Article Text

Abstract
Objectives To investigate the associations of residential greenness with bone mineral density and incident osteoporosis, and further evaluate the potential modifying effect of genetic susceptibility.
Methods We used the Normalised Difference Vegetation Index (NDVI) at various buffer distances, including 300 m (NDVI300m), 500 m (NDVI500m), 1000 m (NDVI1000m) and 1500 m (NDVI1500m), to serve as indicators of greenness. We fitted linear regression, logistic regression and Cox proportional hazard models to assess the associations of residential greenness with estimated bone mineral density (eBMD), prevalent osteoporosis and incident osteoporosis, respectively. With the Polygenic Risk Score (PRS) for osteoporosis, we further assessed the joint effects of genetic risk and greenness on the risk of osteoporosis. We conducted causal mediation analyses to explore potential mediators.
Results Each IQR increase in NDVI300m was associated with 0.0007 (95% CI 0.0002 to 0.0013) increase in eBMD, 6% lower risk of prevalent osteoporosis (OR 0.94; 95% CI 0.92 to 0.97) and 5% lower risk of incident osteoporosis (HR 0.95; 95% CI 0.93 to 0.98). The joint effects of greenness and PRS on the risk of osteoporosis displayed a clear dose-response pattern. Compared with individuals exposed to low NDVI levels and high genetic risk, those exposed to high NDVI levels and low genetic risk had a 56% (95% CI 51% to 61%) lower risk of osteoporosis. The primary mediators in the association between greenness and incident osteoporosis were identified as PM2.5 and NO2.
Conclusions Residential greenness was associated with higher bone mineral density and decreased risk of incident osteoporosis.
- polymorphism, genetic
- osteoporosis
- epidemiology
- bone density
Data availability statement
Data are available upon reasonable request. The data used in this current study are available from the UK Biobank data resources. Permissions are required in order to gain access to the UK Biobank data resources, subject to successful registration and application process. Further information can be found on the UK Biobank website (https://www.ukbiobank.ac.uk/).
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Osteoporosis is a complex disease caused by both genetic and environmental factors.
The presence of green spaces has been linked to decreased risk of negative outcomes. However, no research has been conducted to prospectively investigate the effects of exposure to green spaces on incident osteoporosis.
To date, no research has explored the interplay between genetic susceptibility and exposure to greenness in relation to the risk of osteoporosis, as well as the combined effects of these factors.
WHAT THIS STUDY ADDS
The findings from this study present the first evidence indicating that residential greenness is associated with higher bone mineral density and a decreased risk of developing osteoporosis.
Compared with individuals with low genetic risk, those with intermediate or high genetic risk had a 48% or 117% elevated risk of developing osteoporosis, respectively.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings provide valuable insights into the potential of greenness in preventing the onset of osteoporosis and emphasise the significance of urban greening in developing effective prevention strategies.
The presence of green spaces has been linked to decreased risk of negative outcomes. However, no research has been conducted to prospectively investigate the effects of exposure to green spaces on incident osteoporosis.
Introduction
Osteoporosis, the most prevalent metabolic bone disorder, is characterised by the deterioration of bone microarchitecture and reduced bone density.1 With the global rise in life expectancy and changing lifestyles, osteoporosis is becoming a significant health issue in many parts of the world.2 Osteoporosis can lead to serious consequences, such as fractures, chronic pain, diminished mobility and decreased quality of life, imposing significant social and economic burdens.3 The estimated direct annual cost of treating osteoporotic fractures in Europe, Canada and the USA alone is between US$5000 million and US$6500 million on average.3 Efforts are underway to raise awareness about osteoporosis, promote early detection and implement preventive measures to reduce the burden of osteoporosis on individuals and healthcare systems globally.4
An increasing number of studies are focusing on the role of environmental factors in the development of osteoporosis. Previous studies have indicated that ambient air pollution exposure was linked to an elevated risk of osteoporosis.5 6 These findings provide inspiration for how enhancing environmental conditions can potentially mitigate the adverse effects of these hazards, thereby aiding in the prevention of osteoporosis. Meanwhile, the presence of green spaces, a significant factor in promoting health in urban environments, has been linked to decreased risk of negative outcomes, such as overall mortality, cardiorespiratory diseases and mental illness.7–10 These associations are thought to be mediated through potential psychosocial pathways, as green spaces mitigate air pollution harm, alleviate psychological stress and promote exercise.11 12 These factors have the potential to contribute to a reduced risk of osteoporosis. So far, the investigation of the effects of greenness on bone health has been limited to three studies, yielding inconclusive results.13–15 No research has been conducted to prospectively investigate the effects of exposure to green spaces on incident osteoporosis.
Osteoporosis is a multifactorial condition influenced by both genetic and environmental risk factors. A growing body of evidence has indicated that genetics also play a significant role in the development of osteoporosis.16 Genome-wide association studies (GWASs) have achieved significant success in identifying the genetic predisposition to osteoporosis.17 18 Emerging research findings proposed that genetic susceptibility has the potential to influence the effects of environmental factors on human health.19–22 The interplay between genes and the environment is a complex area of research that seeks to understand how genetic variations interact with external factors to influence an individual’s health. To date, no research has explored the interplay between genetic susceptibility and exposure to greenness in relation to the risk of osteoporosis, as well as the combined effects of these factors.
In the present study, we investigated the associations of long-term exposure to greenness with bone mineral density (BMD) and the risk of osteoporosis using a large cohort. Additionally, we explored the combined effect of greenness and genetic susceptibility on the incident osteoporosis.
Materials and methods
Study population
For the current study, data were obtained from the UK Biobank. In this cohort, more than half a million individuals aged 40–69 years were recruited throughout the country at baseline (2006–2010). At the assessment centre, participants reported their information regarding demographics, socioeconomic status and lifestyle. In addition, they underwent physical examinations and consented to be followed up through record linkage. Informed consent was provided by each participant. Further information regarding this cohort can be found at http://www.ukbiobank.ac.uk/.
Based on 502 482 individuals initially enrolled in the UK Biobank, we excluded 5154 participants who have missing data on greenness exposure. We also excluded those with incomplete data on BMD (n=15 346) and important covariates (n=90 684). Accordingly, 391 298 participants were included in the main analyses (figure 1).

Flowchart of selection process. eBMD, estimated bone mineral density; OP, osteoporosis; PRS, Polygenic Risk Score.
Residential greenness
Normalised Difference Vegetation Index (NDVI) was employed as an indicator of residential greenness,23 an indicator reflecting the difference in spectral reflectance between visible read (absorbed by chlorophyll in plants) and near-infrared regions (reflected by internal structure of leaves) to the sum of the two. The equation is given as: NDVI=(Near infrared−Red)/(Near infrared+Red). In general, the index lies in the range of −1 to +1, where a larger value represents more green cover. Data for this study were obtained from the 250-metre resolution, 16-day composite remote sensing product from MODIS satellite (https://modis.gsfc.nasa.gov/data/). To prevent temporal mismatch, summer-time images of the study area during baseline were captured, then processed using quality control parameters to remove cloudy and snowy pixels. We restricted NDVI values to greater than 0 to avoid effects of water bodies. Finally, NDVI values were averaged within a buffer region of 300, 500, 1000 and 1500 m around participants’ residence, following national recommendations of UK (300 m)24 and previous studies.25 26
Outcome assessment
Estimated bone mineral density (eBMD) was measured using Sahara heel ultrasound device (Hologic, USA). BMD (g/cm2) was calculated by combining the speed of sound (SOS, in m/s) and bone ultrasound attenuation (BUA, in dB/MHz), with the equation as eBMD=(SOS+BUA)*0.002592–3.687.27 Additionally, T-scores indicated the difference between an individual’s BMD to that of healthy adults in the same gender, namely, the number of SD between one’s measured value and the standard. Prevalent osteoporosis was defined as T-score ≤−2.5.1 Detailed information on assessment procedure and quality control was available at https://biobank.ndph.ox.ac.uk/showcase/refer.cgi?id=100248.
Incident osteoporosis events during follow-up were confirmed based on self-reports and medical records covering hospital inpatient, primary care and death registry data, consistent with previous UK Biobank studies.28 29 Self-reported diagnoses were collected through a verbal interview. Data on hospital inpatient records were collected through linkage to Health Episode Statistics and the Scottish Morbidity Records. Data on primary care were gathered from a series of general practice records in the UK. Data on Death registration was from the National Health Service Information Center and the National Health Service Central Register Scotland. Osteoporosis cases were identified by the International Classification of Diseases Tenth Revisions (M80-M82). To enhance the accuracy of diagnosis for incident osteoporosis, we excluded those with prevalent osteoporosis at baseline (n=11 875). Participants were followed up until osteoporosis event, death or 31 March 2021.
Polygenic Risk Score
The UK Biobank’s genotyping process and quality control has been documented elsewhere.30 The Polygenic Risk Score (PRS) of osteoporosis in the current study was from the UK Biobank PRS Release in the UK Biobank’s Research Access Platform (May 2022). Bayesian analysis was used to generate the score based on meta-analyses of summary statistics from external GWASs (standard PRS). Calculation of PRS was conducted by multiplying the genome-wide sum of the per-variant posterior effect size by allele dosage. Detailed information regarding the methods was available via https://biobank.ndph.ox.ac.uk/showcase/refer.cgi?id=5202. We further categorised the PRS into tertiles (low, medium and high genetic risk).
Covariates
We considered age, gender, ethnicity, annual household income, education level, employment status, residential area, alcohol consumption, smoking status and healthy diet score as potential confounders. Data on these variables were collected through self-report questionnaires. Among them, residential area (urban or rural) was derived by matching participants’ postcode of residence with data from the Office of National Statistics to account for spatial confounding. Other information was collected through self-report questionnaires. Ethnicity was divided into six categories (white, mixed, Asian, black, Chinese or others). Socioeconomic indicators, including annual household income, education level and employment status, were categorised into five (<£18 000, £18 000–30 999, £31 000–51 999, £52 000–100 000 or >£100 000), seven (college or university degree, A/AS levels, O levels/General Certificate of Secondary Education, Certificate of Secondary Education, Higher National Certificate or Higher National Diploma or National Vocational Qualification, other qualifications or none of these above) and three (employed, retired or unemployed) categories, respectively. Alcohol consumption and smoking status were classified as never, former or current drinker/smoker. The healthy diet score was constructed based on recommendations for health-promoting diets,31 including the following factors: refined grains: ≤1.5 servings daily; whole grains: ≥3 servings daily; vegetables: ≥3 servings daily; fruits: ≥3 servings daily; unprocessed red meat: ≤1.5 servings weekly; processed meat: ≤1 servings weekly; fish: ≥2 servings weekly. For every healthy factor, one point was added, and the score ranged from 0 to 7.
Using land use regression models, the annual average exposures to NO2 and PM2.5 were estimated based on the ESCAPE project. Details are provided in online supplemental material text S1. Physical activity was divided into regular/not regular, with the former category defined as sustaining vigorous exercise ≥75 min/week or moderate exercise for ≥150 min/week (or an equivalent combination), or moderate exercise ≥5 days/week or vigorous exercise ≥1 day/week.32 As an indicator of mental health, the neuroticism score was calculated using the Eysenck Personality Questionnaire–Revised Short Form33 (online supplemental material text S2).
Supplemental material
Statistical analyses
R (V.4.2.1) and SAS (V.9.4; SAS Institute) were implemented throughout our study. All p values were two-sided. P value under the threshold of 0.05 was defined as statistically significant. Demographics were presented as counts (proportions) for categorical variables and means (SD) for continuous variables. Missing indicators were substituted for missing variables (all categorical).
First, we employed a linear regression model to assess the association between residential greenness and eBMD, and a logistic regression model to evaluate the association between residential greenness and prevalent osteoporosis. Furthermore, we implemented Cox proportional hazard models to assess the HRs and 95% CIs for the association between residential greenness and incident osteoporosis. Several confounders were incorporated, namely, age, gender, ethnicity, annual household income, education level, employment status, residential area, alcohol consumption, smoking status and healthy diet score. We confirmed the proportional hazards assumption using Schoenfeld residuals. Non-linearity was assessed using restricted cubic spline (RCS) models.
To evaluate the mediating roles of PM2.5, NO2, physical activity and neuroticism score, causal mediation analyses were conducted using PROC CAUCALMED in SAS V.9.4.34 We examined the four mediators one at a time, in four different mediation models. Detailed information on the statistical method is provided in online supplemental material text S3.
For genetic analyses, we excluded participants with missing data on PRS (n=8533) and those who failed to pass genotyping quality control filter (n=91), then restricted the analyses to participants of European descent (excluded n=30 680). We repeated the analyses of Cox models separately for PRS categories, as well as assessed the joint effect of NDVI300m and PRS at different levels. These analyses further adjusted for genotyping batch and the first 10 genetic principal components.
Several sensitivity analyses were conducted to test the robustness of the results: (1) employing multiple imputation method to repair missing data on covariates (online supplemental material text S4); (2) excluding those with osteopenia condition (ie, T-score less than −1) at recruitment; (3) excluding participants with incident osteoporosis at first 2 years of follow-up; (4) restricting analyses to those who have lived in the current address for at least 5 years; (5) employing NDVI within larger buffers (500, 1000 and 1500 m) as greenness indicators; (6) employing land use indicators as proxies for greenness exposure (online supplemental material text S5); (7) employing greenness exposure as time-varying variables in the models to account for levels of exposure during follow-up (online supplemental material text S6); (8) further adjusted for medical conditions, including BMI, vascular/heart problems (including hypertension, stroke, angina and heart attack), and diabetes; (9) further adjusted for vitamin (A, B, C, D, E, B9 or multivitamin)/mineral (fish oil, glucosamine, calcium, zinc, iron or selenium) supplements intake; (10) further adjusted for time spend outdoors in summer and winter35 ; (11) only considering diagnosis with medical records (excluding self-reported diagnosis).
Results
Online supplemental table S1 displays a demographic comparison between the study population and the full sample of the UK Biobank, revealing that they exhibited a high degree of comparability. The baseline characteristics of participants, stratified by prevalent/incident osteoporosis, are presented in table 1. The mean age (SD) of the 391 298 participants was 56.2 (8.1), with 53.0% of them being female. Following a median follow-up period of 12.07 years (and the mean follow-up period was 11.77 years), a total of 9307 incident osteoporosis cases were identified. Patients with osteoporosis exhibited characteristics such as advanced age, female gender, retired status and smoking habits. Furthermore, they were more inclined to experience economic disadvantage and possess lower levels of education. Online supplemental table S2 presents the distribution of greenness exposures. The median value for NDVI300m was 0.57, with the lower and upper quartiles being 0.51 and 0.64, respectively.
Baseline characteristics of participants stratified by prevalent/incident osteoporosis status
Table 2 illustrates the associations between residential greenness and eBMD and prevalent osteoporosis at baseline. After full adjustment, per IQR increment of NDVI300m was associated with 0.0007 (0.0002, 0.0013) increase in eBMD. We also observed significant associations between residential greenness and prevalent osteoporosis at baseline (table 2). Each IQR increase in NDVI300m was related to 6% lower risk of prevalent osteoporosis (OR 0.94; 95% CI 0.92 to 0.97). Participants exposed to higher quartiles of NDVI categories exhibited a lower risk of osteoporosis compared with those exposed to the lowest quartile (p for trend=0.001).
Linear regression for the association between residential greenness and estimated bone mineral density, and logistic regression for the association between residential greenness and prevalent osteoporosis at baseline
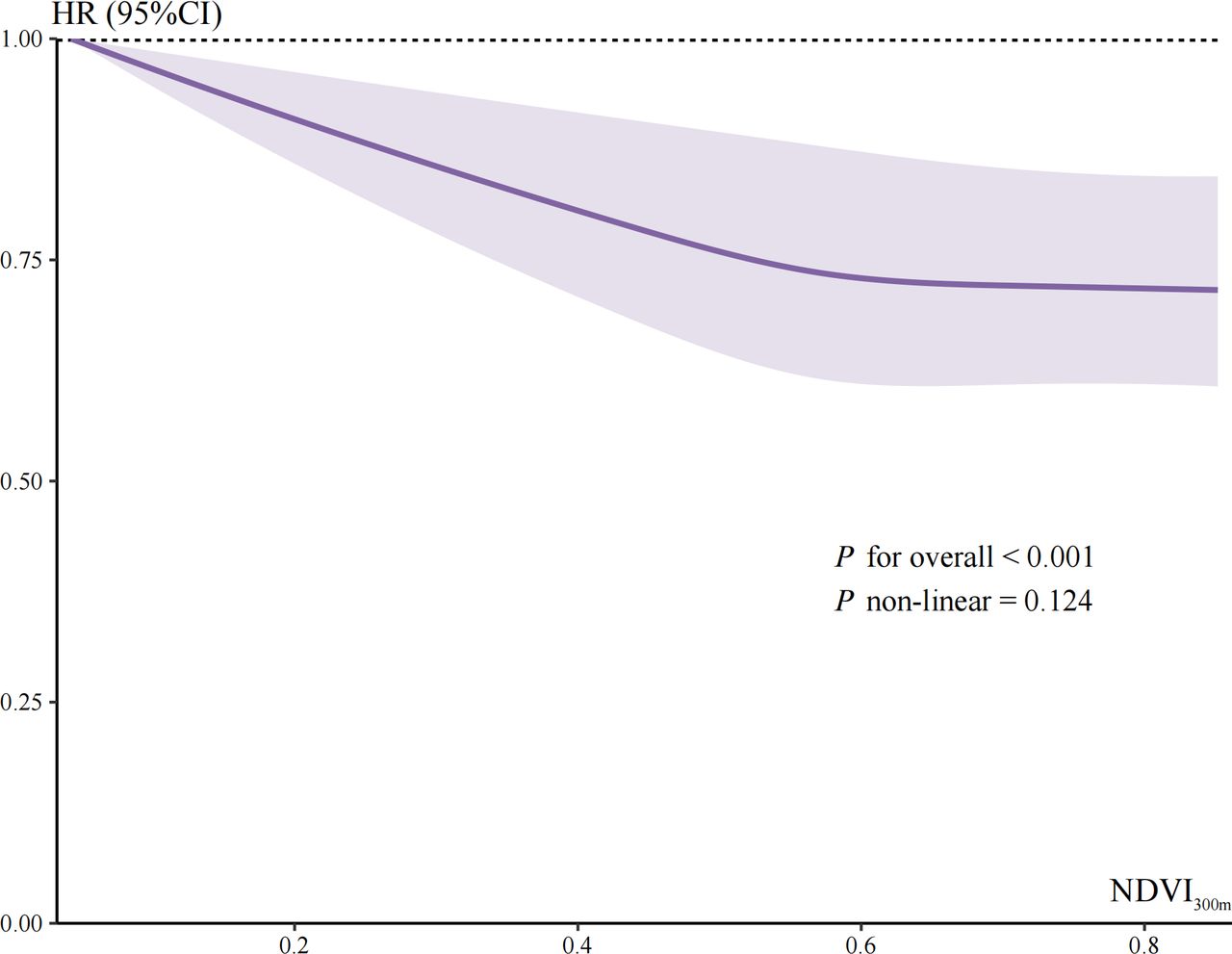
The RCS analysis demonstrates a monotone association between greenness and the incidence of osteoporosis (figure 2). Table 3 depicts the association between residential greenness and incident osteoporosis. In the fully adjusted model, for each IQR increase in NDVI300m, the HR (95 % CI) was 0.95 (0.93 to 0.98). Participants in quartiles 2 (0.94; 0.89 to 1.00), 3 (0.92; 0.86 to 0.97) and 4 (0.92; 0.87 to 0.97) exhibited a decreased risk of developing osteoporosis compared with those in quartile 1. The sensitivity analyses confirmed the robustness of the results (online supplemental tables S1–S13). We consistently observed associations between NDVI within larger buffers (500, 1000 and 1500 m) and incident osteoporosis (online supplemental table S7). Additionally, we found consistent associations between the percentage of greenspace, domestic gardens, and natural environment and the incidence of osteoporosis (online supplemental table S8). Employing greenness exposure as time-varying variables in the models had minimal influence on the results (online supplemental table S9).

Restricted cubic spline of the association between residential greenness and incident osteoporosis. The models were constructed based on Cox regression models with time to incident osteoporosis as dependent variable. NDVI300m was modelled using restricted cubic splines. NDVI300m, Normalised Difference Vegetation Index within 300 m buffer.
Cox regression for the associations between residential greenness and incident osteoporosis
Online supplemental table S14 displays the association between PRS and incident osteoporosis. Compared with individuals with low genetic risk, those with intermediate or high genetic risk had a 48% (95% CI 39% to 57%) or 117% (95% CI 105% to 130%) elevated risk of developing osteoporosis, respectively. Online supplemental table S15 presents associations between residential greenness and incident osteoporosis, separately for PRS categories. We observed a significant association between NDVI as a continuous variable and the occurrence of osteoporosis only in the low genetic risk group. We assessed the combined impact of greenness and PRS on the risk of osteoporosis (figure 3). The joint effects of greenness and PRS on the risk of osteoporosis followed a dose-response pattern. Individuals exposed to high NDVI levels and low genetic risk were associated with a 56% (95% CI 51% to 61%) reduction in the risk of osteoporosis compared with those exposed to low NDVI levels and high genetic risk.

{kind=link}
{kind=link}
{kind=link}
Joint effects of residential greenness and PRS on the risk of incident osteoporosis. The models were constructed based on Cox regression with time to incident osteoporosis as dependent variable. The first group (high genetic risk and first quartile of NDVI300m) was the reference category. Models were adjusted for age, gender, ethnicity, annual household income, education level, employment status, residential area, smoking status, alcohol consumption, healthy diet score, the first 10 genetic principal components and genotyping batch. Ranges for quartile NDVI300m: quartile 1, 0.01–0.51; quartile 2, 0.51–0.57; quartile 3, 0.57–0.64; quartile 4: 0.64–0.86. Ranges for tertile PRS: low, −8.72 to −0.46; medium, −0.46 to 0.34; high, 0.34 to 4.72. NDVI300m, NDVI300m, Normalised Difference Vegetation Index within 300 m buffer; PRS, Polygenic Risk Score; Ref., reference.
Table 4 displays the results of the mediation analysis examining the association between greenness and the incidence of osteoporosis. PM2.5 and NO2 emerged as the primary mediators, accounting for approximately 88.5% and 84.5% of the mediation effect, respectively. Physical activity and neuroticism score were also identified as mediators but had relatively small proportions in mediating the association.
Mediation analysis on the association between residential greenness (NDVI300m) and incident osteoporosis
Discussion
To our knowledge, this is the first cohort study to investigate the association between greenness and incident osteoporosis risk. We observed that higher residential exposure to greenness was independently associated with higher eBMD and decreased risk of incident osteoporosis. We also observed consistent positive associations between the percentage of greenspace, domestic gardens, and natural environment and the incidence of osteoporosis. The association between greenness and osteoporosis was found to be partially mediated by air pollution (specifically PM2.5 and NO2), physical activity and neuroticism score. We also explored the joint effect of greenness and genetic susceptibility on the osteoporosis risk, observing a notable dose-response association. The impacts of greenness on osteoporosis appeared to be more evident in individuals with low genetic risk.
To date, a limited number of population-based studies have examined the effects of greenness on bone health, and the findings from these studies have been inconclusive and contradictory. In a cross-sectional study conducted in China, the quantitative ultrasound index was used as an indicator of bone strength. The study found a positive association between residential greenness and higher bone strength.15 On the contrary, a separate study involving elderly individuals from Hong Kong observed that higher levels of green space were linked to a slower increase in lumbar spine BMD and an elevated risk of incident fracture.14 However, no significant associations were observed regarding BMD changes in the total hip, femoral neck and whole body.14 Another Hong Kong study conducted among the senior population revealed empirical evidence that planned greenspace, as opposed to natural greenspace, exhibited a negative association with osteoporosis.13 However, in empirical studies, determining the temporal sequence can often be challenging because the identification of exposure and outcome takes place at a single time point. Our study employed a large nationwide prospective cohort study to examine the association between residential greenness and bone health. The findings from this study present the first evidence indicating that residential greenness is associated with higher BMD and a decreased risk of developing osteoporosis.
Our study offers valuable novel understanding regarding the biological processes that underlie the impact of exposure to residential greenness on osteoporosis risk. Based on mediation analyses, a significant portion of the association between greenness and osteoporosis can be attributed to the mediating factor of air pollution. This finding aligns with previous evidence indicating that areas with greater greenness tend to experience vegetation-related mitigation of particulate matter levels.36 Several studies have demonstrated that chronic air pollution exposure can disrupt the equilibrium of bone homeostasis through various mechanisms, such as oxidative stress, systemic inflammation, vitamin D deficiency and endocrine disruption.37 38 These factors collectively contribute to an increased risk of osteoporosis.5 6 Additionally, a significant yet small mediating pathway through physical activity was identified. Individuals residing in areas with higher residential greenness had increased opportunities for engaging in physical activity.39 Evidence suggests that physical activity is likely to have a role in the prevention of osteoporosis.40
Our study possesses several notable strengths. First, our study analysed a large sample of adults from a nationwide prospective cohort, first providing novel epidemiological evidence for the longitudinal association between greenness and osteoporosis risk. Second, we investigated the underlying mechanisms by which air pollution and physical activity act as mediators in the association between greenness and osteoporosis. This analysis enhances our understanding of the complex pathways involved in this association. Third, our study involved the calculation of the PRS for osteoporosis, allowing us to examine the potential modifying effect of genetic susceptibility. Recent research indicates that genetic susceptibility holds the potential to exert influence over the impact of environmental factors on human health.19–22 Nevertheless, there is currently limited knowledge regarding the potential genetic modifications that may influence the health effects of greenness. This analysis provides valuable insights into how genetic factors may interact with greenness exposure in influencing the risk of osteoporosis. Lastly, our study employed multiple rigorous sensitivity analyses to ensure the robustness of our results.
However, this study also has several limitations. First, the NDVI calculation was based on the residential addresses of the participants, which means that the actual level of exposure could be either higher or lower than estimated. Second, for the cross-sectional analyses, the use of NDVI at baseline as the exposure variable may introduce exposure misclassification. Third, even after extensively adjusting for covariates, there is a possibility of unmeasured or unknown factors still being present. Fourth, due to the fact that participants in the UK Biobank were voluntary and generally healthy individuals, it was not possible to completely eliminate the potential for selection bias. Fifth, although not the gold standard method for measuring BMD, heel ultrasound has been shown to correlate strongly with dual energy X-ray absorptiometry and is a valid technique in epidemiological studies.41
In this prospective cohort study, we discovered a positive association between residential greenness and increased bone strength, as well as a decreased risk of developing osteoporosis. This association can be attributed primarily to the beneficial impact of green environments in mitigating air pollution. These findings provide valuable insights into the potential of greenness in preventing the onset of osteoporosis and emphasise the significance of urban greening in developing effective prevention strategies.
Data availability statement
Data are available upon reasonable request. The data used in this current study are available from the UK Biobank data resources. Permissions are required in order to gain access to the UK Biobank data resources, subject to successful registration and application process. Further information can be found on the UK Biobank website (https://www.ukbiobank.ac.uk/).
Ethics statements
Patient consent for publication
Ethics approval
The ethics approval was authorised by the North West Multicenter Research Ethics Committee (reference no. 16/NW/0274). All participants provided informed consent to participate. The current study was performed under the UK Biobank application number 69741. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We gratefully thank all staff and participants at the UK Biobank for their contributions to the present study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
TT and LT contributed equally.
YT and ZO contributed equally.
Contributors YT and ZO conceived and designed the study. TT and LT prepared the data. TT, LT, XG and TL conducted the data analysis, performed interpretation of the results and drafted the manuscript. YT, ZO, TT and LT made critical revisions. All authors agreed on the final version of the manuscript and take responsibility for its content. ZO accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish. ZO is responsible for the overall content as the guarantor.
Funding This research is funded by the National Natural Science Foundation of China, grant numbers 82000849 and 82371600; the Natural Science Foundation of Hunan Province, grant numbers 2021JJ30930 and 2021JJ40810; the Natural Science Foundation of Hunan Province of Outstanding Young Scholars, grant number 2021JJ20086; the Scientific Research Projects of the Health Commission of Hunan Province, project number B202304077119; and the Degree & Postgraduate Education Reform Project of Central South University, grant number 2023JGB066.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.