Article Text

Abstract
Objective Early diagnosis of knee osteoarthritis (KOA) in asymptomatic stages is essential for the timely management of patients using preventative strategies. We develop and validate a prognostic model useful for predicting the incidence of radiographic KOA (rKOA) in non-radiographic osteoarthritic subjects and stratify individuals at high risk of developing the disease.
Methods Subjects without radiographic signs of KOA according to the Kellgren and Lawrence (KL) classification scale (KL=0 in both knees) were enrolled in the OA initiative (OAI) cohort and the Prospective Cohort of A Coruña (PROCOAC). Prognostic models were developed to predict rKOA incidence during a 96-month follow-up period among OAI participants based on clinical variables and serum levels of the candidate protein biomarkers APOA1, APOA4, ZA2G and A2AP. The predictive capability of the biomarkers was assessed based on area under the curve (AUC), and internal validation was performed to correct for overfitting. A nomogram was plotted based on the regression parameters. Model performance was externally validated in the PROCOAC.
Results 282 participants from the OAI were included in the development dataset. The model built with demographic, anthropometric and clinical data (age, sex, body mass index and WOMAC pain score) showed an AUC=0.702 for predicting rKOA incidence during the follow-up. The inclusion of ZA2G, A2AP and APOA1 data significantly improved the model’s sensitivity and predictive performance (AUC=0.831). The simplest model, including only clinical covariates and ZA2G and A2AP serum levels, achieved an AUC=0.826. Both models were internally cross-validated. Predictive performance was externally validated in an independent dataset of 100 individuals from the PROCOAC (AUC=0.713).
Conclusion A novel prognostic model based on common clinical variables and protein biomarkers was developed and externally validated to predict rKOA incidence over a 96-month period in individuals without any radiographic signs of disease. The resulting nomogram is a useful tool for stratifying high-risk populations and could potentially lead to personalised medicine strategies for treating OA.
- Knee Osteoarthritis
- Incidence
- Outcome Assessment, Health Care
- Chondrocytes
- Osteoarthritis
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Knee osteoarthritis (KOA) is one of the most prevalent rheumatic diseases ranked in the top 10 causes of chronic disability with a huge impact on public burden.
The inability to detect early disease stages and the lack of effective treatments leave KOA patients without non-surgical clinical options.
A major research interest is focused on discovering prognostic markers to identify individuals at high risk for developing KOA before the joint damage appears.
WHAT THIS STUDY ADDS
A prognostic model based on clinical data and three protein biomarkers was developed and externally validated to predict the incidence of radiographic KOA in individuals without any radiographic signs of the disease, with an area under the curve of 0.83.
The nomogram based on this prognostic model may be warranted in routine clinical practice to identify individuals at a higher risk of developing KOA.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This nomogram for KOA incidence is a useful tool for stratifying high-risk populations in order to prevent disease onset or delay its progression, and thereby decrease the associated burden. The prognostic model may also be valuable in improving patient recruitment into clinical trials.
Introduction
Osteoarthritis (OA) is one of the most prevalent and disabling rheumatic diseases, and therefore, causes a significant public health burden. The knee is the joint most frequently affected by OA, and knee OA (KOA) is responsible for 85% of the total socioeconomic costs derived from the disease.1 2 The strongest risk factors associated with the development of KOA are older age, female sex and high body mass index (BMI). Globally, cases of OA increased by 113% in the last three decades, and the prevalence of OA is expected to increase even further as the population ages and becomes more obese.3
Currently, there is no cure for KOA, and it is not possible to predict who will develop the disease. The diagnosis of KOA is established based on clinical symptoms in combination with radiographic findings indicative of structural joint damage, typically assessed using the Kellgren and Lawrence (KL) grading system. Consequently, joint destruction is irreversible by the time of diagnosis.4 5 Late diagnosis of OA limits opportunities to modify the natural course of the disease in preclinical stages and thereby restore joint homeostasis and prevent joint dysfunction.6 7 Stratification of high-risk groups in the early stages of OA is thus necessary to facilitate good clinical trial outcomes that could promote the development of preventative strategies and personalised medicine therapies for OA.8 9
Advances in the development of early diagnostic tools would allow for prompt management of patients using non-pharmacological strategies and potentially slow disease progression by targeting non-modifiable KOA risk factors.10 11 One of the most promising approaches for achieving this goal entails the discovery, validation and qualification of non-invasive molecular biomarkers and their inclusion in combination with patient demographic and clinical information in prognostic models of KOA. The developmental pipeline for establishing reliable prognostic biomarkers is long due to the need for longitudinal studies in prospective cohorts of well-characterised patients to evaluate biomarker utility in terms of predictive ability and costs efficiency.12
In a previous shotgun proteomics study, our research group identified a specific differential profile of 11 peptides in serum from radiographic KOA (rKOA) patients compared with controls.13 14 In this study, we evaluated the biomarker value of the four proteins from which the aforementioned peptides were derived: apolipoprotein A-I (APOA1), apolipoprotein A-IV (APOA4), zinc-alpha-2-glycoprotein (ZA2G) and alpha-2-antiplasmin (A2AP). The utility of the marker proteins in routine clinical practice was evaluated using a predictive model of the future development of rKOA.
Methods
Study design and population
This study was carried out in two phases: development and validation.15 The outcome was incident rKOA, defined as KL grade ≥2 in at least one knee at any examination during the 96-month follow-up period. The eligibility criterion for study participants was KL=0 in both knees at the time of inclusion (baseline). All analyses were conducted according to the Declaration of Helsinki. Informed written consent was obtained from all participants before inclusion.
This study examined two independent large cohorts with a long follow-up and extensive associated data, which is essential for performing longitudinal studies of OA. The development phase was carried out using serum samples from Caucasian subjects belonging to the OA initiative (OAI) (https://nda.nih.gov/oai), a well-described multicentre prospective cohort from USA that studied KOA. To ensure a blinded outcome assessment and minimise bias, the entire OAI cohort available at baseline (N=1551) was randomised prior to the analyses. All patients from the incidence and non-exposed OAI subcohorts who fulfilled the eligibility criteria and had serum samples available for the molecular analysis were included in the analysis of rKOA incidence. Accordingly, the panel proteins were quantified in samples from 282 subjects with KL=0 in both knees at baseline. Of these subjects, 29 (10.3%) were classified as having incident rKOA (KL≥2), whereas 253 (89.7%) did not develop rKOA by the end of the follow-up period.
External validation was carried out using serum samples obtained from Caucasian individuals of the Prospective Cohort of A Coruña (PROCOAC) cohort from the Grupo de Investigacion de Reumatologia (GIR) group in A Coruña (Spain).13 In this case, a total of 100 patients with KL=0 in both knees were analysed, and of these patients, 15 (15%) developed rKOA during the 96-month follow-up and 85 (85%) did not. This sample size (n=100) in the validation cohort allows estimating an area under the curve (AUC)=0.7 (α=0.05% and precision=±0.07).
Protein quantification
A custom-made multiplex antibody suspension bead array based on Luminex xMAP technology was developed and used to simultaneously determine the absolute levels of APOA4, ZA2G and A2AP in serum samples. APOA1 was quantified using a commercial Milliplex MAP kit (Merck, Darmstadt, Germany). All assays were read using a MagPix plate reader (Luminex, Austin, Texas, USA) according to the manufacturer’s instructions. Part of this analysis was performed by the ICTS ‘NANBIOSIS’, specifically, by the Proteomics Unit of the CIBER in Bioengineering, Biomaterials and Nanomedicine (CIBERBBN) at SERGAS (Spain).
Statistical analysis
A descriptive analysis of the collected data was performed. Continuous variables are expressed as mean, SD, median and IQR, whereas qualitative variables are expressed as absolute and relative frequencies. Differences in continuous variables between patients with incident OA and those without were analysed using the Student’s t-test or non-parametric Mann-Whitney U test, after determining whether the data followed a normal distribution according to the Kolmogorov-Smirnov test. The χ2 test was used to examine associations of qualitative variables between the two groups.
Development and evaluation of the rKOA risk prediction models followed several steps, including feature selection, model development and evaluation of model accuracy and usefulness. Univariate and multivariate logistic regression analyses were used to identify variables independently related to the probability of developing rKOA. Altogether, a total of 36 baseline, clinical and radiographic variables and 4 biomarkers were assessed in the development cohort. In the validation cohort, a total of 64 clinical and radiographic variables and 4 biomarkers were examined. First, each variable was compared individually between prognostic and clinical and radiographic type groups to search for indicators associated with the clinical endpoint. The selected variables were then subjected to binary logistic regression analysis. All variables with p<0.05 in both univariate and multivariate logistic regression analysis (variable entry method) would serve as candidate predictors for modelling. To avoid overfitting and to reduce model predictors, the model was formulated by multivariate logistic regression using the forward stepwise method (stepwise selection probability: predictor entry p<0.05 and predictor removal p>0.15) in the training cohort. In each step, those variables whose coefficient βi was not significantly different from zero were eliminated, using the Wald test as the selection criterion. For the selection of the final clinical model, a parsimonious model was considered, based on the AIC criterion, while maintaining the clinical sense, based on risk factors described in the literature. Subsequently, the clinical model was combined with the biomarkers.
Receiver operating characteristic curve analysis was used to determine the discriminative ability of each model. In each case, cut-off points were calculated using the Youden index. The sensitivity, specificity and probability ratios were also determined in turn to assess the validity and safety of the procedures. CIs for sensitivity and specificity were computed with 2000 stratified bootstrap replicates. The adequacy of multivariable logistic regression analyses was assessed based on the AUC. AUC values for the extended models with biomarkers were compared with those of models including only clinical variables to determine the contribution of each studied biomarker to the clinical models. Among models with similar predictive power, the simplest (fewer variables included) was selected. A nomogram plot was drawn based on the estimated parameters of the proposed model. The model was internally validated using bootstrap techniques with 500 iterations.
The Net Reclassification Index (NRI) was calculated as a measure of predictive improvement when incorporating the new biomarkers into the clinical model. For this purpose, the PredictABEL and rmda packages were used.
Finally, the proposed models were externally validated using the validation cohort with the same covariates and regression coefficients obtained from the development cohort. AUC values were calculated as a measure of discrimination, together with the corresponding 95% CI. The alpha level was set at 0.05, and tests of statistical significance were all two tailed. A value of p<0.05 was considered statistically significant.
This study was conducted and reported in line with the guidelines for Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis.14
Results
Development of a prognostic model of OA incidence based on clinical data from the OAI cohort
A stepwise multivariable logistic regression analysis using clinical data from the OAI cohort was performed to develop a prognostic model of incident rKOA (KL≥2) in individuals without any radiographic sign of the disease. The analysis included 282 individuals from the OAI cohort who had a KL score of 0 in both knees at the time of inclusion. The annual incidence rate for rKOA in the development cohort was 13.45 cases per 1000 subjects. The cumulative probability of rKOA incidence over time in these subjects is illustrated in online supplemental figure 1. Table 1 summarises the most relevant demographic and clinical characteristics of the participants included in this clinical model.
Supplemental material
Descriptive demographic and clinical characteristics of the study participants included in the development phase (OAI cohort) and the validation phase (PROCOAC cohort), together with the levels of the protein biomarkers measured in the sera at baseline
As shown in table 2, those subjects who developed rKOA during the follow-up had a significantly higher (p<0.05) BMI and WOMAC pain at baseline compared with patients who did not develop rKOA. The association of these variables with the incidence of rKOA was confirmed by univariate logistic regression analysis. To facilitate its applicability, the developed clinical model included some of the most important non-radiographic risk factors for KOA, such as female sex, age, high BMI and WOMAC pain. This straightforward model exhibited an AUC (95% CI) of 0.702 (0.598 to 0.805) for discriminating patients with incident rKOA from radiographically healthy controls (KL=0).
Univariate logistic regression, assessing the association of the clinical variables and biomarkers with the prospective incidence of rKOA in patients with KL=0 at baseline
Analysis of novel protein biomarker candidates in serum samples from the OAI cohort
Next, we evaluated the usefulness of a panel of four proteins (APOA1, APOA4, ZA2G and A2AP) as biomarkers for estimating rKOA incidence. Levels of 11 proteotypic peptides derived from these proteins were previously reported to be significantly altered in the serum of rKOA patients compared with controls (online supplemental table 1)16 17; thus, we hypothesised that including these peptides in the clinical model would improve its predictive power. First, levels of the panel proteins were determined in baseline serum samples from 282 individuals from the OAI cohort who had KL=0 in both knees at the time of inclusion. Table 1 summarises the serum protein concentrations The association of ZA2G and APO1 levels with the incidence of rKOA was confirmed by univariate logistic regression analysis (p-value<0.05). The results are shown in table 2 and suggest that higher serum levels of ZA2G and APOA1 are a risk factor for KOA incidence (OR (OR)=1.371 and 1.462, respectively). Higher levels of A2AP at baseline might exert a protective role against rKOA (OR=0.631), although the association between lower A2AP levels and rKOA incidence did not reach statistical significance (p=0.059).
Development of prognostic models combining clinical data and protein biomarkers
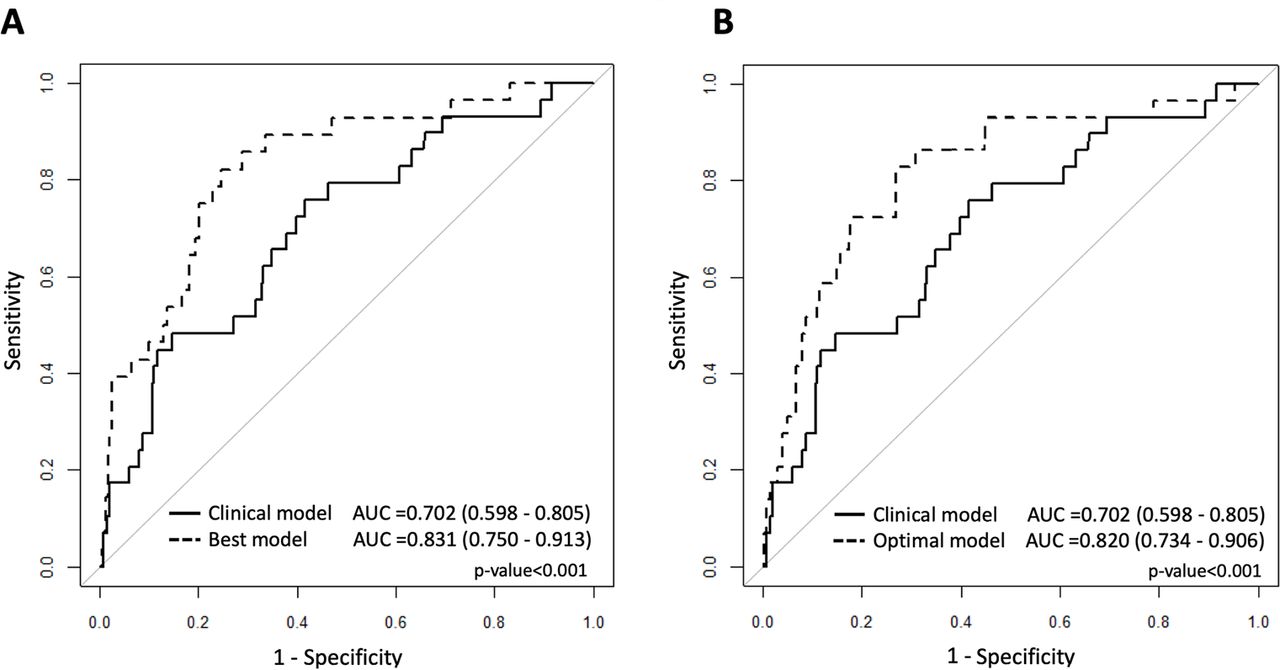
The contribution of the protein biomarkers to the clinical model was also assessed. The AUCs obtained for each combination are shown in online supplemental table 2. The highest predictive value, with an AUC (95% CI) of 0.831 (0.750 to 0.913), was observed for the prognostic model that included the four clinical variables reported above and baseline serum levels of A2AP, APOA1 and ZA2G. The difference in predictive capability between the best-performing model (including the A2AP, APOA1 and ZA2G protein biomarkers) and the clinical model was significant (p<0.001) (figure 1A). No difference was found between the predictive capability of this model and a simpler model including only the serum levels of A2AP and ZA2G (AUC (95% CI)=0.820 (0.734 to 0.906)) together with the clinical variables (p=0.963), hereafter referred to as the optimal model. The optimal model (AUC=0.820) has a significantly better predictive capacity (p<0.001) than the clinical model (AUC=0.702) to discriminate between incident rKOA and non-rKOA at baseline (figure 1B). To correct for overestimation, the proposed models were internally validated using a bootstrap procedure, and the results and parameters including AUC, sensitivity and specificity are detailed in online supplemental table 3.

Overlap of ROC curves and area under the curve (AUC) values for the clinical model and the clinical model including biomarkers to predict KOA incidence in patients with baseline KL=0 in the development phase (OAI cohort). (A) Model with the highest AUC (best performance), including serum levels of the biomarkers ZA2G, A2AP and APOA1. (B) Optimal model, including only the biomarkers ZA2G and A2AP. Inclusion of the biomarkers significantly improved the predictive power of the model built exclusively with the clinical variables age, sex, BMI and WOMAC pain score. No significant differences between the two models were found in terms of AUC. BMI, body mass index; KOA, knee osteoarthritis; KL, Kellgren and Lawrence; OAI, osteoarthritis initiative; WOMAC, Western Ontario and McMaster University Osteoarthritis pain index.
An NRI was calculated to quantify the added value of the biomarkers. The NRI demonstrated that the proposed models improved the discriminative ability of the clinical model, with a value of 0.856 (0.528–1.184) for the best performance model and 0.839 (0.559–1.118) for the optimal model (online supplemental table 3). The categorical NRI (0.1–0.3) was 0.379 for the optimal model and 0.483 for the best performance model in the presence of the outcome (online supplemental table 4). As shown in supplemental table 4, the optimal model displayed a net reclassification of 37% of incident subjects classified as having higher risk (11/29 events as upward movements), while the best performance model showed a higher net reclassification (48%) (with 14/29 upward movements). Altogether, the global NRI (0.1–0.3) was 0.39 (0.18–0.60) and 0.52 (0.28–0.76) for the optimal and the best performance models, respectively.
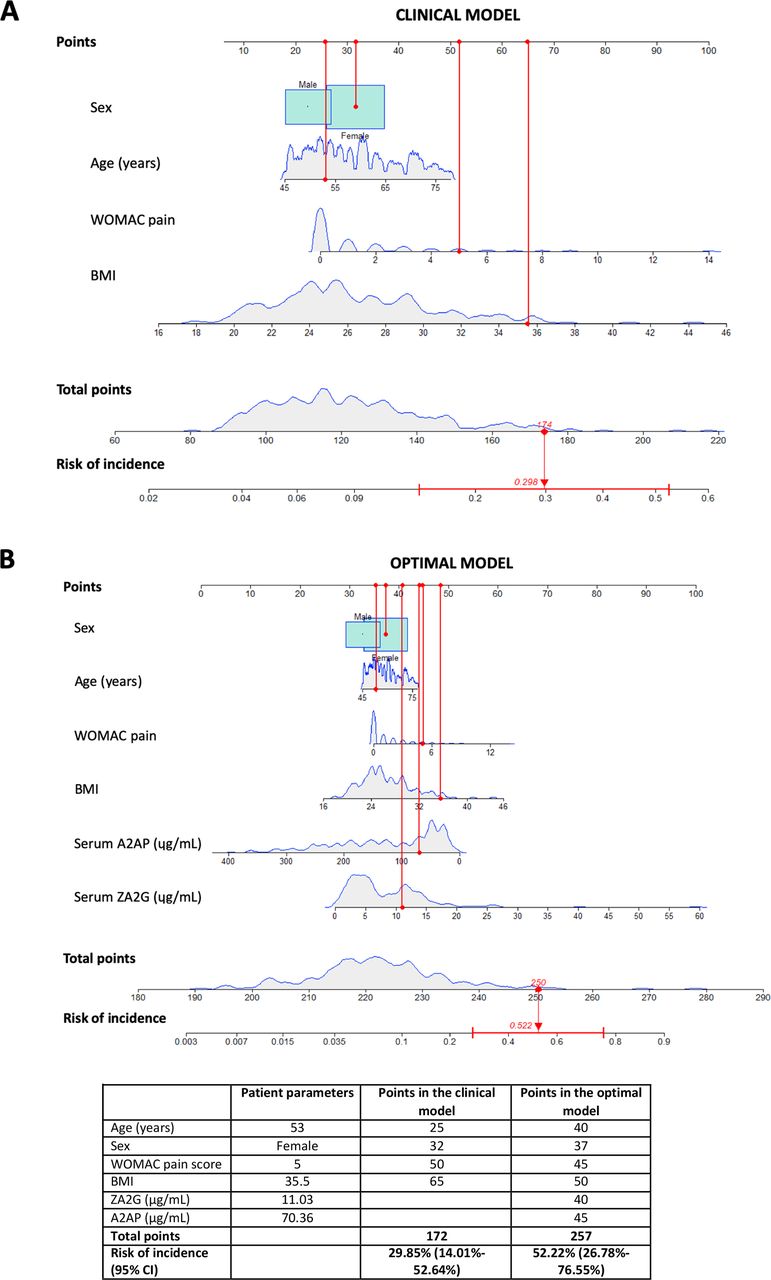
Based on the estimated parameters of the developed models, a nomogram was constructed to enable easy estimation of the risk of rKOA using the best performance model (online supplemental figure 2). Figure 2 shows the application of this clinical tool in a real-world case of a woman from the OAI cohort with incident rKOA as an example of how the nomogram obtained with the optimal model (figure 2B) enhanced the ability to assess the risk of developing rKOA over the clinical variables (figure 2A). The mathematical expressions employed to estimate the probability of incidence, based on the parameters included in the developed models, are described in online supplemental table 5.

{kind=link}
{kind=link}
Nomogram developed as clinical tool for predicting radiographic knee osteoarthritis (rKOA) incidence in individuals with baseline Kellgren and Lawrence (KL)=0. (A) Including only clinical variables (age, sex, body mass index (BMI) and WOMAC score) and (B) considering the optimal model developed in this study, which also included serum levels of ZA2G and A2AP. In using the nomogram, the scale at the top of the figure indicates the points that correspond to the score for each predictor. Once all the points for each predictor are summed, the total points scale at the bottom of the nomogram is aligned with the risk of incidence scale to determine the probability a particular individual will develop rKOA within a period of 96 months. A histogram of the data for each variable recorded in the development phase is shown to provide an overall landscape of the study population. As an example, a woman of 53 years of age with a BMI of 35.5 kg/m2 and WOMAC pain score of 5 shows a total of 172 points (29.85% risk of incidence) when applying the nomogram of the clinical model. For this individual, the nomogram of the optimal model provided a risk of incidence 85 points higher than the clinical model, with a probability of 52.22%. WOMAC, Western Ontario and McMaster University Osteoarthritis pain index.
External validation of the models in the PROCOAC
Finally, the usefulness of these models for predicting the incidence of rKOA was determined by measuring levels of the panel proteins in an independent cohort from A Coruña, the PROCOAC. A total of 100 serum samples from PROCOAC subjects with baseline KL=0 in both knees were analysed. The demographic and clinical characteristics of the study participants included in this analysis are summarised in table 1. The annual incidence rate for rKOA in the validation cohort was 37.88 cases per 1000 subjects. The cumulative probability of rKOA incidence over time in these subjects is illustrated in online supplemental figure 1. As shown in table 3, no statistically significant differences were found regarding the predictive capability of the proposed models as determined for the OAI development cohort and PROCOAC validation cohort, taking Youden’s J statistic as a reference.
External validation in the PROCOAC cohort of the prognostic models that were developed in the OAI cohort
Discussion
Despite the large burden associated with OA, there are no effective drugs for this disease. Non-pharmacological strategies, including changes in lifestyle, exercise or weight loss if required, are thus the primary alternative for mitigating the OA epidemic.18 19 Currently, the lack of prognostic biomarkers for predicting the likelihood of future development of KOA reduces the possibility of intervening in the early stages of the disease, when the course is potentially modifiable.20 21 This study validated and qualified the usefulness of three novel protein biomarkers (APOA1, A2AP and ZA2G) in two independent cohorts for inclusion along with clinical variables in statistical models for predicting the future incidence of rKOA in healthy individuals (flow summarised in online supplemental figure 3).
To develop these statistical tools, we defined a straightforward prognostic clinical model comprising age, sex, BMI and WOMAC pain score. These variables were selected based on their prospective association with rKOA incidence and their accessibility for measurement in clinical practice, avoiding imaging techniques not sufficiently sensitive to detect disease onset, such as X-rays. Also in order to facilitate the applicability of the prognostic model, we did not include the MRI data accessible from the OAI in our analysis. Although they could undoubtedly provide valuable information about early changes in the joint, MRI techniques are not routinely used for OA diagnosis, and in fact, they were not available for the PROCOAC. The addition of serum levels of the analysed biomarkers significantly improved the predictive capability of the model, yielding the highest AUC reported to date in individuals with a KL grade of 0 in both knees (AUC=0.831 (95% CI 0.750 to 0.913)). Interestingly, a similar result was observed when only ZA2G and A2AP serum levels were included in the model (AUC=0.820 (95% CI 0.734 to 0.869)), which could make it easier to implement in clinical practice. The model was validated in the PROCOAC, although reaching a lower AUC. This decrease in the predictive power may be due to the distinctness of the two cohorts, and also to the smaller sample size available in the PROCOAC. Importantly, this difference was not statistically significant (table 3), thus confirming its reproducibility and generalisability. Additional validation studies in other external cohorts might be considered to further substantiate the present model.
To facilitate use of the proposed prognostic model in routine clinical practice, a discriminating nomogram plot was constructed to determine the probability that a given individual will develop rKOA within the subsequent 96 months. Our results clearly demonstrate that the proposed protein biomarkers add value to measurement of conventional risk factors by improving the predictive capability, as well as the sensitivity and specificity, of current clinical models.21
An independent cohort of serum samples was then analysed to validate the performance of the developed models and link the biomarkers to prediction of rKOA development in subjects without any radiographic signs of the disease. The results showed that there were no statistically significant divergences in terms of predictive capability between the models in the two different cohorts analysed.
To our knowledge, there are no in vitro or animal models of OA that include analysis of the proteins included in the models proposed here. Therefore, the potential functional link between these proteins and disease pathogenesis remains unclear. A2AP is a plasma protein of the serine protease inhibitor superfamily commonly known as serpins. These enzymes promote the activation of latent matrix metalloproteinases and can even destroy the extracellular matrix directly. Some previous studies have reported that serpins are downregulated in OA, consistent with the results of our study, which could affect proteolytic activity.22 Although there is no evidence of direct involvement of A2AP in KOA, evidence suggesting serine proteinases play a role in cartilage destruction is now emerging.23 An alternative hypothesis suggests that A2AP functions as the primary inhibitor of fibrinolysis, a process intimately involved in the control of inflammation,24 the pathways of which are activated during the OA disease process.25 Indeed, activation of the fibrinolytic system in the synovial fluid of OA patients has been described,26 and A2AP might play a role in this pathway.
ZA2G is a novel adipokine implicated in playing a role in lipid metabolism. Interestingly, we did not find any significant correlation between the levels of this protein and variations in the BMI. Although the primary source of adipokines is adipose tissue, chondrocytes, synoviocytes and osteoblasts can release these molecules. In addition to the mechanical damage to the joint in KOA caused by load excess, the enhanced secretion of adipokines also affects joint homeostasis.27 In this case, adipokines may contribute to the pathogenesis of OA via synovial inflammation and matrix metalloproteinase production.28 Accordingly, one study reported that ZA2G levels were significantly increased in synovial fluid from osteoarthritic dogs in comparison with controls.29
APOA1, the major constituent of high-density lipoprotein, not only shuttles cholesterol but also exhibits anti-inflammatory functions. Zhang et al recently reported that APOA1 levels in synovial fluid are negatively correlated with KL grade progression and proposed APOA1 as a predictor of disease severity.30 However, Sánchez-Enríquez et al reported higher plasma levels of APOA1 in OA patients in comparison with healthy controls,31 which is consistent with our results. A similar serum APOA1 pattern was also reported by Oliviero et al.32 Previous work from our research group showed that APOA4, which is also involved in lipid metabolism, is significantly associated with KL grade.33 Current data regarding the role of apolipoproteins in OA thus suggest that alterations in the lipid metabolism profile are associated with disease development. Indeed, proper cholesterol distribution plays a critical role in chondrocyte differentiation, whereas abnormal lipid deposition in the joint has been observed in early disease stages.34
The identification of protein biomarkers useful for predicting the incidence of OA has been a central focus of research in recent decades. To date, however, only serum cartilage oligomeric protein has been proposed as a potential biomarker candidate for predicting KOA incidence.35 Furthermore, a recent study carried out in the OAI cohort showed that addition of the protein inter-alpha-trypsin inhibitor heavy chain 1 into a clinical model including age, gender, BMI, WOMAC pain score and previous injury yielded an AUC of 0.786 (95% CI 0.705 to 0.867) for predicting KOA incidence, but this was in subjects with baseline KL≤1 in at least one knee.12 Unlike previous studies, the present work went a step further in validating the sole inclusion of non-invasive biomarkers for early OA prediction for the first time in a study of KOA incidence in subjects without any radiographic evidence of structural joint damage (KL=0) in both knees. The model proposed in this work for predicting rKOA incidence achieved the highest predictive capacity reported to date, an AUC=0.831, with fewer variables. The results of NRI demonstrate the improvement in discriminant ability of the proposed models. All these data support the value of the addition of certain molecular biomarkers to models including demographic and clinical factors in order to improve predictive capability.
Biomarkers for early prediction of KOA development must represent a preradiographic stage to be truly effective and aid in the prevention of joint dysfunction. The validation of novel biomarkers for early OA detection opens new windows of opportunity for OA treatment and could also help facilitate the discovery of new drugs to treat the disease.21 Moreover, the possibility of identifying patients with a higher probability of developing the disease in the subsequent 96 months could prove very useful for improving clinical trial outcomes.36 Thanks to the nomogram developed in this work, the proposed algorithm overcomes the critical hurdle in the translation of biomarkers from discovery to clinical application. This nomogram can be easily used as a prognostic tool to facilitate the implementation of the model in routine clinical practice, facilitating the early management of patients in order to delay disease progression,21 thereby decreasing the burden of the disease and potentially leading to personalised medicine therapies for OA.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Comité ético de investigación clínica de Galicia. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the study participants who made this work possible by their generous donation of samples. The Osteoarthritis Initiative (OAI) is a public–private partnership comprised of five contracts (N01-AR-2-2258; N01-AR-2-2259; N01-AR-2-2260; N01-AR-2-2261; N01-AR-2-2262) funded by the National Institutes of Health, a branch of the Department of Health and Human Services, and conducted by the OAI Study Investigators. Private funding partners include Pfizer; Novartis Pharmaceuticals Corporation; Merck Research Laboratories and GlaxoSmithKline. Private sector funding for the OAI is managed by the Foundation for the National Institutes of Health. Part of the protein analysis was performed by the ICTS 'NANBIOSIS', specifically by the Proteomics Unit of the CIBER-BBN at SERGAS (Spain).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors RP-G, CR-R and FJB conceived and designed the study, and drafted the article. RP-G, LL, VC and PF-P carried out the data acquisition. RP-G, VB-B, NO, CR-R and FJB conducted the data analysis and interpretation. All authors revised and approved the final manuscript for submission. FJB is the guarantor for this manuscript.
Funding This work has been funded by Instituto de Salud Carlos III (ISCIII) through the projects PI19/01206, PI20/00793, PI20/01409 and PI22/01155, and co-funded by the European Union, and also by the grant RD21/0002/0009 financed by Instituto de Salud Carlos III–European Union-NextGenerationEU-Plan de Recuperación transformación y resiliencia. This study has been also supported by grants IN607A2021/07 and IN607D2020/10 from Xunta de Galicia. The Biomedical Research Networking Center (CIBER) is an initiative from Instituto de Salud Carlos III (ISCIII). LL is supported by Contrato Sara Borrell (CD19/00229), Fondo de Investigación Sanitaria, ISCIII. VC is supported by RICORS-REI RD21/0002/0009.
Disclaimer CR-R and FJB hold a patent for a method for the diagnosis of osteoarthritis based on peptide biomarkers (ES2568702B1, WO 2016/051006A1). This manuscript was prepared using an OAI public use data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH or the private funding partners.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.