Article Text

Abstract
Background Polymyalgia rheumatica (PMR) and Giant cell arteritis (GCA) are chronic inflammatory diseases. Despite the progress made in the management of these conditions, new unmet needs have emerged particularly in terms of prevention of disease- and treatment-related complications. A treat-to-target (T2T) strategy, which has been well established in other rheumatic diseases, has not yet been developed for PMR and GCA.
Objectives To retrieve current evidence on T2T strategies in PMR and GCA to inform an international task force (TF) developing T2T recommendations.
Methods A systematic literature review (SLR) was conducted. Medline, EMBASE, Cochrane Library and clinicaltrials.gov (from inception until May 2022), as well as EULAR/ACR abstract databases were searched (2019-2021). Randomized controlled trials (RCTs) and non-randomized interventional studies published in English and answering at least one of the eleven PICO questions on treatment targets and outcomes, were identified (Table 1). The study selection process, data extraction, data synthesis and risk of bias assessment were conducted independently by two investigators.
Results Of 7809 screened abstracts, 397 were selected for detailed assessment and 76 papers were finally included (31 RCTs, 8 subgroup/exploratory analyses of RCTs and 37 non-randomized interventional studies). No study comparing a T2T strategy against standard of care was identified.
In PMR RCTs, treatment-related outcomes were most commonly used (90.9% of RCTs), specifically in terms of the glucocorticoids (GC) cumulative dose and GC tapering, followed by clinical, laboratory and safety targets (63.3% each). Conversely, the most frequently reported outcomes in RCTs in GCA were prevention of relapses (72.2%), remission, treatment, and safety (66.7 % each).
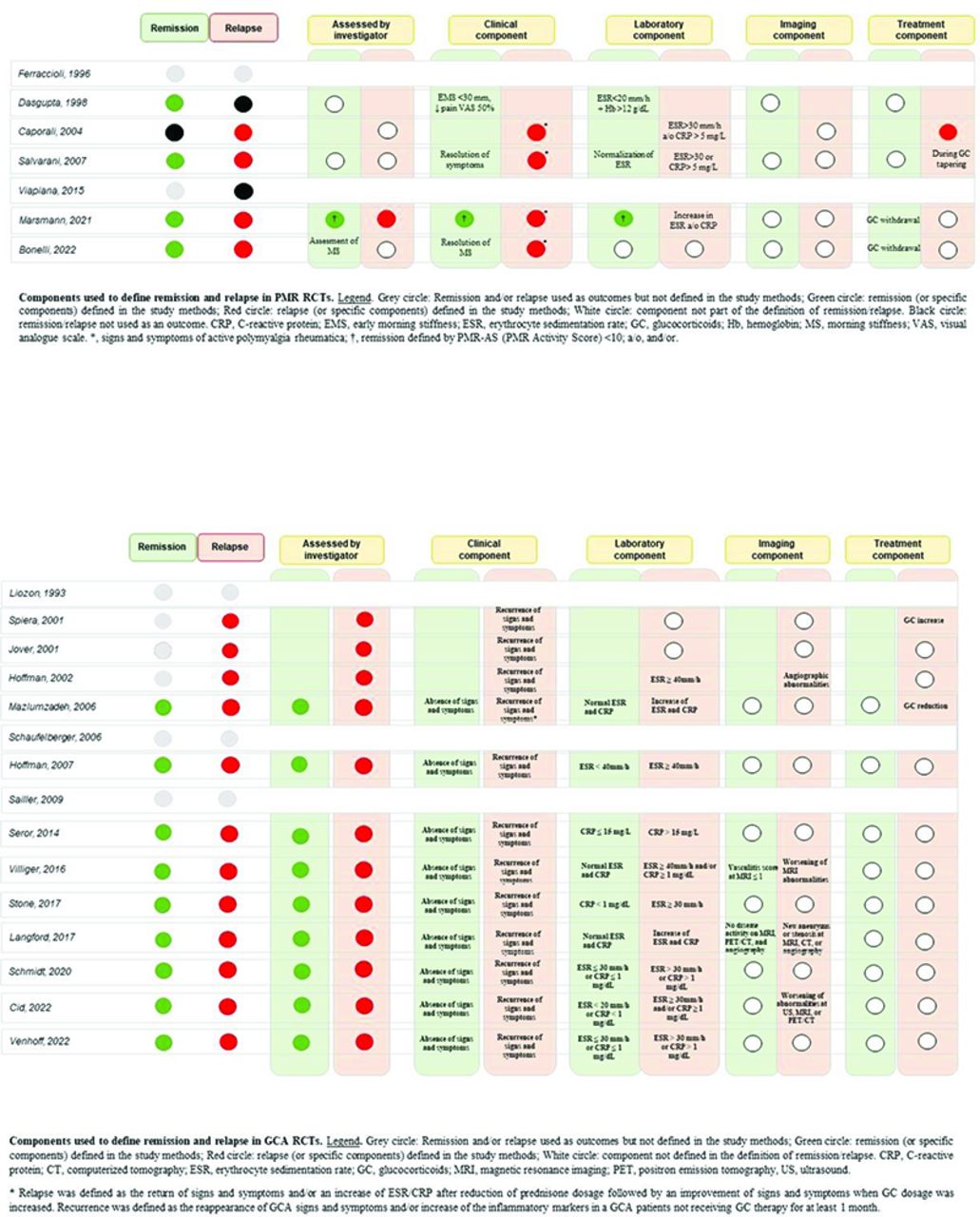
Remission and relapses were variably defined in PMR and GCA RCTs but, in most cases, they comprised a combination of clinical and laboratory parameters (Figure 1).
The following predictors of poor treatment response were identified: for GCA, data from RCTs yielded female sex, initial prednisone dose <30mg/day, bad baseline patient-reported outcomes, increased inflammatory markers after the achievement of clinical remission and absence of PMR symptoms at baseline as risk factors for treatment failure and an increased relapse rate. In PMR, no high-quality data predicting clinical outcomes were identified.
Finally, in RCTs comparing the outcomes of GCA patients with new onset versus established disease, no differences were found, given that treatment was equal in both groups.
Conclusion This SLR informed an international TF developing T2T recommendations in PMR and GCA. It provides up-to-date evidence while simultaneously highlighting the gaps in current knowledge about T2T strategies in these diseases.
Clinical key questions

{kind=link}
Components used to define remission and relapse in PMR and GCA RCTs
Acknowledgements 1. Elvis Hysa and Milena Bond contributed equally to this work.
2. Grant support from Abbvie.
Disclosure of Interests Elvis Hysa: None declared, Milena Bond: None declared, Lisa Ehlers: None declared, Dario Camellino Speakers bureau: speaker fees from Abiogen, BMS and GSK, Louise Falzon: None declared, Christian Dejaco Speakers bureau: consulting/speaker’s fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer, Roche, Galapagos, Sparrow and Sanofi, Consultant of: consulting/speaker’s fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer, Roche, Galapagos, Sparrow and Sanofi, Grant/research support from: grant support from Abbvie, Frank Buttgereit Speakers bureau: consultancy fees, honoraria and travel expenses from Abbvie, Novartis, Pfizer, Roche, and Sanofi, Consultant of: consultancy fees, honoraria and travel expenses from Abbvie, Novartis, Pfizer, Roche, and Sanofi, Daniel Aletaha Speakers bureau: grants, speaker fees, and/or consultancy fees from Abbvie, Amgen, Galapagos, Lilly, Janssen, Merck, Novartis, Pfizer, Sandoz, and Sanofi, Consultant of: grants, speaker fees, and/or consultancy fees from Abbvie, Amgen, Galapagos, Lilly, Janssen, Merck, Novartis, Pfizer, Sandoz, and Sanofi, Grant/research support from: grants, speaker fees, and/or consultancy fees from Abbvie, Amgen, Galapagos, Lilly, Janssen, Merck, Novartis, Pfizer, Sandoz, and Sanofi, Andreas Kerschbaumer Speakers bureau: consultancy fees, honoraria and travel expenses from AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Gilead, Janssen, Merck Sharp and Dohme, Novartis, UCB and Pfizer, Consultant of: consultancy fees, honoraria and travel expenses from AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Gilead, Janssen, Merck Sharp and Dohme, Novartis, UCB and Pfizer.
- Remission
- Vasculitis
- Treat to target