Article Text

Abstract
Background The role of endogenous androgens for body composition and physical performance in women athletes is still not elucidated.
Aim To examine the serum androgen profile in relation to body composition and physical performance in women Olympic athletes and to compare endocrine variables and body composition to controls.
Study design Cross-sectional study, conducted between 2011 and 2015 at the Women’s Health Research Unit, Karolinska University Hospital, Stockholm.
Methods Swedish women Olympic athletes (n=106) and age-matched and body mass index-matched sedentary controls (n=117) were included in the study. Blood sampling was performed in a rested, fasting state for the measurement of serum androgens and their metabolites by liquid chromatography–tandem mass spectrometry. Body composition was determined by dual-energy X-ray absorptiometry (controls n=100, athletes n=65). The athletes performed standardised performance tests (n=59) (squat jump (SJ) and countermovement jump (CMJ).
Results The athletes demonstrated significantly higher levels of the precursor androgens dehydroepiandrosterone (DHEA) and 5-androstene-3β, 17β-diol (5-DIOL) and the metabolite etiocholanolone glucuronide (Etio-G), significantly lower levels of estrone (p<0.05, respectively), higher bone mineral density (p<0.001) and more lean mass (p<0.001) compared with controls. Serum levels of DHEA, 5-DIOL and Etio-G correlated positively to lean mass variables and physical performance in the athletes. DHEA and lean mass legs explained 66% of the variance in SJ, whereas lean mass explained 52% of the variance in CMJ.
Conclusions The present data suggest that endogenous androgens are associated with a more anabolic body composition and enhanced performance in women athletes. These results are of importance for the current discussion regarding hyperandrogenism in women athletes.
- androgens
- dehydroepiandrosterone
- steroids
- body composition
- elite performance
- female
- athlete
Statistics from Altmetric.com
Introduction
Androgens are considered beneficial for athletic performance by anabolic effects on muscle tissue, stimulating erythropoiesis and the immune system and affecting behaviour.1 2 However, most studies have been performed in men, and surprisingly little is known about endogenous androgens and physical performance in women.
One study showed positive correlations between serum testosterone (T) and explosive performance in women athletes.3 However, another study in four women Olympic weightlifters found no correlation between pre-workout T levels and performance tests.4 On the other hand, women athletes with polycystic ovary syndrome (PCOS) were shown to have the highest performance values compared with non-PCOS athletes.5 Furthermore, the prevalence of hyperandrogenic 46 XY disorders of sex development (DSD) associated with T levels within the male range is many times higher among women athletes than expected.6 These findings suggest that essential hyperandrogenism in women may have performance-enhancing effects.
In addition, exogenous androgens have since the 70s been used to enhance performance with reports of increased power, strength and training capacity.7 These substances are banned from sports and labelled as doping agents. Studies regarding exogenous anabolic androgens in women athletes are few, the exception being experiments performed in the former German Democratic Republic (GDR). Documentation revealed that GDR athletes were exposed to exogenous androgens from an early age and that the performance enhancing effects were especially prominent in women athletes.8
Currently, there is an international controversy whether women athletes with endogenous androgen levels within the male range (about ten times increased) shall be allowed to compete against women athletes with normal androgen levels.9 In 2011, the International Association of Athletics Federation (IAAF) and in 2012, the International Olympic Committee (IOC) implemented regulations concerning women athletes with severe hyperandrogenism.10 These regulations were suspended in 2015 by the Court of Arbitration of Sport pending further evidence of the role of endogenous androgens for athletic performance in women athletes.
In women, androgens are secreted by the ovaries and the adrenal glands, the latter being responsible for the production of precursor androgens (androstenedione (A4), dehydroepiandrosterone (DHEA) and 5-androstene-3β, 17β-diol (5-DIOL)).11 12 A larger part of active androgens (T and dihydrotestosterone (DHT)), those that are able to bind to the androgen receptor, are synthesised in peripheral tissue from DHEA by the mechanism of intracrinology, that is, the transformation of precursor androgens to active androgens within the cell.13 14 Therefore, DHEA is considered a major tissue-specific source of T and DHT in women.14 15 Active androgens are then finally metabolised intracellularly by uridine-diphospho-glucuronosyl transferases to androsterone glucuronide (ADT-G), androstane-3α, 17β-3glucuronide (3α-diol-3G) and androstane-3α,17β-17glucuronide (3α-diol-17G) (5α-reduction pathway) or to etiocholanolone glucuronide (Etio-G) (5β-reduction pathway) and released into the circulation. The former process is considered an important way to maintain androgen homoeostasis by inactivating T.16 Androgen metabolites and precursors have been suggested as a measurement of androgen activity in women.17
The primary aim of this cross-sectional study was to examine the serum androgen profile, including precursors and metabolites in relation to body composition and physical performance in women Olympic athletes and to compare endocrine variables and body composition with controls. Our secondary aim was to compare the androgen profile and body composition between women athletes of different sport categories (power, endurance and technical).
Material and methods
Study population and data collection
Women athletes (>18 years), members of a Swedish Olympic team or part of the high performance programmes of the Swedish Olympic Committee (SOC) received written information about the study. The recruitment was initiated in November 2011 and completed in April 2015 when a representative population of Swedish women athletes participating in the summer (London 2012, n=81) or winter Olympic Games (Sochi 2014, n=45) was reached. Fifteen athletes did not reply. Of those approached in person, five declined, giving a busy schedule, together with living, training and competing at distant locations as the primary reasons. Finally, 106 Swedish women Olympic athletes were included in the study. The athletes were divided into sport categories: Power, Endurance and Technical (table 1).
Classification of type of sport in each sport category for the women Olympic athletes
Age-matched and body mass index (BMI)-matched women having physical activity of maximum 2 hours endurance and/or strength training per week and no prior participation in elite level competition served as controls. Controls were recruited via a Swedish scientific study recruitment webpage (www.studentkaninen.se). Initially, 128 controls were recruited, however, 11 controls were excluded due to prior participating in elite level sports (n=1), training load higher than inclusion criteria (n=8) or too high BMI (n=2). Finally, 117 controls were included in the study.
The subjects were investigated at the Women's Health Research Unit, Karolinska University Hospital or in connection with training camps. Data regarding health problems and gynaecological data (hormonal contraceptive (HC) use, bleeding pattern, menstrual disorders and pregnancies) were collected from all participants. For participants not using HC, menstrual status was categorised as: amenorrhoea (absence of menstruation during at least the previous 3 months), oligomenorrhoea (5–9 periods during the past year occurring at intervals >6 weeks) or regular menstruation (RM) (consistent periods at an interval of 22–34 days). Subjects in the first two categories were defined as exhibiting menstrual dysfunction (MD). Data on sport discipline and training hours per week were collected from the athletes.
A fasting blood sample was collected between 07.00 and 10.00 hour and stored at −20° C until further analysis. Blood samples were collected randomly according to the menstrual cycle. Physical training was not allowed in the morning prior to blood sampling. All subjects were offered an examination of body composition by dual-energy X-ray absorptiometry (DXA). The majority of the athletes performed standardised physical performance tests via the SOC.
The study was approved by the Regional Ethics Committee, Stockholm (EPN 2011/1426-32). Informed consent was obtained from all participants. All subjects were screened for anabolic androgenic steroids at the Doping laboratory, Karolinska University Hospital, Huddinge, none was identified as positive.
Body composition
Sixty-five athletes and 100 controls underwent investigation of body composition (bone mineral density (BMD), fat mass and lean mass) by DXA, Lunar Prodigy Advance (GE Healthcare, Madison, Wisconsin, USA), the same day as blood sampling at the Karolinska University Hospital, Solna. Upper and lower body fat mass (limit between defined as the line drawn from the upper margin of the iliac crest to the neck of the femur) was calculated by the software. Upper/lower fat mass ratio was then established. Spinal BMD was established from the whole body DXA. Z-scores were estimated from the mean BMD and their SD values supplied by the manufacturer of the scanner (Z-score <−2SD is defined as low BMD). Reproducibility has been calculated to be <0.01 g/cm3 or 0.1xSD.18 Lean mass total % and lean mass legs % were calculated by dividing lean mass for the respective section with total mass and total mass legs, respectively.
Physical performance tests
Fifty-nine athletes, mainly of the power group, performed the physical performance tests (see online supplementary table 1), as part of the ‘Physical Profile’ via SOC at the Sports Institute, Bosön, Stockholm. Squat jump (SJ) and countermovement jump (CMJ) were performed and maximum height (cm) recorded using an infrared contact plate, IVAR equipment (IVAR Ltd., Tallinn, Estonia). SJ and CMJ are validated tests for measuring explosive power of the lower limbs.19
Endocrine analyses
Serum levels of T, DHEA, DHEA sulfate (DHEAS), DHT, A4, 5-DIOL, estrone (E1), estradiol (E2), progesterone and androgen metabolites, ADT-G, 3α-diol-3G, 3α-diol-17G and Etio-G, were determined by liquid chromatography–tandem mass spectrometry (LC-MS/MS) at the Endoceutics laboratory, Quebec, Canada, as previously described.20 21 Free androgen index was calculated (T nmol/L divided by sex hormone-binding globulin (SHBG) nmol/L). Follicle-stimulating hormone (FSH), luteinising hormone (LH) and SHBG were determined by electrochemiluminiscence immunoassay (ECLIA) using commercial kits from Roche Diagnostics AG (CH 6343 Rotkreuz, Switzerland) (Cobas8000) at the Department of Clinical Chemistry, Karolinska University Hospital, Solna. Detection limits and within and between assay coefficients of variation were for FSH 0.1 IU/L, 2.6% and 3.6%, for LH 0.1 IU/L, 1.2% and 2.0% and for SHBG 0.04 µg/mL, 1.3% and 2.1%, respectively.
For RM subjects not using HC, menstrual cycle phase was determined. Early follicular phase (cycle days 1–7) was defined as E2 <81 pg/mL, progesterone <1.6 ng/mL and low FSH and LH. Ovulatory phase was defined as E2 ≥81 pg/mL, progesterone <1.6 ng/mL and LH higher than FSH. Luteal phase was defined as progesterone >5.3 ng/mL.
Statistical analyses
Statistical analyses were performed using Statistica 13 software (Statsoft, Tulsa, Oklahoma, USA). Continuous data was presented as mean ± SD or as median and interquartile range (25th–75th percentile) depending on distribution. For normally distributed data (clinical parameters, T, A4, 5-DIOL and body composition), the Student’s t-test was used and otherwise the Mann-Whitney U test was applied to compare athletes and controls. For comparison of anthropometric data and body composition between sport categories (endurance, technical and power), one-way analysis of variance was used followed by pairwise comparisons between groups. p Values were then adjusted according to Bonferroni. Two-way analysis of covariance was used when comparing sport categories regarding serum androgens and androgen glucuronide metabolites (not normally distributed data were log transformed) controlling for HC use and age. Associations between variables were evaluated by the Spearman rank-order correlation. Forward stepwise multiple regression analysis was employed to examine the extent to which the physical performance tests (SJ and CMJ) could be explained by the hormone variables and lean mass variables. After fitting the regression equation, we examined the residuals by Cook’s distance. Extreme cases were excluded and the model was reanalysed. A p value <0.05 was considered statistically significant.
Results
General characteristics, endocrine values and body composition for athletes and controls are presented in table 2.
General characteristics, endocrine variables, androgen metabolites and body composition in controls and Olympic athletes
The frequency of MD was higher among the athletes. However, there was no significant difference between groups in the frequency of HC use, or menstrual cycle phase in RM subjects not using HC (follicular phase: athletes 57% (n=24) and controls 39% (n=24), ovulatory phase: athletes 19% (n=8) and controls 29% (n=18), luteal phase: athletes 24% (n=10) and controls 31% (n=19)) (p=0.20). Among women using HC, the majority used a HC type that inhibits ovulation (88% in the athlete group and 83% in the control group). In addition, the distribution of different hormonal components was comparable between groups (see online supplementary tables 2 and 3).
Serum levels of E1 were significantly lower (p<0.05) and levels of DHEA (32.7%) (p<0.01), 5-DIOL (13.9%) (p<0.05) and Etio-G (26.6%) (p<0.05) were significantly higher in athletes compared with controls (table 2). The subgroup of athletes with MD had higher serum levels of Etio-G than the other athletes (41.9 (32.1–59.4) vs (29.9 (20.8–41.2) ng/mL, (p<0.01). Furthermore, the athletes with MD had lower E1 (34.4 (23.8–68.8) vs 60.3 (40.5–89.5) pg/mL, (p<0.01) and higher Etio-G (41.9 (32.1–59.4) vs 27.5 (17.8–40.3) ng/mL, (p<0.01) compared with controls. As expected, the athletes had significantly higher total and spinal BMD (p<0.001), Z-score (p<0.001) and lean mass variables (p<0.001), whereas body fat percentage was significantly lower (p<0.001) than the controls (table 2).
General characteristics, endocrine values, and body composition for athletes of different sport categories are presented in table 3.
General characteristics, endocrine values and body composition in Olympic athletes of the different sport categories: power, endurance and technical
Athletes in the technical group were significantly older and therefore statistical analysis for all endocrine variables was adjusted for age. Furthermore, endocrine variables were statistically adjusted for HC use. All endocrine variables and androgen metabolites were comparable between groups. The only significant difference was lower SHBG values in the endurance group compared with the other two groups.
The power athletes demonstrated the highest total BMD, spinal BMD and Z-score compared with the other sport categories (table 3). In the whole group of athletes, significant positive correlations were found between androgen levels and total BMD (T (rs =0.31, p<0.05), DHEA (rs =0.28, p<0.05), A4 (rs =0.27, p<0.05)), and between androgen levels and Z-score (T (rs =0.35, p<0.01), DHEA (rs =0.29, p<0.05), A4 (rs =0.30, p<0.05)).
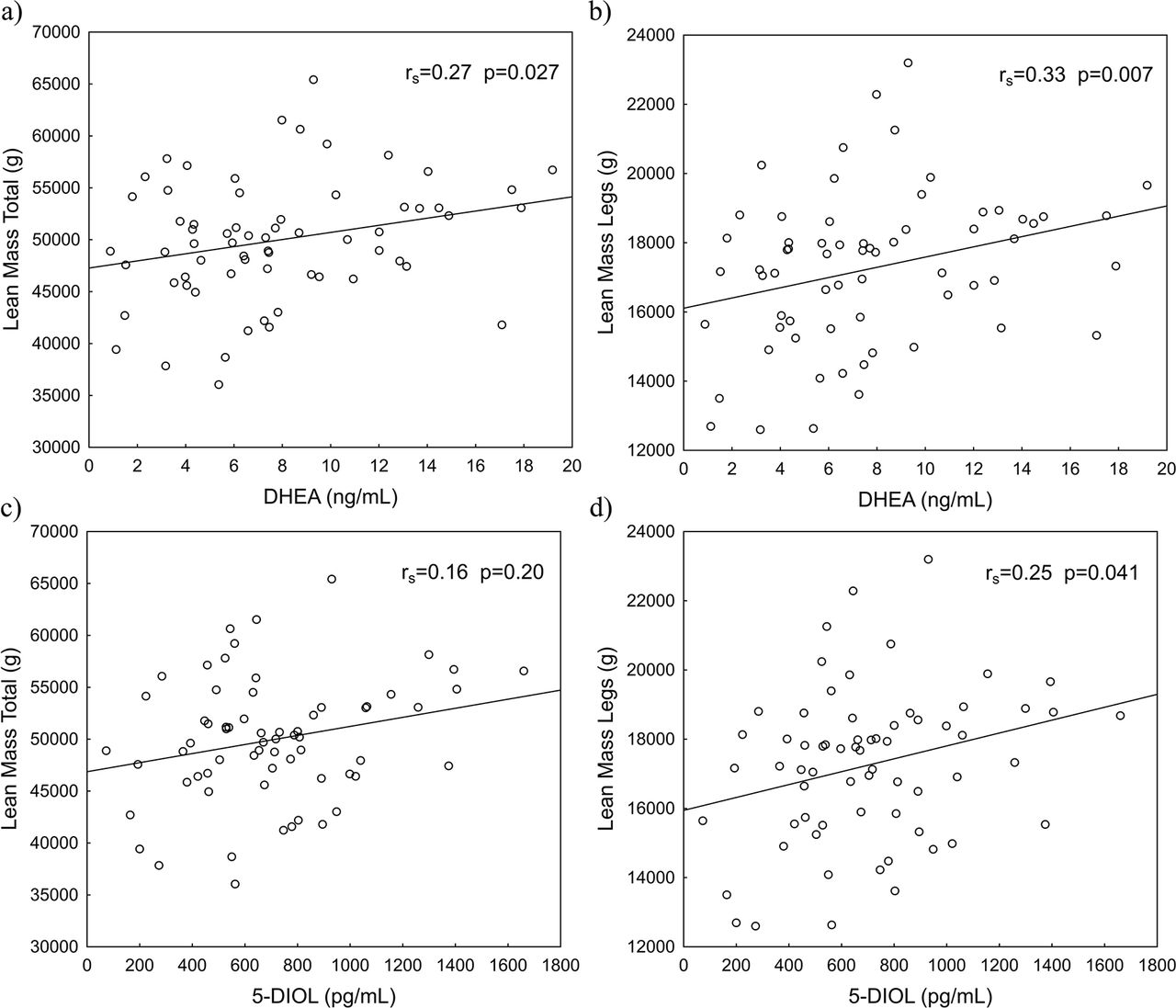
Endurance athletes had the highest lean body mass values and lowest body fat percentage, whereas the technical athletes had the highest fat percent. In the whole group of athletes, serum levels of DHEA correlated positively to lean mass total (g) and lean mass legs (g), and 5-DIOL correlated positively to lean mass legs (g) (figure 1). Etio-G correlated positively to both lean mass total (%) (rs =0.31, p<0.05) and lean mass legs (%) (rs =0.32, p<0.01). Among the subgroup of athletes not using HC, similar significant positive correlations between DHEA, 5-DIOL and lean mass variables were found (see online supplementary table 4).

Correlation of serum androgen precursors with lean mass variables (presented in grams (g)) in women Olympic athletes (n=65). (A) Relationship between DHEA and lean mass total; (B) between DHEA and lean mass legs; (C) between 5-DIOL and lean mass total, and (D) between 5-DIOL and lean mass legs. Significant positive correlations are seen between serum androgen precursors and lean mass variables. DHEA, dehydroepiandrosterone; 5-DIOL, 5-androstene-3β, 17β-diol.
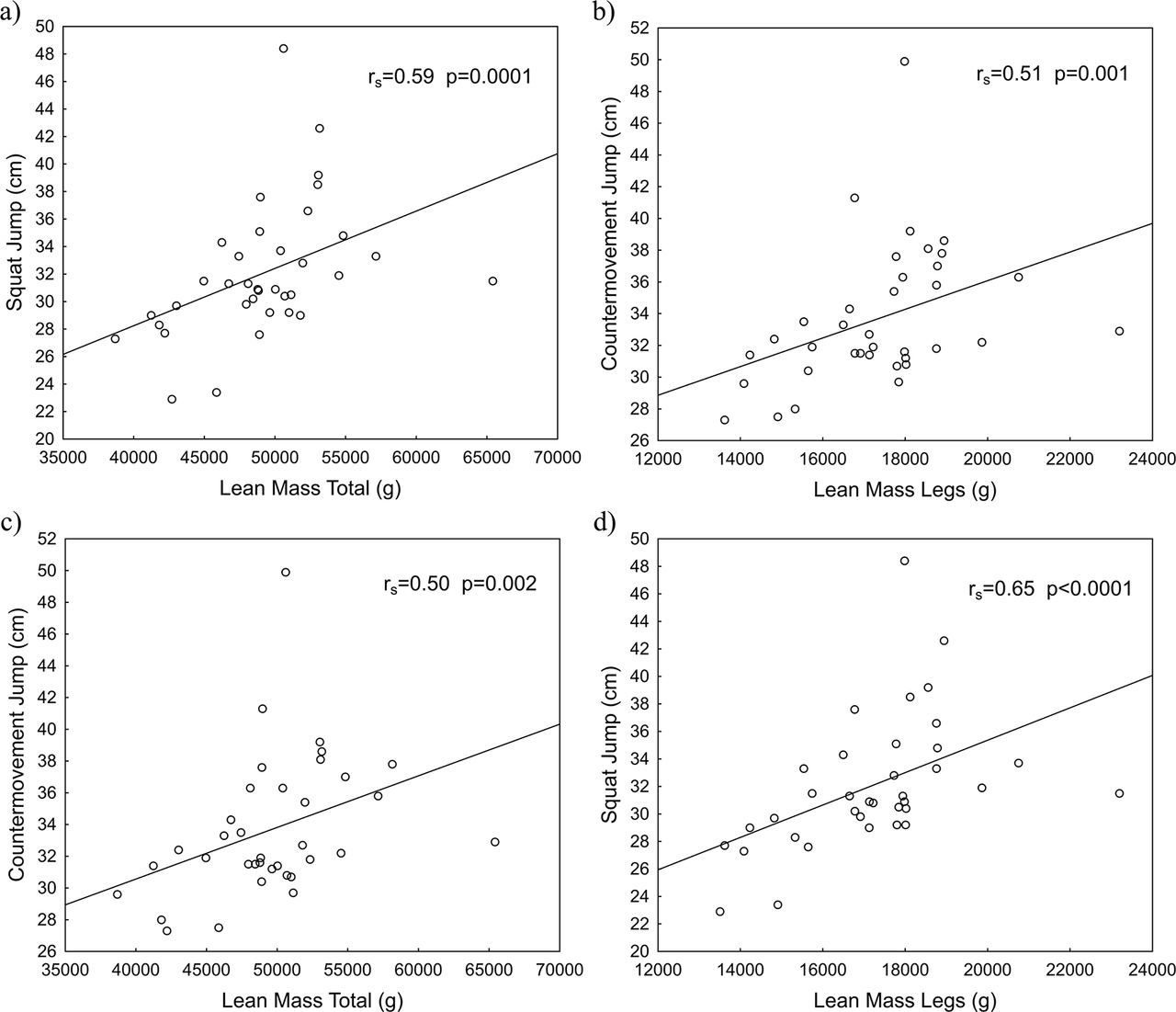
There were significant positive correlations between serum levels of DHEA, 5-DIOL and DHT on the one hand, and SJ and CMJ on the other (figure 2). Most significant correlations for the whole group remained in the group of athletes not using HC as shown in online (supplementary table 5). In the whole group of athletes, serum levels of Etio- G correlated positively to SJ (rs =0.26, p<0.05). The corresponding correlation was found among athletes not using HC (rs =0.36, p<0.05). Figure 3 shows positive correlations between lean mass, SJ and CMJ, respectively.

Correlation of serum androgen precursors and DHT with physical performance tests in women Olympic athletes (n=59). (A) Relationship between DHEA and SJ; (B) between DHEA and CMJ; (C) between 5-DIOL and SJ, and (D) between 5-DIOL and CMJ (E) between DHT and SJ (F) between DHT and CMJ. Significant positive correlations are seen between serum androgen precursors, DHT and physical performance tests. CMJ, countermovement jump; DHEA, dehydroepiandrosterone; DHT, dihydrotestosterone; 5-DIOL, 5-androstene-3β, 17β-diol; SJ, squat jump.

{kind=link}
{kind=link}
{kind=link}
Correlation of lean mass variables (presented in grams (g)) with physical performance tests in women Olympic athletes (n=36). (A) Relationship between lean mass total and SJ; (B) between lean mass legs and SJ; (C) between lean mass total and CMJ, and d) between lean mass legs and CMJ. Significant positive correlations are seen between lean mass variables and physical performance. CMJ, countermovement jump; SJ, squat jump.
Multiple regression analysis was used to evaluate the association between the serum androgen profile, lean mass variables and physical performance. The strongest factor predicting SJ was DHEA (β=0.59, p<0.001), followed by lean mass legs (g) (β=0.42, p<0.001), together accounting for 66% of the variance in SJ, whereas lean mass legs (g) (β=0.65, p<0.001) and lean mass total (%) (β=0.40, p<0.01) were significant determinants of CMJ, explaining 52% of the variance in CMJ. When adding HC to the regression models (SJ and CMJ), no statistically significant interactions were found between HC and lean mass legs or HC and DHEA.
Discussion
Here we report for the first time results on the endogenous androgen profile, including androgen precursors and metabolites, in relation to body composition and physical performance in women Olympic athletes. The athletes had higher levels of DHEA, 5-DIOL and Etio-G, and lower E1 levels compared with controls. As expected, the athletes had a more anabolic body composition with higher values of both BMD and muscle mass than the controls. Athletes in power sports demonstrated the highest BMD values, whereas endurance athletes had the highest values of lean body mass. Importantly, we found positive correlations between endogenous serum androgens, lean mass variables and explosive performance in the athletes. Thus, the present data support a role of endogenous androgens for athletic performance in women athletes.
Serum androgens in athletes and controls
In the present study, we used the golden standard LC-MS/MS method to analyse the detailed androgen profile. We found comparable levels of T between athletes and controls and all individual values were within the normal range, whereas DHEA and 5-DIOL and Etio-G were elevated. Very limited data exist concerning serum androgen levels in women athletes compared with controls. Tegelman et al 22 found no difference in T levels between women endurance athletes and untrained controls. In agreement, another study found comparable T levels between women kayakers, judokas and non-athletic students.23 On the other hand, Rickenlund et al 5 showed that a subgroup of endurance athletes with menstrual disturbance had significantly higher androgen levels than sedentary controls. These athletes were found to fulfil the criteria for PCOS. Similarly, a recent study24 demonstrated that women elite athletes had significantly higher salivary T than non-elite athletes. However, none of these studies used the LC-MSMS method or investigated the full androgen profile.
The specific aetiology of increased androgen precursors and lower E1 levels in the athletes is not known. Exercise-induced elevation of androgens is not likely the cause since blood sampling was performed in a resting state and DHEA and other hormones have been shown to return within hours to baseline values post-exercise.25 Furthermore, doping was excluded and no one was diagnosed with any form of DSD. However, there was an increased occurrence of MD among the athletes and this subgroup had higher serum levels of Etio-G than the other athletes and higher levels of Etio-G and lower levels of E1 than the controls, which could at least partly explain different endocrine values between the groups. Previous studies have suggested that PCOS is common among athletes.5 6 26 In this study, we were not able to assess the occurrence of polycystic ovaries with gynaecological ultrasound. Although the athletes did not have increased levels of T, it is possible that at least some of them, particularly those with MD, had PCOS since this condition is also associated with enhanced secretion of precursor androgens.27
Serum androgens, body composition and physical performance
As expected, women athletes demonstrated a more anabolic body composition and lower body fat percentage than controls. Athletes in higher impact sports, such as power sports, had higher BMD than endurance or technical athletes. This has previously been explained by training load and bone adaptation.28 29 Furthermore, leanness with low body fat content and high amount of lean mass have been reported previously for endurance athletes.26 In addition, we here demonstrate significant associations between endogenous androgen precursors and metabolites versus lean mass and physical performance, respectively, and between lean mass and physical performance in women Olympic athletes.
We found no correlation between serum T and physical performance. As far as we know, there are only two previous studies investigating serum T levels in association with explosive performance in adult women athletes. Cardinale and Stone3 demonstrated a positive correlation between T levels and CMJ in 22 women athletes, whereas Crewther and Christian4 measured salivary T in four women Olympic weightlifters and found no correlation between pre-work out T and performance tests. Moreover, women athletes with PCOS and enhanced secretion of androgens have been demonstrated to perform better than other athletes.5
However, we found that serum levels of DHEA, 5-DIOL and Etio-G correlated positively to lean mass variables. Furthermore, DHEA, 5-DIOL and DHT correlated even more strongly to explosive performance, suggesting that androgens have a significant role for physical performance in women. This was supported by multiple regression analysis showing that the strongest factor predicting SJ performance was DHEA, whereas lean mass was the most significant determinant for CMJ.
In male athletes, studies concerning exogenous DHEA have not been able to demonstrate an anabolic effect.30 This is not surprising since men produce substantial amounts of endogenous T from the testis and the amount generated from DHEA is relatively small.2 31 The same relationship is possibly also true for women with supra-physiological levels of T, while for women with T levels within the normal range, DHEA might be of greater importance for physical performance.31 One could reasonably speculate that higher serum levels of DHEA result in more substrate for intracrine androgen formation and thereby increased anabolic effects. This would explain our finding that DHEA correlated positively to physical performance in the athletes. Furthermore, when adding DHEA to muscle biopsies obtained from non-athletic women, intramuscular T concentration but not E2 increased significantly. In addition, intramuscular hormone levels of E2, T, DHT and DHEA were proven to be independent predictors of muscle strength and power.32
Strengths and limitations
In order to overcome potential factors that could influence circulating androgens, blood sampling was standardised according to time, food intake and physical activity. However, we were not able to take into account the phase of the menstrual cycle as well as HC use. On the other hand, Guerrero et al 33 found no significant variation in DHEA, 5-DIOL and DHT during the menstrual cycle, and in our study cycle phase did not differ between athletes and controls. The frequency of HC use was comparable between athletes and controls. However, when comparing hormonal values between sport categories, the analyses were statistically adjusted for HC use and age. In addition, when adding HC to the regression models no significant interaction was found between HC and lean mass legs or HC and DHEA. Moreover, most of the significant correlations between endogenous androgens, lean mass variables and physical performance for the whole group remained in the subgroup of athletes not using HC.
Another limitation is incomplete data concerning body composition and physical performance tests. Due to practical reasons, not all athletes were able to perform these tests in connection with the blood sampling and other data collection. One strength of the study was, however, that the physical performance tests were conducted in a standardised manner by the instructions of SOC at their training laboratory. Furthermore, we used the highly specific, golden standard method LC-MS/MS for analysis of the androgen profile.20 21
Conclusion
The present study demonstrates higher levels of precursor androgens and metabolites in women Olympic athletes than controls and significant correlations between androgens, lean mass and physical performance in the athletes. These results support a significant role of endogenous androgens for athletic performance in women, which is highly relevant for the ongoing dialogue regarding women athletes and hyperandrogenism.
What are the findings?
This is the first study examining the endogenous serum androgen profile, body composition and physical performance in women Olympic athletes.
Women athletes have higher serum levels of dehydroepiandrosterone, 5-androstene-3β, 17β-diol and etiocholanolone glucuronide and lower estrone levels compared to controls.
In women athletes, precursor androgens and metabolites positively correlate to lean mass and muscle performance.
We suggest that endogenous androgens are associated with a more anabolic body composition and enhanced physical performance in women athletes.
How might it impact on clinical practice in the future?
The results are of importance for the current discussion regarding potential benefits of endogenous hyperandrogrnism in women athletes.
Acknowledgments
The authors would like to thank research midwifes, Berit Legerstam and Lotta Blomberg and research nurse Siv Rödin Andersson at the Women’s Health Research Unit, Karolinska University Hospital for logistical support. They also thank coaches and athletes for their help in contributing to sport medicine research, statistician Elisabeth Berg for continuous help with statistical analyses and the SOC for their valuable support in recruiting and promotion of this scientific work.
The study was financed by grants from the Swedish Research Council, the Swedish Research Council for Sport Science and the Clinical Scientist Training Programme (CSTP) from Karolinska Institutet.
References
Footnotes
Contributors All authors listed met the conditions required for full authorship. EE, BB and ALH were involved in concept/design of the study, acquisition of data and data analysis. FL performed the quantification of serum androgens. EE, BB, FL, KC, LE and ALH were involved in the manuscript preparation, critical revision of the article and approval of the article.
Competing interests EE, LE and KC have nothing to declare. FLis the president of EndoCeutics, BB is the current medical director for SOC and ALH is a medical advisor to SOC, IAAF and IOC.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Regional Ethics Committee, Stockholm (EPN 2011/1426-32).
Provenance and peer review Not commissioned; externally peer reviewed.