Article Text

Abstract
Background Communication is problematic in healthcare. The Veterans Health Administration is implementing Medical Team Training. The authors describe results of the first 32 of 130 sites to undergo the programme. This report is unique; it provides aggregate results of a crew resource-management programme for numerous facilities.
Methods Facilities were taught medical team training and implemented briefings, debriefings and other projects. The authors coached teams through consultative phone interviews over a year. Implementation teams self-reported implementation and rated programme impact: 1=‘no impact’ and 5=‘significant impact.’ We used logistic regression to examine implementation of briefing/debriefing.
Results Ninety-seven per cent of facilities implemented briefings and debriefings, and all implemented an additional project. As of the final interview, 73% of OR and 67% of ICU implementation teams self-reported and rated staff impact 4–5. Eighty-six per cent of OR and 82% of ICU implementation teams self-reported and rated patient impact 4–5. Improved teamwork was reported by 84% of OR and 75% of ICU implementation teams. Efficiency improvements were reported by 94% of OR implementation teams. Almost all facilities (97%) reported a success story or avoiding an undesirable event. Sites with lower volume were more likely to conduct briefings/debriefings in all cases for all surgical services (p=0.03).
Conclusions Sites are implementing the programme with a positive impact on patients and staff, and improving teamwork, efficiency and safety. A unique feature of the programme is that implementation was facilitated through follow-up support. This may have contributed to the early success of the programme.
- Healthcare quality improvement
- communication
- teamwork
- safety culture
- crew resource management
Statistics from Altmetric.com
Introduction
Background
Ineffective communication contributes to adverse events in healthcare.1–5 Seventy-six per cent of root cause analyses in The Veterans Health Administration (VHA) identified problems with communication. Several studies identified that better communication and/or teamwork are associated with improved patient outcomes and/or processes of care.4 6–13
Problem
Communication is a challenge in surgical care.14 15 In an analysis of 342 surgical adverse events in the VHA over five and a half years, the most common root cause was communication problems.
Recognising the importance of improved communication, the VHA developed and implemented a Medical Team Training (MTT) programme for operating room (OR) and intensive care unit (ICU) staff. The VHA MTT programme is based upon the aviation model of crew resource management and is adapted for healthcare. Aviation uses a teamwork approach which includes preflight briefings and principles such as flattening the hierarchy so all team members can voice safety concerns.16 17 The Institute of Medicine18 and Joint Commission19 recommend implementing team training programmes. Others are using briefings or team training to improve patient safety with positive results.20–30
Purpose of change
The goals of the MTT programme are to improve patient outcomes and staff satisfaction by facilitating communication through teamwork.
The main questions we sought to answer were:
To what degree did facilities implement skills taught in the MTT programme?
What impact did implementation have on patient safety, processes of care and team functioning/staff satisfaction?
We hope this interim report provides useful information for others implementing similar programmes outside the VHA, and informs future implementers within the VHA.
Methods
Study design
The study design is a descriptive analysis of reactions to a learning session and self-reported behaviours implemented as a result of the programme. This is a preliminary report and includes only 32 of the 130 facilities that will be trained. This report includes the reaction and behaviour phases of Kirkpatrick's model.31
Setting and function
The VHA includes 130 facilities that provide surgical care. The target audience was staff who provided surgical care such as OR and ICU staff. One of the main components of the programme was briefings and debriefings. VHA hospitals vary in size and location, and the majority (71%) of facilities that provide surgical care have surgical residents. The first nine facilities in this study volunteered to participate in the programme; the following 23 were part of the national roll-out of the MTT programme throughout the VHA system.
Intervention
The VHA MTT programme has three phases: (1) preparation and planning, (2) the learning session and (3) implementation and follow-up.
Phase 1: preparation and planning
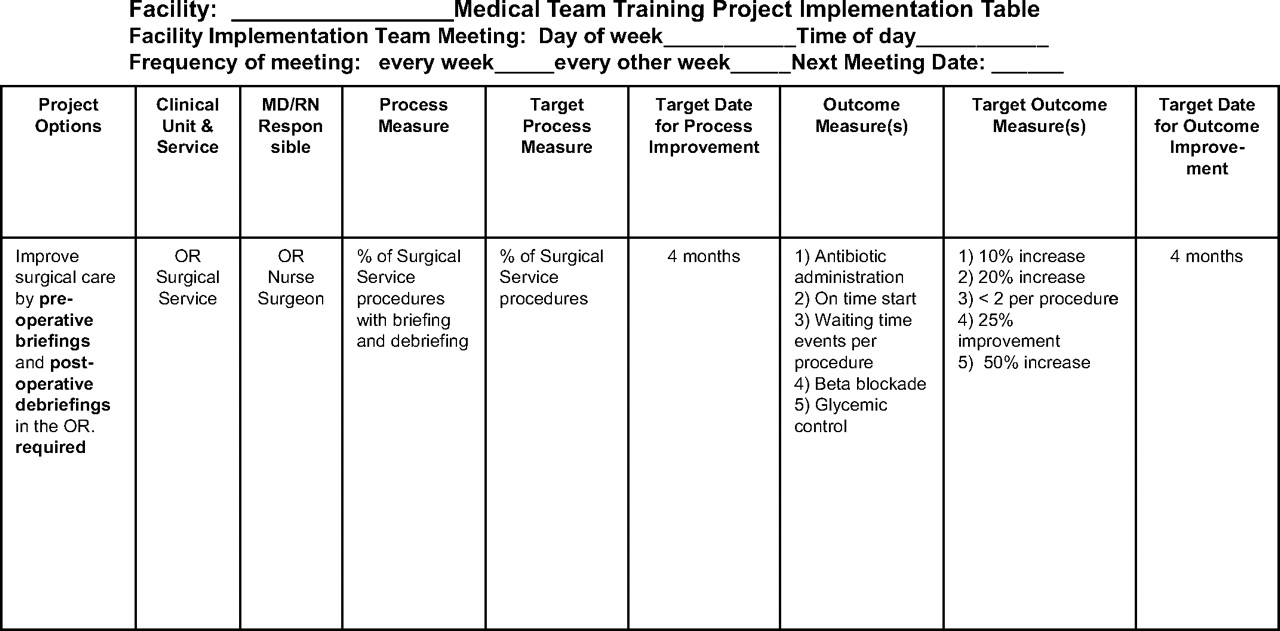
During preparation and planning, MTT faculty worked with surgical staff at the facility to compose an implementation team and held calls with this team. The implementation teams consisted of leaders (eg, Chief of Surgery, OR Nurse Manager) as well as frontline personnel. Faculty assisted the team in developing a project plan to improve communication over the 12 months following the learning session. Teams were asked to plan to implement briefings and debriefings, and to select other communication projects. Figure 1 is an example of the components of an implementation table which teams developed in the preparation and planning of the programme.

Implementation table.
Phase 2: learning session
The learning session was a day-long interactive conference held at the facility. The OR was closed to achieve maximum attendance. We used lecture, discussion and videos including topics such as scenarios of effective and ineffective communication, how to conduct briefings and a difficult code situation where a variety of communication tools were necessary to ensure patient safety. The day ended with a session for the implementation team to finalise project plans. Many sites shared how rare and valuable it was to have all OR staff in one room at the same time and discuss how to improve communication.
During the learning session, participants were taught a variety of communication skills, such as preoperative briefings, postoperative debriefings, patient-centred interdisciplinary rounds, utilising communication rules of conduct, fatigue management and structured communication such as SBAR (Situation, Background, Assessment, Recommendation) for handoffs.27 32–35
Preoperative briefings and postoperative debriefings are the cornerstones of the programme. The preoperative briefing is a face-to-face discussion involving the surgical team (surgeon, anaesthesiologist, circulating nurse, scrub nurse, resident, physician assistant, others) ensuring all have a common understanding of what will be done and that everyone has what they need for the case. The debriefing focuses on what went well and what could be improved (figure 2).

Example of briefing/debriefing guide checklist elements. This list was developed based upon a sampling of the majority of elements as suggested by frontline OR teams from the VA as well as some additional features from the WHO Surgical Safety Checklist, which is available at: http://www.safesurg.org/uploads/1/0/9/0/1090835/sssl_checklist_finaljun08.pdf. We encourage sites to create and develop guides/checklists that are specific to their facility and specialty specific as indicated. We hope this list is helpful to sites when they are developing or modifying their preoperative briefing and postoperative debriefing guides.
Phase 3: implementation and follow-up
To reinforce skills taught and to help teams implement communication projects, we conducted semistructured, quarterly consultative telephone interviews with the teams to explore implementation during the year following their learning session. The phone interviews included coaching, such as how to overcome obstacles and suggestions for implementation from the faculty. Team members participating in the interviews usually consisted of the OR nurse manager, chief of surgery or a surgeon champion, staff nurses, anaesthesia staff, often the ICU nurse manager and an ICU physician champion.
Measures and analytical methods
Facility characteristics
Number of surgical procedures performed and percentage of facilities that are teaching hospitals (defined as having surgical residents).
Learning session evaluations
Participants completed faculty and programme evaluations.31
Interview coding
Interview results for the 32 sites (126 interviews) were reviewed and summarised.
Interview measures
The interview measures were as follows:
degree of implementation of briefing and debriefing at final interview (from ‘None’ to ‘All services, all cases’);
percentage of facilities that implemented an additional project at any time during follow-up;
perceived self-reported impact ratings on staff and patients as of final interview;
percentage of sites with improved OR or ICU teamwork;
improved OR efficiency;
percentage of sites that reported a success story or undesirable event avoided.
Regression analysis
Logistic regression was used to examine factors related to high levels of briefing and debriefing activities. The independent variables were:
teaching facility (having surgical residents);
inpatient surgical volume (high volume=more than 1000 annual procedures in fiscal year 2007);
leadership on 75% or more of the interviews;
surgeon on 75% or more of the interviews;
number of projects implemented besides briefings/debriefings at any time during the project.
Results
Situation analysis
Fifty per cent of the 32 facilities performed more than 1000 inpatient surgical procedures per year, with a range of 163–3045 procedures. Seventy-two per cent of the 32 facilities had surgical residents. Ninety-two per cent of participants agreed or strongly agreed that the programme was worth while. Complete learning session data were available for 26 of the 32 learning sessions.
Outcomes
Facility interviews
Nearly all facilities (97%) were implementing briefings and debriefings as of their final interview, with 28% doing so for all cases in all services (figure 3). These implementation percentages refer to the process and conversation of a briefing and debriefing, not to the time out of the Universal Protocol.36 Although some sites reported they conducted the preoperative briefing in conjunction with the time out, the briefing is still a distinct communication tool that involves a conversation about the upcoming case. The timing of briefings varied, though the majority (61%) reported performing the briefing before induction of general anaesthesia. Figure 2 provides an example of a briefing/debriefing guide checklist elements. We encouraged teams to modify the briefing/debriefing guides for their facility and for specialties.

Degree of implementation of briefings and debriefings at the final interview.
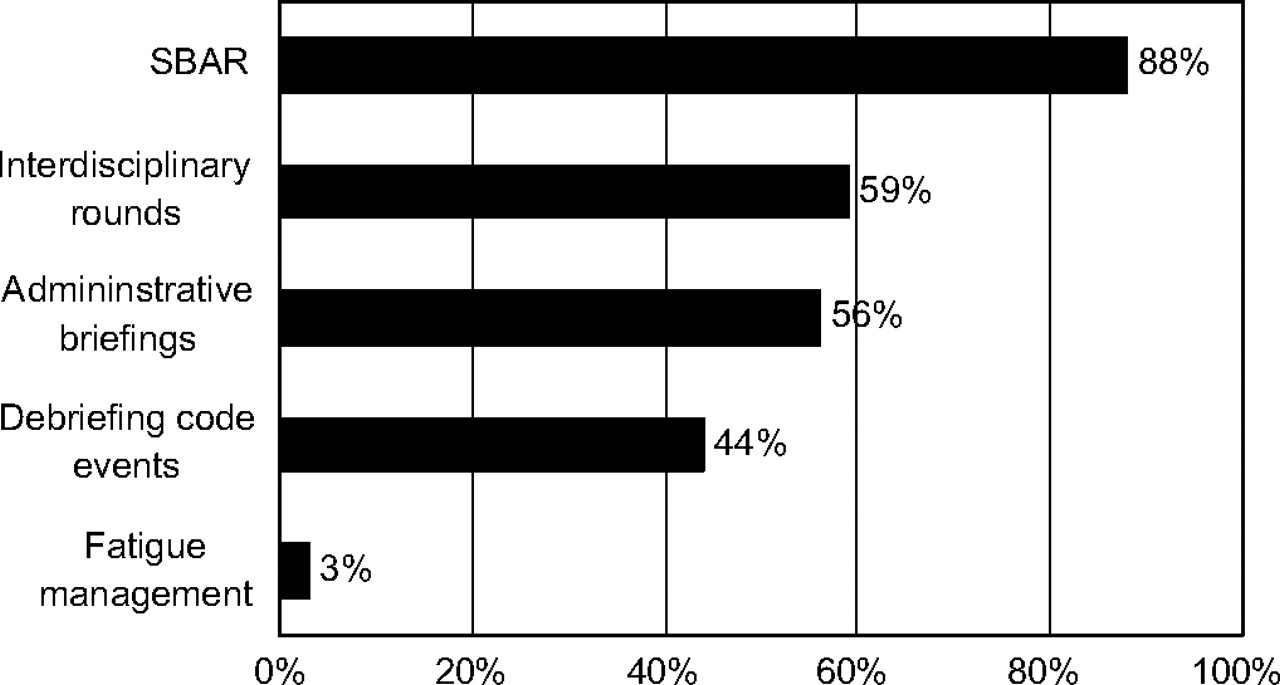
All facilities reported implementing a project in addition to the briefing/debriefing during the follow-up period (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Additional projects implemented during the follow-up period.
OR and ICU facility teams rated the self-reported impact of MTT on staff and patients using a 1–5 scale, where 1 represented ‘no impact,’ and 5 represented ‘significant impact.’ As of the final interview, 73% (22/30) of OR teams and 67% (12/18) of ICU teams gave a self-reported rating of 4–5 for MTT impact on staff. Eighty-six per cent (25/29) of OR teams and 82% (14/17) of ICU teams gave a 4–5 self-reported rating for perceived patient impact.
Improved teamwork was reported by 84% of OR teams and 75% of ICU teams. Efficiency improvements were reported by 94% of OR teams. Specific reported elements of teamwork and efficiency are shown in table 1.
Improvements reported by implementation teams during medical team training interviews (N=32)
Most facilities (97%) reported a success story or that they had avoided an undesirable event at some time during the project. A sampling of examples is provided in Box 1.
Box 1 Sampling of success stories or undesirable events avoided reported by implementation teams during medical team training interviews
On a redo heart case, where the likelihood of complication was high, the scrub nurse realised that there tends to be differing opinions about what to do if complications arise and asked during the briefing what the plan was. They realised that there were indeed different ideas, but they discussed and resolved before the incision, so that if a problem did happen, they knew what to do and were all on the same page.
The OR was conducting the preoperative briefing for a patient on warfarin and discovered that they did not have an INR for the patient. After obtaining the INR, they found it was too high and cancelled the case, thus avoiding an adverse event.
In the first carotid case, the briefing helped avoid getting to shunt insertion and not having the proper shunt available. They were able to have the correct equipment in time. On the second case, a general vascular set was pulled instead of a carotid set, and this was caught and corrected during the briefing.
They have seen a decrease in cancellations in the OR, and the flash sterilisation rate has decreased from 50% to 5%, now that staff members are asked to check in before flashing instruments.
In July, they had 715 min of delay and 25 cases delayed; in September, 342 min and 13 cases delayed; and in December, 364 min and 16 delays. They have cut their delays by about half.
The OR has seen improvements in communication, including surgeon's intent, having necessary equipment on hand and patient positioning. The ICU staff have also seen improvements in communication, particularly nurse to nurse as related to the SBAR handoffs.
Ventilator days of care and length of stay have both decreased since initiating the MTT programme.
The ICU has seen a decrease in the number of patient readmissions and improvements in bed flow and communication, though there is still room for some improvement.
The OR project team decided to add a check box for DVT prophylaxis for appropriate patients to their briefing tool because they were not satisfied with their measure for that area of care. Following this addition, they achieved 100% for DVT prophylaxis. They also added a wound classification section to the briefing tool to ensure correct classification (agreement by the surgeon) and appropriate care for the wound.
The results for the logistic regression were significant only for surgical volume (p=0.03); sites with a lower volume were more likely to conduct briefings/debriefings in all cases for all surgical services.
Discussion
Our results indicate that a communication improvement programme for OR and ICU clinicians can improve reported perceptions of teamwork, safety and efficiency. In addition, the majority of teams reported the project was helpful to their staff and patients. These results appear to have been achieved through the implementation of communication skills over the course of the follow-up period after the learning session. These initial results were achieved in both teaching and non-teaching hospital of varied sizes.
The majority (84%, OR and 75%, ICU) reported improved teamwork, which was our primary objective. An added benefit is that 94% of ORs reported improved efficiency. Many used improved efficiency results to encourage buy in from additional surgical specialties.
Sites with lower surgical volume were more likely to end the programme with briefing and debriefing all cases in all services. Larger facilities may require more support with implementing briefings and debriefings in all cases and all services.
While some of the literature reports positive results from team training programmes,20–30 our results differ from other studies of MTT using principles of Crew Resource Management. Nielsen et al found no difference in impact for an obstetrics-related team-training programme.37 France et al also found no impact from a team-training programme.38 The main difference between our programme and others is that we worked with facilities prior to the learning session to develop an individualised communication improvement plan, and coached teams over a follow-up period. Pratt et al also reported that coaching implementation was a key factor in their success.22 Our programme also required briefing and debriefing rather than depending on the participants' devising their own ways to employ what they learnt in the training.
Our study has several limitations: we observed change over time without comparison with a control group. Consequently, it is impossible to say with certainty whether changes can be attributed to our interventions. In addition, these data are self-reported and therefore susceptible to observation bias. We think this is unlikely, however, since there was variation in the degree of implementation of briefings and debriefings, and the impact scores also varied. Future plans include using administrative databases to examine before/after outcomes which may help decrease possible self-report bias.
Conclusions
Early results of the VA MTT programme are encouraging with a high degree of reported implementation and positive impact on staff and their perceptions of enhanced teamwork and also on patients and efficiency. Our model is a unique approach to implementing MTT and is likely to have contributed to the programme's early success. These results will inform those VA facilities who have not yet implemented MTT or who are in the midst of their follow up period. These early results might also benefit private-sector facilities implementing a team training programme, so they go beyond just training and offer facilitated implementation through prework and follow-up coaching.
Acknowledgments
We would like to acknowledge S Boar, for her diligent work in support of the evaluation process.
References
Footnotes
Funding This work is based upon work supported by the Department of Veterans Affairs, Veterans Health Administration.
Competing interests None.
Ethics approval This project was considered exempt from further review by the Dartmouth comittee for the Protection of Human Subjects.
Provenance and peer review Not commissioned; externally peer reviewed.