alcohol consumption was associated with all injuries in this population, but more strongly so with interpersonal violence. Although we cannot assume that alcohol itself was responsible for the violence, it is likely that efforts to develop community mobilization and injury prevention strategies targeting alcohol consumption would be beneficial in this community. This study also suggests other future research directions, including prospective studies of patterns of intimate partner assault, use of standardized assessments of alcohol, and investigation of community strategies for decreasing interpersonal violence in this community.
Acknowledgments
Steve Reinert, MS, of Rhode Island Hospital/Brown University, for his statistical assistance; William Tierney, MD, of Indiana University, for supporting WO during the design of MEISS.
REFERENCES
Footnotes
Contributors: MLR conceived research questions and was the primary analyzer/interpreter of the data, the primary author, and the guarantor of the paper. WO conceived and designed the database, made critical revisions, and gave final approval. MW contributed to research questions and analysis and made critical revisions. MJM contributed to research questions and analysis, made critical revisions, and gave final approval. RSF contributed to research questions, analysis, and authorship and made critical revisions.
Funding: Initial database design and data collection was supported by a grant to WWO from the National Institute of Health, Fogarty International Center, Medical Informatics Fellowship (1-D43-TW01082).
Competing interests: None.