Article Text

Case presentation
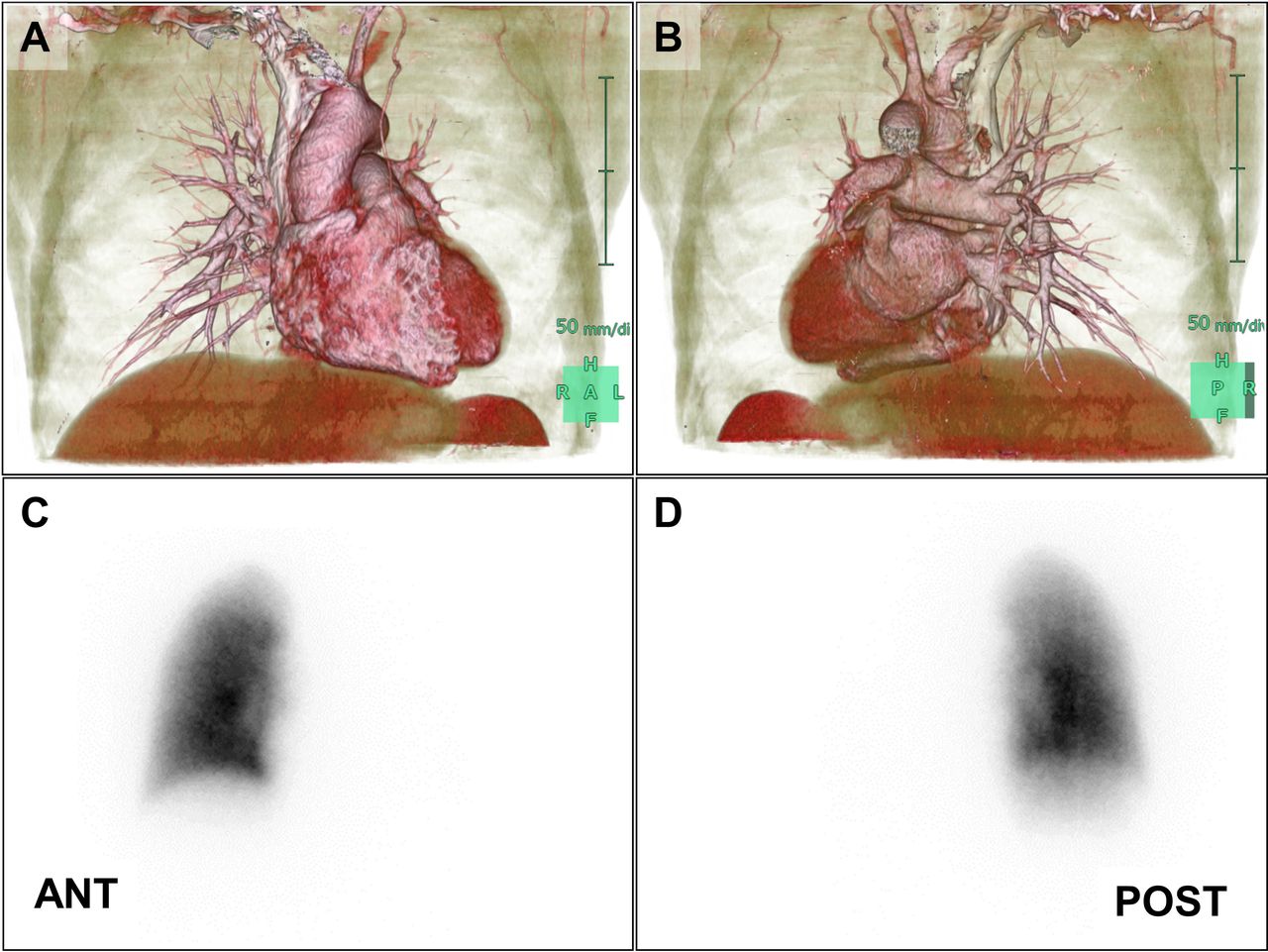
A 47-year-old man developed chest pain and low-grade fever. He was diagnosed with pneumonia with parapneumonic pleural effusion using a chest X-ray image (figure 1A) and CT without contrast (figure 2A). Although he received azithromycin, followed by garenoxacin, imaging indicated worsening of the condition (figures 1B and 2B). As haemoptysis was observed, he was referred to our hospital.

Chest X-rays taken at the time of the first onset of illness (A), on the day of bronchoscopic examination (B), on the first day of prednisolone (0.5 mg/kg/day) treatment (C) and after prednisolone administration (0.5 mg/kg/day for 7 days and 1 mg/kg/day for 7 days) (D).

Chest CT scans obtained at the time of first onset of illness (A), at the time of the first visit to our hospital (B), on the day of bronchoscopic examination (C) and after prednisolone administration for 14 days (D). Arrowheads indicate the site for transbronchial lung biopsy.
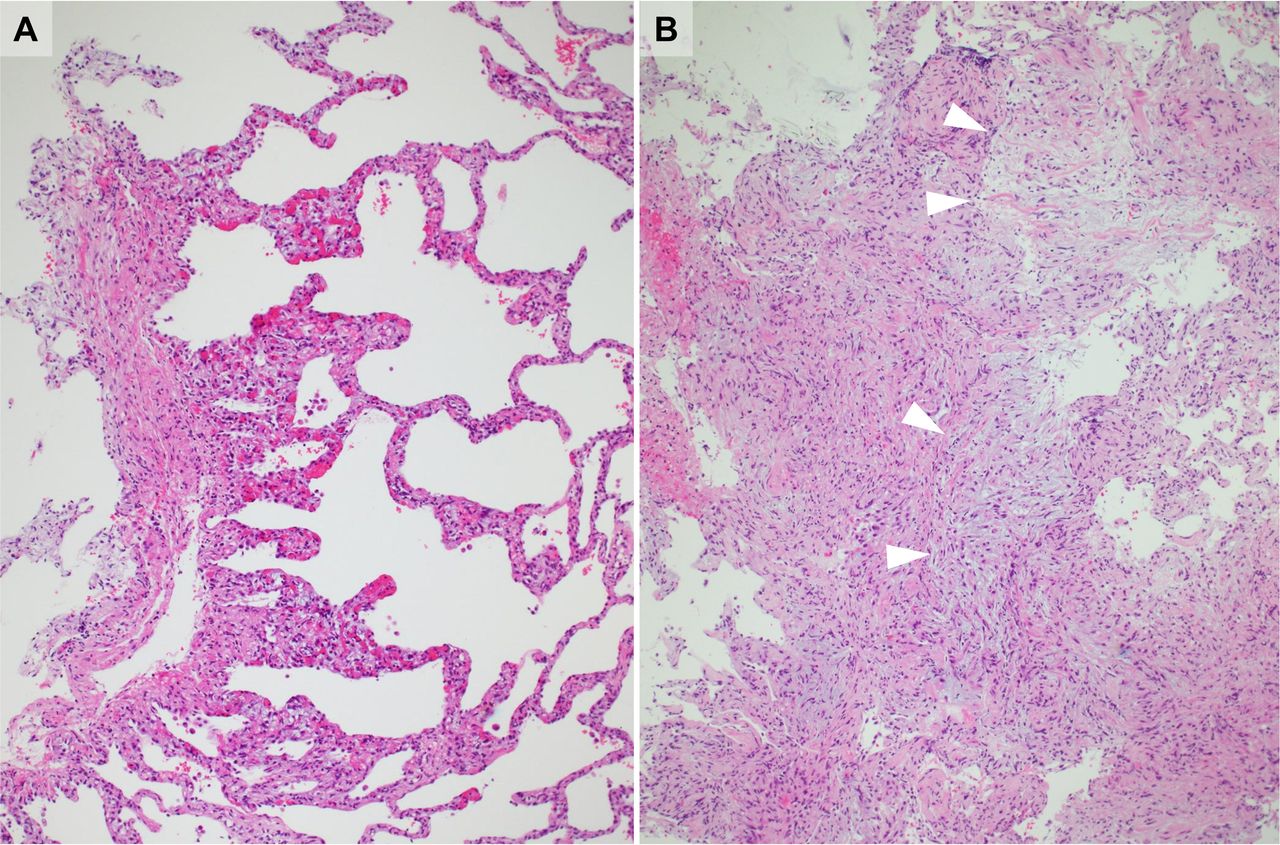
He had never smoked and had been previously healthy except for atrial fibrillation that had been successfully treated via catheter ablation, without complications, 5 months previously. Physical examination revealed normal percussion and auscultation findings for both lungs, a blood pressure of 110/60 mm Hg, peripheral oxygen saturation of 97% at room air, a heart rate of 88/min without arrhythmia, a respiratory rate of 18 breaths/min and a body temperature of 36.8℃. Routine blood tests yielded no remarkable finding except a C reactive protein level of 30.2 mg/L. Bronchoalveolar lavage and transbronchial lung biopsy of the apicoposterior segment of the left upper lobe (figures 1C and 2C) were performed. The lavage fluid was clear and the cells included macrophages (90.2%), neutrophils (5.8%), eosinophils (0.2%) and lymphocytes (3.8%). Histological examination revealed some tissue plugs within the lumina of the small airways, part-extending into the alveolar ducts and alveoli. Two weeks after bronchoscopic examination, we prescribed prednisolone (0.5 mg/kg/day) because the infiltration had progressed to the left lower lung field. Although the consolidation transiently regressed, it became slightly worse 2 weeks after treatment (figure 1D). Although we increased prednisolone (to 1 mg/kg/day), opacities in the left upper lobe migrated (figure 2D).
Question
What is the differential diagnosis of this ‘wandering consolidation’?



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
Contributors TK, NO and NT wrote the manuscript. YN, TK, NN, NO, HN, HY and NT treated the patient. KK and KS supervised the imaging analysis. YM supervised the histological diagnosis and capturing imaging.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Airwaves