Article Text

Abstract
Objectives: To examine the size and direction of osteophyte in knee osteoarthritis (OA) and to determine associations between osteophyte size and other radiographic features.
Methods: Knee radiographs (standing extended anteroposterior and 30 degrees flexion skyline views) were examined from 204 patients referred to hospital with symptomatic knee OA (155 women, 49 men; mean age 70, range 34–91 years). A single observer assessed films for osteophyte size and direction at eight sites; narrowing in each compartment; varus/valgus angulation; patellofemoral subluxation; attrition; and chondrocalcinosis using a standard atlas, direct measurement, or visual assessment. For analysis, one OA knee was selected at random from each subject.
Results: Osteophyte direction at the eight sites was divisible into five categories. At all sites, except for the lateral tibial plateau and the medial patella, osteophyte direction varied according to (a) the size of osteophyte and (b) the degree of local narrowing. At the medial femur, medial tibia, and lateral femur osteophyte direction changed from being predominantly horizontal to predominantly vertical with increasing size. The size of osteophyte correlated positively with the severity of local narrowing, except for the medial patellofemoral compartment where osteophyte size correlated positively with the severity of narrowing in the medial tibiofemoral compartment. Logistic regression analysis showed that osteophyte size was associated not only with local narrowing but also with local malalignment and bone attrition, and that chondrocalcinosis was positively associated with osteophyte size at multiple sites.
Conclusion: In patients referred to hospital with knee OA different patterns of osteophyte direction are discernible. Osteophyte size is associated with local compartmental narrowing but also local alignment and attrition. Chondrocalcinosis is associated with osteophytosis throughout the joint. These data suggest that both local biomechanical and constitutional factors influence the size and direction of osteophyte formation in knee OA.
- osteoarthritis
- knee
- osteophytes
- chondrocalcinosis
- radiographs
- OA, osteoarthritis
- PFJ, patellofemoral joint
- TFJ, tibiofemoral joint
Statistics from Altmetric.com
Osteoarthritis (OA) is the most prevalent form of arthritis.1 It shows a strong association with aging and selective targeting of certain joints such as the knee.1 A variety of genetic, constitutional and environmental risk factors for OA are recognised, which vary according to joint site.2 The defining radiographic features of OA are (a) focal cartilage loss, resulting in “joint space narrowing” and (b) accompanying endochondral ossification at the joint margins that produces “marginal osteophyte”.1, 3
Although osteophyte is viewed as a remodelling and reparative feature of OA, the factors that determine osteophyte formation and growth are unknown. Growth factors influence both chondrocyte synthesis and osteophyte formation in experimental joint damage,4, 5 and evidence from animal6 and human studies7–9 shows that cartilage damage initiates “secondary” osteophyte growth. However, osteophyte may also develop as an isolated feature associated with age10 and precede rather than follow cartilage loss in animal studies.11 Joint instability has been emphasised as a biomechanical trigger to osteophyte formation, with osteophyte and bone remodelling being viewed as an attempt to stabilise and broaden the compromised joint to better withstand loading forces.12, 13 Chondrocalcinosis due to calcium pyrophosphate crystals has also been suggested to be associated with a tendency to osteophyte formation and a “hypertrophic” form of OA.14 Possibly, therefore, multiple factors may influence osteophyte formation and contribute to the marked heterogeneity of OA.
Assessment of individual radiographic features is the main outcome measure for evaluating structural changes in OA.15, 16 There is little information, however, on the morphology of knee osteophyte seen on radiographs. The present study aimed at (a) describing the size and direction of osteophyte in the OA knees of a group of patients in hospital and (b) assessing possible associations between osteophyte size and other factors visible on standard knee radiographs that may influence osteophyte growth.
PATIENTS AND METHODS
Approval for the study was obtained from the local research ethics committee.
Patients and radiographs
Routine radiographs of patients seen for symptomatic knee OA (new and follow up) over a nine month period in a hospital rheumatology clinic were examined for the study. No patient had coexisting inflammatory arthropathy as determined by clinical inquiry, examination, and limited laboratory and radiographic investigation. Radiographic knee OA was defined as the presence of joint space narrowing and osteophyte in any knee compartment. No radiograph showing patellectomy or joint replacement was included. All radiographs were obtained under standardised conditions and included (a) weightbearing, full extension anteroposterior views (55 kV, 8 mA/s, full scale deflection 100 cm; Kodak film) and (b) skyline 30 degrees flexion views according to the method of Laurin et al (60 kV, 10 mA/s, full scale deflection 100 cm; Kodak film).17
Radiographic assessment
After an initial training period a single observer who was unaware of the patient details examined all the radiographs. For follow up patients with sequential knee radiographs, the earliest available knee films taken within the previous seven years, during which anteroposterior and skyline films were standardised, were used.
Individual radiographic features were separately assessed for the lateral and medial tibiofemoral joints (TFJ) and lateral and medial patellofemoral joints (PFJ). Joint space narrowing for each compartment and osteophyte at each of six sites (lateral and medial femur, lateral and medial tibia, lateral and medial aspect of the patella) were graded 0–3 according to a standard atlas.16 Although not included in any photographic atlas, osteophytes at the lateral and medial femoral trochlea were given a similar 0–3 grading using a line drawing system.18 Osteophyte size was therefore graded at eight sites in each knee. The direction of osteophyte alignment at the eight sites was divided by visual inspection into five categories—upward, upper middle, outward, lower middle, or downwards.
Bone attrition (reduction in normal bone contour) and chondrocalcinosis in the TFJ and PFJ were graded 0–1 (absent/present). Local alignment was assessed for both the TFJ and PFJ. The femorotibial angle, an indicator of varus alignment, was measured on anteroposterior films to the nearest 1° using a protractor.19, 20 Patellar subluxation on skyline films was graded medial 0–1 and lateral 0–3.16
Statistics
To minimise any bias produced by similarity between right and left knees of the same person,21 all analyses were performed for one knee selected at random from each patient. Intraobserver reproducibility was assessed by regrading 50 sets of masked bilateral films three weeks apart in the middle of the study period. Levels of agreement were quantified using the κ statistic,22 and reproducibility of continuous variables assessed according to the method of Bland and Altman.23 Other analyses were performed using Spearman rank correlation or Mann-Whitney test, as appropriate. Odds ratios were calculated according to the presence or absence of grade 1 or more osteophyte or grade 2 or 3 osteophyte using logistic regression. Stepwise logistic regression was used for multivariate analysis (SPSS). Grades of narrowing and patellar lateral subluxation were dichotomised at a cut off point between 0 and 1 and 2 and 3, respectively. Patient demographics (age, sex, body mass index), local narrowing, and any radiographic feature found to associate on univariate analysis were included in the model.
RESULTS
Radiographs of 204 patients (155 women, 49 men; mean age 70, range 34–91 years; median body mass index 28.4, range 19.1–50.8) were included in the study. Radiographs were of reasonable to good standard for contrast and alignment (anterior and posterior margins of the medial tibial plateau were superimposed within 1 mm in 42% of knees). Within the 198 patients with bilateral radiographic OA there was close correlation between x ray findings in right and left knees (ranges for correlation coefficient in different compartments: narrowing 0.55–0.72; osteophyte 0.44–0.62; attrition 0.34–0.59; chondrocalcinosis 0.73–0.81; all p<0.01). Six patients had only one eligible knee, which was therefore selected for study (three unilateral patellectomy, two unilateral OA, one missing film).
Reproducibility
Intraobserver reproducibility of grading (κ statistic) was generally good (joint space narrowing 0.77; osteophyte 0.71; osteophyte direction 0.67; attrition 0.90; chondrocalcinosis 0.66; patellar subluxation 0.80). Reproducibility of measurements for continuous variables (95% limits of agreement) was ±0.8 mm for medial joint space width and ±3° for femorotibial angle.
Direction of osteophyte
Osteophyte occurred at all sites (lateral femur 93; lateral tibia 112; medial femur 101; medial tibia 101; lateral patella 72; lateral femoral trochlea 60; medial patella 68; medial femoral trochlea 67). Various shapes and directions of osteophyte were observed. Figure 1 shows the frequency of the different directions at the eight sites.

Direction of osteophyte at each site among 204 subjects. Size of arrow reflects frequency of direction. Osteophyte was seen in 93 subjects at the lateral femur, 112 at the lateral tibia, 101 at the medial femur, 101 at the medial tibia, 72 at the lateral patella, 60 at the lateral femoral trochlea, 68 at the medial patella, and 67 at the medial femoral trochlea.
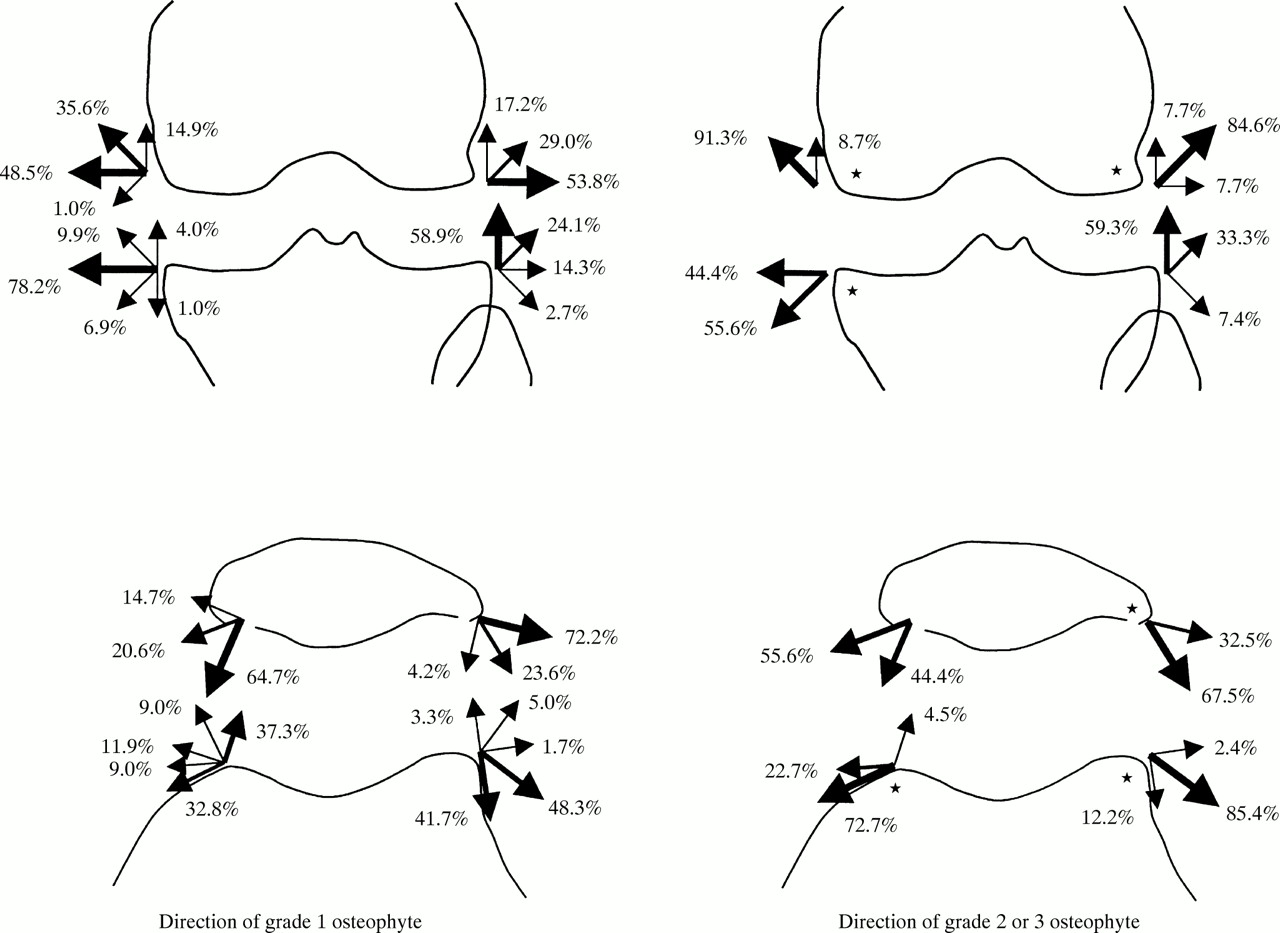
Because numbers in some of the grades for osteophyte and narrowing were small at some sites, these data were dichotomised. The direction of larger (grade 2 or 3) osteophyte differed from that of smaller (grade 1) osteophyte at the following six sites: lateral femur (p=0.004); medial femur (p<0.001); medial tibia (p=0.027); lateral patella (p<0.001); lateral femoral trochlea (p<0.001); and medial femoral trochlea (p=0.022). As seen on the anteroposterior view (fig 2), small osteophytes at the medial femoral, medial tibial, and lateral femoral sites point mainly in a horizontal direction, whereas larger osteophytes at these sites predominantly point vertically away from the joint line. Lateral tibial osteophytes, however, mainly point upwards (or upper middle) towards the joint line, irrespective of size. On the skyline view (fig 2) small medial femoral trochlear osteophytes equally point upwards (into) or downwards (away) from the joint line, but large osteophytes predominantly point downwards; lateral trochlea osteophytes mainly point downwards (away) from the joint line but larger osteophytes point more laterally than small ones. Most small medial patella osteophytes point towards the joint line but larger osteophytes point more laterally than small ones, whereas small lateral patella osteophytes mainly point laterally but large osteophytes point more downwards towards the joint line. At some sites, therefore, osteophyte direction clearly differs for large osteophytes in comparison with small osteophytes.

Comparison of direction of osteophyte between grade 1 osteophyte and grade 2 or 3 osteophyte. * Significance was found between grade 1 and grade 2 or 3 osteophytes.
Similarly, osteophyte direction in knees having marked (grade 2 or 3) local (same compartment) joint space narrowing was significantly different from those with none/mild (grade 0–1) narrowing at the following four sites: lateral femur (p=0.006); lateral tibia (p<0.001); medial femur (p=0.001); and lateral femoral trochlea (p<0.001) (frequencies not shown). At these sites, marked local compartment narrowing was associated with the osteophyte direction of large osteophytes. Osteophyte direction at the lateral tibia was associated with both local (lateral TFJ) and medial TFJ narrowing (fig 3), but not associated with osteophyte size. The osteophyte direction of the medial patella showed no association with either osteophyte size or local narrowing.

{kind=link}
{kind=link}
{kind=link}
Comparison of direction of osteophyte at the lateral tibia between grade 0 or 1 and grade 2 or 3 tibiofemoral narrowing. The direction of osteophyte in grade 2 or 3 narrowing significantly differed from that in grade 0 or 1 narrowing in both lateral (p<0.001) and medial (p<0.001) TFJ. * Significance was found between grade 0 or 1 and 2 or 3 narrowing.
Osteophyte size
Positive correlations were found between grades of osteophyte and grades of local narrowing (that is, the greater the narrowing the larger the osteophyte) in all compartments except the medial PFJ (table 1). At the medial PFJ, however, the size of both patella and medial trochlear osteophytes were positively correlated with medial TFJ narrowing. The size of femoral and tibial osteophytes in the lateral TFJ was also positively correlated with lateral PFJ narrowing.
Correlations between osteophyte grades and joint space narrowing grades in local compartment and the other compartment. Spearman's rank correlation coefficients (rs) are shown
The grade of an osteophyte and that of the counterpart osteophyte in the same compartment were highly correlated at all four sites (correlation coefficients: lateral TFJ=0.56; medial TFJ=0.62; lateral PFJ=0.58; medial PFJ=0.39; all p<0.01). The summated osteophyte score within a compartment was also highly correlated with the summated osteophyte score of the other three compartments (correlation coefficients: lateral TFJ=0.64; medial TFJ=0.48; lateral PFJ=0.45; medial PFJ=0.41; all p<0.01).
Associations of osteophyte grades
On univariate analysis various radiographic features and demographic data were found to be associated with grade 1 or more osteophytes and with grade 2 or 3 osteophytes and so were entered into the logistic regression models for multivariate analysis together with the factors described under methods. Tables 2 and 3 show those factors that remained significant after multivariate analysis.
Odds ratio (OR) and 95% confidence intervals (CI) for factors associated with grade 1 or more osteophyte at each site: multivariate analysis
Odds ratio (OR) and 95% confidence intervals (CI) for factors associated with grade 2 or 3 osteophyte at each site: multivariate analysis
Local narrowing was associated with grade 1 or more osteophyte at most sites. Lateral tibial osteophyte did not associate with local narrowing but did associate with both medial TFJ and lateral PFJ narrowing. Lateral patellar and lateral trochlear osteophytes were associated with patellar lateral subluxation rather than local narrowing. Grade 2 or 3 osteophytes in the medial PFJ did not associate with local narrowing but did with varus alignment (femorotibial angle) and medial TFJ narrowing.
Attrition of the TFJ was associated with grade 2 or 3 osteophytes in both lateral and medial TFJ compartments. Attrition of the PFJ was associated with grade 1 or more osteophytes in the lateral TFJ as well as with grade 2 or 3 osteophytes in the lateral PFJ. Chondrocalcinosis was associated with osteophytes at many sites. With respect to local alignment, lateral patellar subluxation was strongly associated with osteophytes in the lateral PFJ, and femorotibial angle (varus) was associated with grade 2 or 3 osteophyte in the medial TFJ. Summated osteophyte scores were associated with osteophytes at the medial femur and medial femoral trochlea.
DISCUSSION
This is the first study that attempts to describe the detailed radiographic topography of osteophyte at the knee and to determine other radiographic features that may be associated with size and direction of osteophyte. Because radiographic findings were similar in right and left knees, reflecting the symmetry of knee OA, we included for analysis only one knee from each subject to avoid problems of interdependence between knees of the same subject.21 The study shows that at all sites except the lateral tibia and medial patella the direction of an osteophyte alters with size; the narrower the local compartment the more the direction assumes that of large osteophyte. We found associations to support the influence of both local biomechanical and more generalised constitutional factors on osteophyte development. For example, the associations between (a) medial PFJ osteophyte size and medial TFJ narrowing; (b) lateral tibial osteophyte size and both medial TFJ and lateral PFJ narrowing; (c) lateral PFJ osteophyte size and lateral patellar subluxation; and (d) medial TFJ and PFJ osteophyte size and varus malalignment are readily understood in terms of biomechanical stimuli. By contrast, the association between chondrocalcinosis and total osteophyte scores suggests constitutional variation between subjects.
It has been proposed that local instability is an important biomechanical trigger to osteophyte formation.12 In experimental models of OA, osteophyte formation in an unstable joint is promoted by joint movement13 and inhibited by immobilisation.24 Removal of osteophytes during total arthroplasty for knee OA increases instability,7 indicating that osteophyte can stabilise the OA joint. To best achieve this splinting function, osteophyte may need to grow laterally to widen the articular surface.12, 13 Our data support this hypothesis for small osteophytes that predominantly extend outwards. The exception, however, is osteophyte at the lateral tibial plateau that mainly appears as a “traction spur” extending upwards, not outwards, when the medial TFJ is narrowed and the lateral TFJ space is minimally involved. Pottenger et al showed that even such a vertical osteophyte can stabilise the joint,7 presumably by creating a newly raised tibial surface and reducing excessive valgus motion. In contrast with small osteophytes, larger osteophytes predominantly extend upwards or downwards. This may reflect the anatomical limitation to lateral growth imposed by the restraints of adjacent fibrous structures, or the need to widen and strengthen the osteophyte base to protect against fracture.
Osteophyte and cartilage loss are central radiographic features of OA.1, 3 Although osteophyte can occur as an apparently isolated feature associated with age,10 radiographs are relatively insensitive and cannot exclude minor, especially focal, lesions in cartilage and bone. More sensitive imaging techniques show a stronger association between osteophyte and cartilage lesions.25, 26 In experimental models of OA osteophyte formation inevitably accompanies cartilage loss and starts soon after disease induction.11 In a murine model of OA a good correlation has been reported between osteophyte size and cartilage damage.6 In our study a similarly strong association was observed between osteophyte size and local cartilage narrowing, especially in the medial TFJ and lateral PFJ. However, osteophyte size in the lateral TFJ showed a stronger association with narrowing in the medial TFJ and lateral PFJ than in its own compartment, and osteophyte size in the medial PFJ showed no correlation with local narrowing but an association with narrowing in the medial TFJ. It therefore seems that changes in distant as well as local compartments may influence osteophyte size. This could be through either mechanical or biochemical stimuli to growth.4, 5 Mechanical mediation, however, would most probably explain the association of both medial TFJ and PFJ osteophyte size with varus malalignment. van Osch et al speculated that cartilage damage and osteophyte formation are not directly linked but that both are induced by the same factor and develop independently of each other.6 Such independent development may have been observed in the lateral PFJ and medial TFJ, where osteophyte size associates more with lateral patella subluxation and femorotibial angle, respectively, than with local narrowing.
The association at several sites between osteophyte and summated osteophyte scores supports the concept of a constitutional tendency towards osteophytosis and a “hypertrophic” bone response in some subjects.27 Presumably, there may be individual variation in expression or response to growth factors, such as transforming growth factor β4, 28 and bone morphogenic protein-2,5 that plays a part in osteophyte formation. Of further interest in this respect is the association between chondrocalcinosis and summated osteophyte score. Although community surveys have confirmed an association between chondrocalcinosis and OA,29 clinical studies suggest a more specific association between calcium pyrophosphate crystals, the usual cause of chondrocalcinosis, and the hypertrophic end of the OA spectrum.14 In addition to its effect on osteophytosis, transforming growth factor β1 enhances production of extracellular pyrophosphate by chondrocytes,30 and mechanical perturbation of chondrocytes increases the release of ATP, a potent source of extracellular pyrophosphate,31 thereby predisposing to pyrophosphate crystal formation. Such shared chemical and/or mechanical predisposing factors may explain the association between osteophytosis and chondrocalcinosis seen in this study.
There are several important caveats to this work. Although the study group was heterogeneous and not selected on the basis of a particular pattern of OA, all subjects were patients referred to hospital with symptoms and moderate to marked structural changes of knee OA, and our sample size of 204 subjects is relatively small. Different results might be obtained in a larger community based sample that included both symptomatic and asymptomatic subjects. Furthermore, we examined radiographs at just one time for each. Prospective serial data are required to confirm true change in direction of osteophyte with growth. Possibly, variability in positioning and rotation of the knee might have influenced assessment of osteophyte size and alignment. Our knee radiographs, however, showed the expected variability in positioning as assessed by medial tibial plateau alignment32; although such variability may have important effects on assessment of progression of joint space narrowing, it has little effect on assessment of osteophyte.32 Our observations, of course, are necessarily restricted to two dimensional radiographic views and not to a three dimensional image of osteophyte. Nevertheless, despite these reservations, we used standardised weightbearing films, included all three joint compartments in the study, had good reproducibility for all radiographic measures, and found highly significant associations with good face validity.
In summary, this hospital based radiographic study has delineated patterns of osteophyte direction of growth that vary between compartments and according to osteophyte size. Osteophyte size is associated not only with local compartmental narrowing but also with local alignment and bone response. Chondrocalcinosis is associated with increased osteophytosis throughout the joint. Such data support an influence of both local and constitutional factors in determining the size and direction of osteophyte formation in knee OA.
Acknowledgments
We are indebted to the Department of Orthopaedic Surgery of Fukushima School of Medicine for a travelling research grant for Dr Nagaosa, and to the Arthritis Research Campaign for infrastructure support through ICAC grant D0541.