Article Text

Abstract
Background: Achieving clinical remission is the primary target for rheumatoid arthritis (RA) treatment. The SELECT clinical trial program has proven upadacitinib (UPA), a selective Janus kinase inhibitor, to be an effective and safe treatment for rheumatoid arthritis[1-6]. The UPwArds study was designed to provide a deeper understanding of UPA’s real-world effectiveness in daily clinical practice. This post-hoc analysis investigates whether UPA treatment benefits patients by achieving clinical remission and to which extent remission impacts patient-reported outcomes (PROs), reflecting the patient’s perspective on RA.
Objectives: First, to evaluate the effectiveness of UPA regarding the achievement of Clinical Disease Activity Index remission (CDAI) after 6 months of treatment. Second, to investigate whether the results of PROs conveying essential information differ regarding CDAI remission status.
Methods: UPwArds was a post-marketing observational study involving adults with moderate-to-severe RA, characterized by a swollen joint count of 3 or more, with inadequate response to at least one other disease-modifying anti-rheumatic drug (DMARD). This analysis examines if patients reaching CDAI-remission (CDAI ≤ 2.8) after 6 months of UPA treatment also differ in PROs reflecting crucial symptom domains from the patient’s perspective from those not in remission. The chosen PROs were: pain and fatigue on a numerical rating scale (NRS, 0-10), the Patient-Health Questionnaire 9 (PHQ-9) reflecting depressive symptoms, the Funktionsfragebogen Hannover (converted into internationally used Health Assessment Questionnaire-Disability Index (HAQ-DI))[7] assessing physical function, and the duration of morning stiffness. Data were analyzed as observed without imputation of missing values.
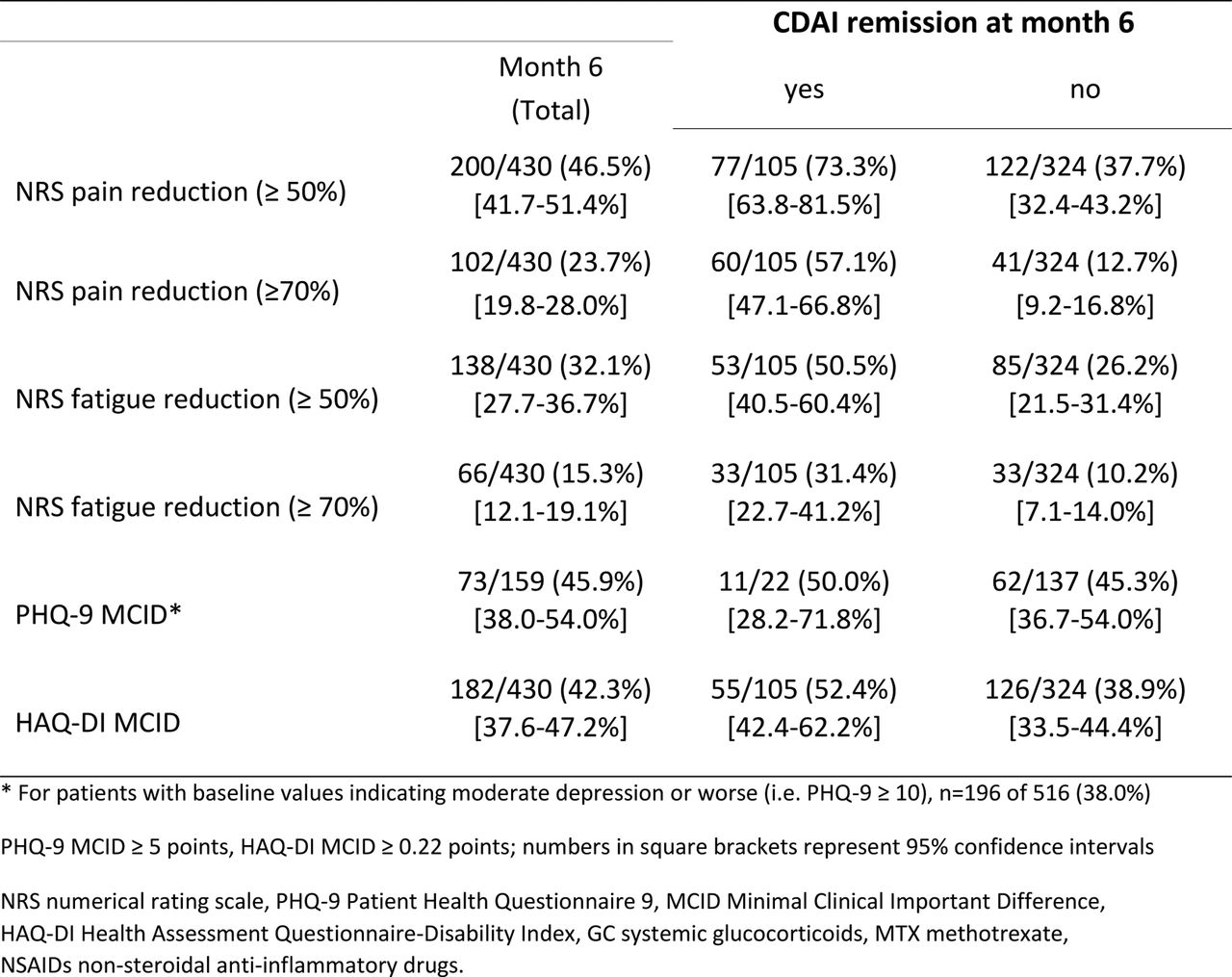
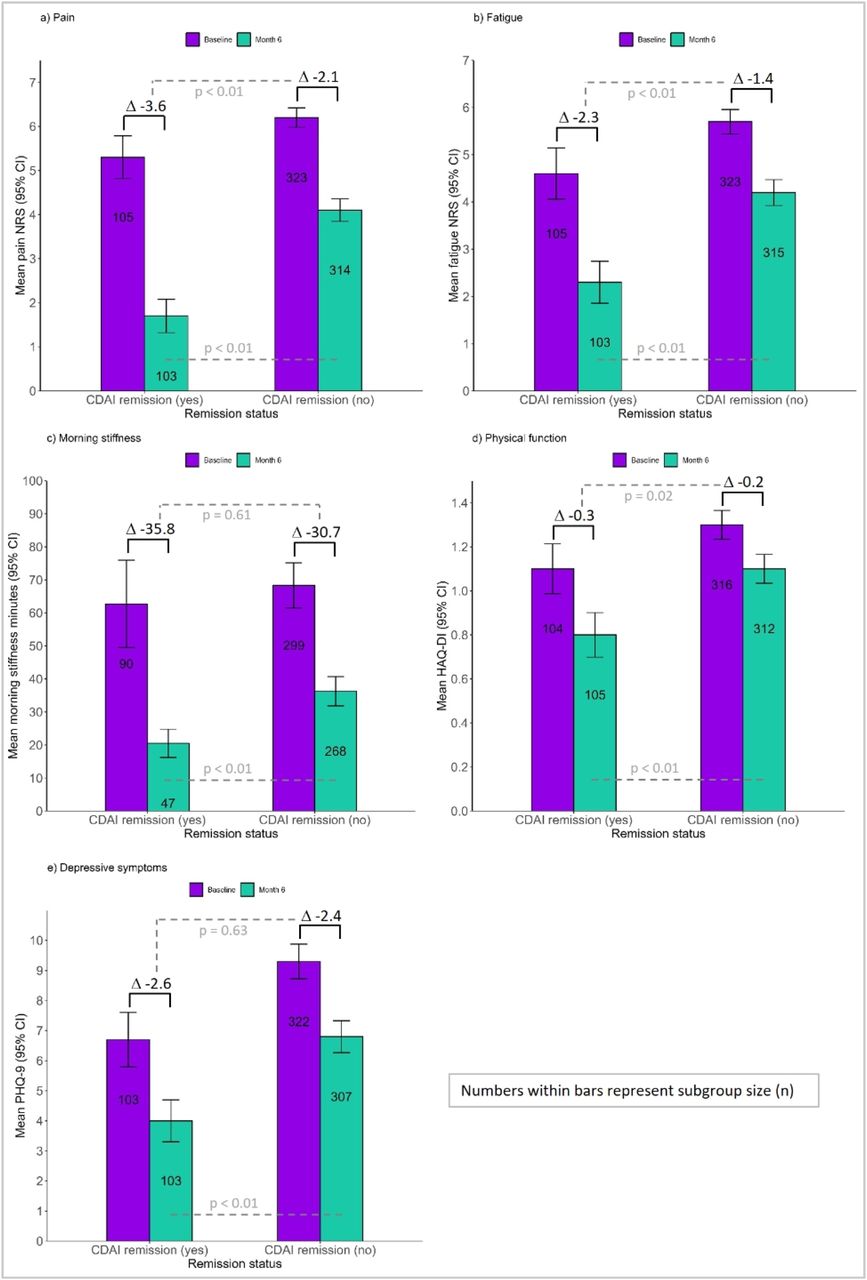
Results: The population for this post-hoc analysis included 516 patients with baseline data and at least one dose of upadacitinib. In total, 76.4% of patients were female and had a corresponding mean disease duration of 9.0 years; 105 of 430 remaining patients (24.4%) achieved CDAI-remission at 6 months, with comparable baseline CDAI scores for those patients, achieving remission, and those who were not in remission at 6 months (23.7 and 24.9). Patients in CDAI remission showed significant improvements in pain and fatigue compared to those not in remission (Figure 1a and b), which was also confirmed for categorized improvements (Table 1). Mean score improvements for PHQ-9 and the duration of morning stiffness were not different when compared between the two patient groups (Figure 1c and e). MCIDs for the PHQ-9 and the HAQ-DI showed similar improvements independent from remission status (Table 1). However, mean HAQ-DI improvements were greater for patients in remission whose month-6 absolute scores were better throughout all PROs compared to patients not achieving remission (Figure 1). Safety data for UPA during UPwArds have been previously reported[8].
Conclusion: In RA patients having previously failed at least one other DMARD treatment, approximately 1 in 4 patients achieved CDAI remission with UPA treatment at month 6. Patients achieving remission were more likely to experience greater improvements in pain, fatigue, and physical function compared to those not in remission.
REFERENCES: [1] Smolen JS, et al. Lancet 2019;393:2303–11;
[2] Burmester GR, et al. Lancet 2018;391:2503–12;
[3] Genovese MC, et al. Lancet 2018;391:2513–24;
[4] van Vollenhoven R, et al. Arthritis Rheumatol 2020;72:1607–20;
[5] Fleischmann R, et al. Arthritis Rheumatol 2019;71:1788–800;
[6] Rubbert-Roth A, et al. N Engl J Med 2020;383:1511–21;
[7] Lautenschläger J et al. Z. Rheumatol. 1997;56(3):144-55
[8] Witte T, et al. Ann Rheum Dis 2023;82:718-719 (https://doi.org/10.1136/annrheumdis-2023-eular.1202)


{kind=link}
{kind=link}
Mean baseline and month-6 scores stratified by CDAI remission at month 6
Acknowledgements: AbbVie funded this study, contributed to its design, participated in data collection, analysis and interpretation of data, and in writing, review, and approval of the abstract. AbbVie and the authors thank all study investigators for their contributions and all patients that participated in this study. No honoraria or payments were made for authorship. Statistical analysis support was provided by StatConsult, which was funded by AbbVie. Medical writing support was provided by Dr. Matthias Englbrecht and was funded by AbbVie.
Disclosure of Interests: Torsten Witte Grant/research support from: AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Chugai, Gilead, Janssen, Lilly, MSD, Mylan, Novartis, Pfizer, Roche, and UCB, Uta Kiltz Consultant of: AbbVie, Biocad, Eli Lilly and Company, Grünenthal, Hexal, Janssen, MSD, Novartis, Pfizer, Roche, and UCB, Grant/research support from: AbbVie, Amgen, Biogen, Fresenius, GSK, Hexal, Novartis, and Pfizer, Florian Haas Consultant of: AbbVie, Celgene, Novartis, and Pfizer, Grant/research support from: AbbVie, BMS, Celgene, Chugai, MSD, Novartis, Pfizer, Roche, and Sanofi Genzyme, Elke Riechers Consultant of: AbbVie, Chugai, Novartis, and UCB, Grant/research support from: AbbVie, Chugai, Lilly, Janssen, Novartis, Pfizer, Roche, and UCB, Daniela Adolf Employee of StatConsult, Ulrich Prothmann Grant/research support from: AbbVie, Amgen, Bristol-Myers Squibb, Chugai, Glaxo Smith Kline, Novartis, Pfizer, Roche, Sanofi, SOBI, and UCB, Kirsten Famulla Employee of AbbVie and may own stock or options, Alexander Rössler Employee of AbbVie and may own stock or options, Konrad Götz Employee of AbbVie and may own stock or options, Klaus Krüger Grant/research support from: AbbVie, Biogen, BMS, Celltrion, Gilead, Hexal, Janssen, Lilly, Medac, MSD, Novartis, Pfizer, Roche, and UCB.
- Patient Reported Outcome Measures
- Remission
- Real-world evidence
- Targeted synthetic drugs