Article Text

Statistics from Altmetric.com
The procedure for intrauterine device (IUD) insertion can cause pain or discomfort. The Faculty of Sexual and Reproductive Healthcare (FSRH) recommends discussing and offering pain relief for IUD insertions to all women.1 2 The use of local anaesthesia (LA) is one of the ways to avoid or manage pain during IUD insertion. However, not all clinicians routinely offer LA for IUD insertions.
There were differences in the uptake of IUD insertion appointments in our service between clinicians related to LA. Appointments with clinicians who routinely offered LA for IUD insertions were fully booked weeks in advance compared with appointments with clinicians who did not. To support timely, equitable, patient-centred care and eliminate this disparity, the service created a project and team to explore ways to ensure LA for IUD procedures was routinely discussed, offered and provided by all IUD-inserting clinicians.
Our service was the largest in North East England, with over 32 000 attendances and 1600 IUD insertions a year. IUD insertion appointments at the time were booked in person or via telephone with either doctor (n=10) or nurse (n=5) IUD-inserting clinicians, of whom 87% (n=13) participated in the project surveys.
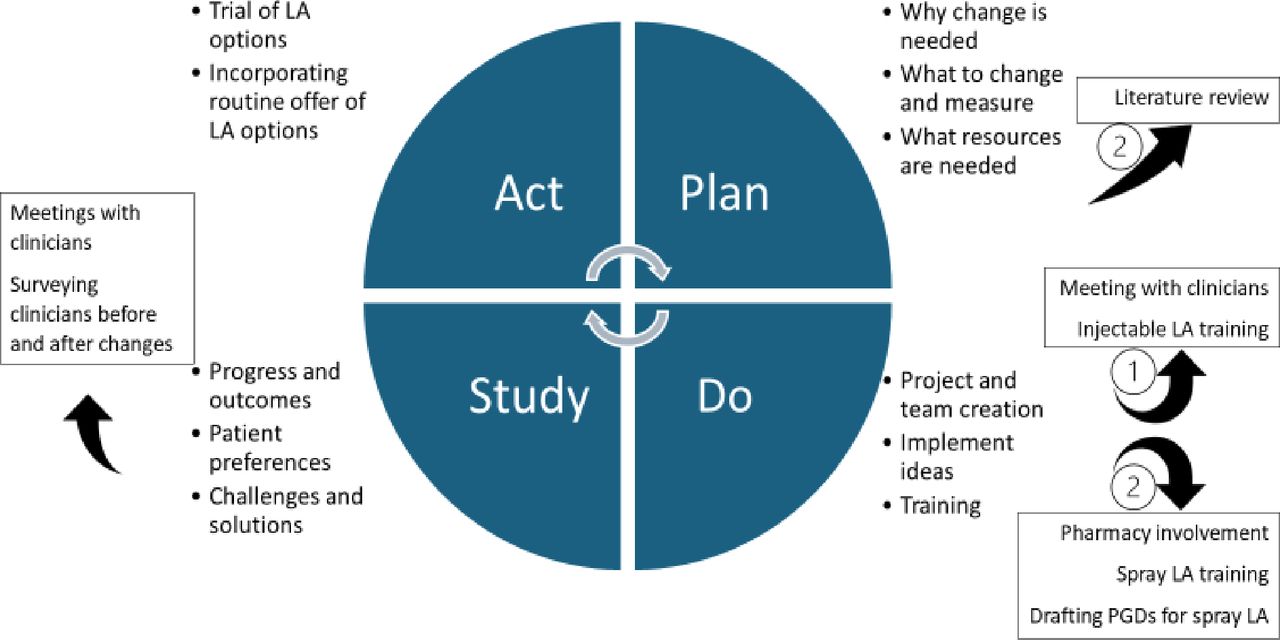
For this project, the team chose the Model for Improvement approach.3 This involved an iterative process of planning, doing, studying, acting and then repeating based on the evaluation and outcome(s) from the previous cycle (figure 1).

{kind=link}
Model for Improvement for project including details during the first (1) and second (2) cycles. LA, local anaesthesia; PGDs, patient group directions.
Topical gel and injectable LA were available in the service, but many clinicians were not trained or confident with injectable LA. Clinicians who were unable to confidently provide injectable LA were trained during the first improvement cycle. An evaluation some months later showed no increase in the number of clinicians who routinely offered or provided injectable LA. This was reported to be due to persisting challenges of ease (including equipment needed, time for assembly and administration, and having to seek a medical colleague to prescribe the injectable LA), lack of clinician confidence to routinely offer an injectable, and patients declining injectable LA. Further meetings led to incorporating another LA option, LA spray, for the second improvement cycle (see figure 1 and online supplemental material LA spray guidance for clinicians).
Supplemental material
A trial of LA spray use was done over a period of 6 months (March 2021–August 2021). The second cycle evaluation showed that uptake of appointments between clinicians had levelled out, with the proportion routinely offering and using LA for IUD insertions increasing from 83% (n=10) to 100% (n=13). LA spray was reportedly easy to use, quick acting, effective, less expensive and more environmentally friendly from the survey (see online supplemental material table) and team meetings, as well as more acceptable to patients compared with injectable LA.
Supplemental material
Our project aim, namely for clinicians to routinely discuss and offer LA pain relief and eliminate a potential disparity in care, was achieved but in a different way to that anticipated at the outset, and led to the successful implementation of change that incorporated LA spray.
Our advice to others considering change is that implementing this improvement required team discussions as well as considerations of motivators for and against LA options. The initial assumption that it was a lack of injectable LA training that was the primary inhibitor proved inaccurate. It is therefore important to be mindful that a simple intervention may constitute part of a complex system within healthcare provision when it comes to implementation.
Another FSRH resource to support improving IUD pain management is the national patient group directions (PGD) template, to support LA use by non-prescriber clinicians.4 Incorporating knowledge or evidence into practice can, however, be unique to local contexts. In addition to team effort and time, also consider patient input or representation for a project team.5
Data availability statement
The data that support the findings of this study are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors are grateful to the clinicians who anonymously participated in the surveys, the service team and other staff who supported this project.
Footnotes
Contributors HA: project design, documents, searches, tasks, data collection and summary, writing – original draft, project administration. CM: project design, documents, tasks, writing – review and editing, project administration. NB: project reporting, statistical advice, writing – draft, review and editing. KMC: project idea, documents, tasks, supervision, writing – review and editing. All authors approved the final version. HA is the author acting as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.