Article Text

Statistics from Altmetric.com
Healthcare systems worldwide have for decades sought to prioritise prompt diagnosis of cancer as a means to improve outcomes. The gatekeeping role of general practitioners (GPs) that restricts access to testing and referral,1 along with their relatively lower propensity to use diagnostic tests,2 has been offered as partial explanations for the UK’s consistently poor performance in cancer compared with other high-income countries.3
In this issue of BMJ Quality & Safety, Akter and colleagues examined primary care investigations prior to a cancer diagnosis using data on 53 252 patients and 1868 general practices from the 2018 English National Cancer Diagnostic Audit.4 Grouping tests into four categories (any investigation, blood tests, imaging and endoscopy), the study demonstrated large variation in use of tests in general practice prior to diagnosis with cancer. Recorded characteristics of practices accounted for only a small proportion of this variation, suggesting the possibility that testing behaviours could be amenable to change, for example, by encouraging greater uptake of particular tests in certain patient groups. Whether such a strategy would benefit patients is unknown and as the study reported on tests in aggregate, rather than the pertinent test for that particular cancer, no definitive judgement can be drawn regarding whether higher levels of testing in the prediagnosis period would have expedited diagnosis.
Akter et al found that the ‘blood test’ category was the test most frequently performed in those who were later diagnosed with cancer, with 23 422 out of 53 252 patients (44%) receiving such a test. Abnormalities on full blood count (FBC) are one (among other) criterion for further investigation or referral for gastrointestinal, endometrial, lung and haematological malignancies but testing with non-specific blood tests does not otherwise feature within National Institute for Health and Care Excellence guidance for diagnosing cancer in general practice.5 However, in some other situations, FBC, along with other tests like inflammatory markers, may help inform decision-making about whether to undertake further investigation or referral when faced with non-specific symptoms or particular uncertainty.6
Uncertain benefits from increases in general practice testing
Substantial increases in blood and imaging tests from general practice in the UK have been observed in recent decades, resulting in costs of around £2.8 billion in 2015, and around 2 hours of GPs’ time per day to review results.7 It is plausible that some of the improvements in specific outcomes, such as cancer diagnosis, that have been achieved over the same period3 could in part be linked to increased testing in general practice. For example, some observational studies have linked increased chest X-rays and endoscopies with improved outcomes for lung and upper gastrointestinal cancers, respectively.8 9 Yet, it seems highly uncertain that the huge costs and substantial harms resulting from increases in testing overall are warranted.
There is also little reason to believe more frequent testing has enhanced patient experience or contributed to enhanced shared decision-making. A UK study examining general practice records of 2572 patients who received blood tests showed that in 47% there was no documented evidence that test results had been communicated.10
Diagnosis relies on using the right test
To achieve a diagnosis via testing a clinician will typically have had to select the appropriate test for the suspected cancer. Avoidable diagnostic delay can occur when testing or referral that is recommended by guidelines in response to particular symptoms is not arranged.11 Where clinicians successfully arrange recommended testing, GPs need to consider other pitfalls that can delay diagnosis. Since symptoms of many different cancers overlap, placing too much emphasis on a negative test result for one cancer type may engender misplaced reassurance. For example, a faecal immunochemical test (FIT) could be one of several tests used in response to weight loss, but will not yield diagnosis if the cause was lung cancer. Particularly in the context of declining relational continuity of care, when patients may follow-up test results with a doctor who had not requested the original test and taken the initial history, there is a risk that these follow-up visits will only focus on conveying test results and providing reassurance rather than revisiting symptoms and reappraising if further testing is indicated. Even where the correct test has been selected, cancer tests have varying sensitivity, meaning patients who have false negative results must rely on the intuition of GPs to understand when to retest or refer despite negative tests.12 GPs must consider these factors to avoid pitfalls in the diagnostic process.
Non-specific blood testing in cancer diagnosis
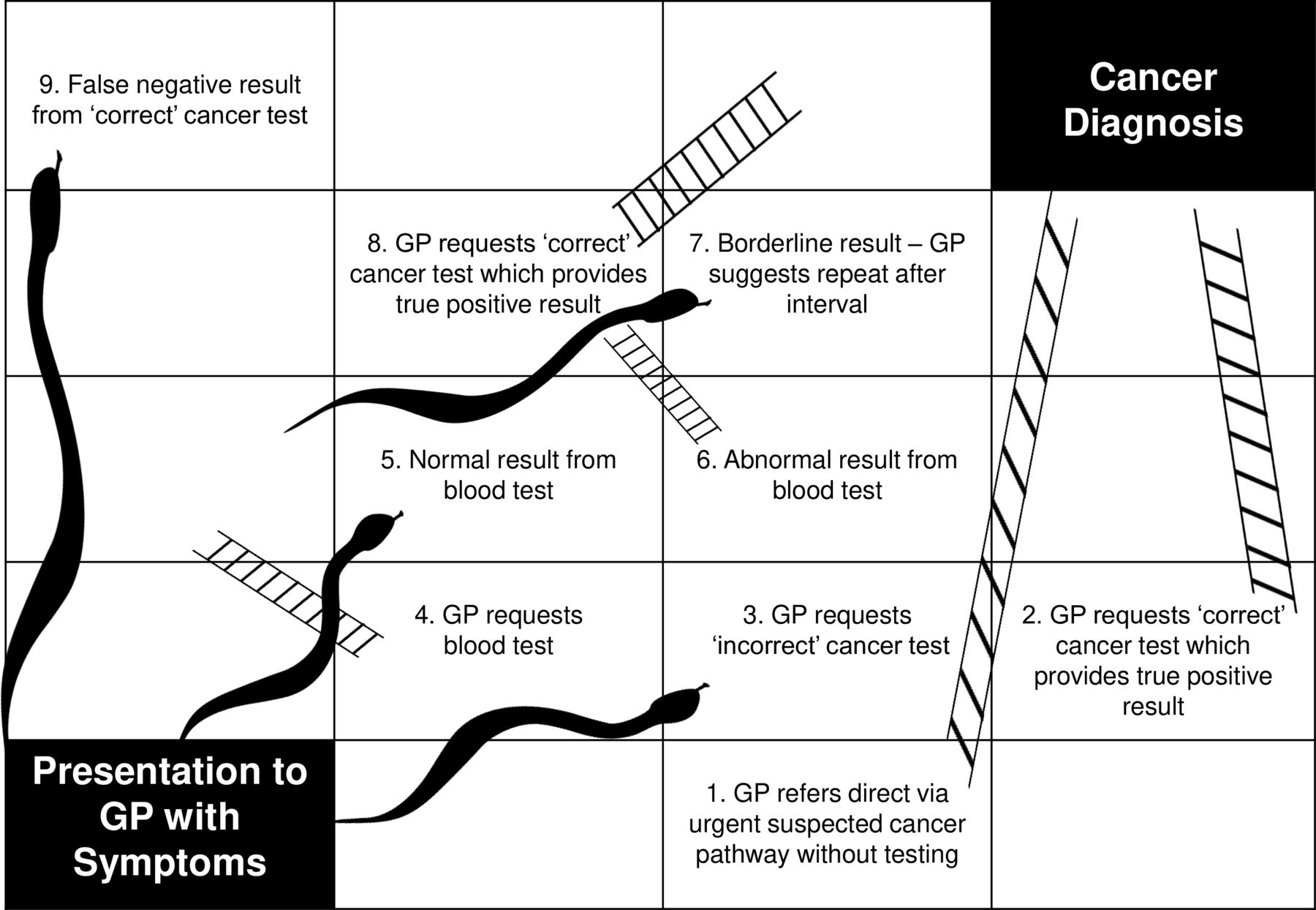
In the context of a clinician’s intuition (sometimes termed ‘gut feeling’) of serious underlying disease, abnormalities in non-specific tests may raise the suspicion of cancer sufficiently to prompt further testing (eg, chest X-ray prompted by thrombocytosis in a patient with tiredness) or lead to referral to diagnostic services commissioned to investigate for cancer in those with non-specific symptoms. However, the prospect that non-specific blood tests alone, such as inflammatory markers, FBC, liver function tests, and urea and electrolytes, can be expected to expedite cancer diagnoses within current practice is not at all assured (figure 1). In Australian general practice, increased blood testing is observed 7 months prior to colorectal cancer diagnoses and 6 months prior to lung cancer. The majority of those tested had abnormal results, but this in itself did not ensure prompt diagnosis, with the earliest abnormal results reported a median of 124 days before colorectal cancer diagnoses (IQR 32–229 days) and 190 days before lung cancer diagnoses (IQR 53–264).13

{kind=link}
Diagnostic snakes and ladders in general practice. This figure is based on the board game snakes and ladders, in which players roll a die to move their piece on the board. Landing on a square with a ladder allows the player to advance to a square nearer to the game’s objective, whereas landing on a snake means the piece needs to be moved back nearer to the start of the game. Diagnostic tests in general practice may expedite cancer diagnosis (box 2), achieve diagnosis indirectly (box 4 leading to boxes 6 and 8) or prolong the diagnostic process (box 3 or box 4 leading to boxes 5 and 7 or box 9). Direct referral without testing (box 1) is recommended for some cancer symptoms. ‘Blood test’ refers to non-specific tests such as full blood count or inflammatory markers. ‘Cancer test’ refers to triage tests used in general practice that can lead to referral for a specific suspected cancer such as chest X-ray (lung), cancer antigen 125 (ovarian), prostate-specific antigen (prostate), faecal immunochemical test (colorectal) or ultrasound (endometrial). GP, general practitioner.
That increased testing is observed prior to cancer diagnoses has led to the suggestion that ‘diagnostic windows’ exist within which diagnosis could potentially be expedited. Within current practice remains the challenge of identifying which patients who have abnormal blood tests warrant further testing or referral, but emerging evidence suggests that information from these common tests can be combined with symptoms to help stratify risk of cancer. For example, a raised inflammatory marker (C reactive protein) in patients with unintentional weight loss is associated with a risk of cancer diagnosis within 6 months of 8.3% (95% CI 6.3% to 10.7%) for men aged 40–49 compared with a baseline risk for the same age group reporting unintentional weight loss of only 1.1% (95% CI 1.0% to 1.2%).14 Important challenges would need to be overcome to operationalise such insights, including the need to consider multiple cancer types and the difficulty for GPs in recognising the risk conferred by the combination of symptoms and particular blood test results.
Blood tests are also not sufficient to rule out serious disease and may be a source of inappropriate reassurance, and possibly delay, since selection bias counterintuitively means that those with normal results have cancer risk that exceeds that of untested populations.15 For example, elevated platelets (thrombocytosis) is known to indicate an increased risk of cancer, but since doctors choose who to test based on clinical concern, the 1-year cancer risk for men aged 40 or over with normal platelet count is substantial at 4.1% (95% CI 3.4% to 4.9%).16
Do increased volumes of testing lead to improved outcomes?
Observational studies have shown that patients attending practices that undertake more cancer referrals have improved survival.17 Since referral for several cancer types is often contingent on concerning results from a triage test, such as FIT for colorectal cancer or cancer antigen 125 for ovarian cancer, it is plausible that increased levels of testing for those with particular symptoms could also lead to improved outcomes.
Practices that undertake greater volumes of testing with non-specific blood tests prior to a cancer diagnosis probably undertake more testing overall. Abnormalities are common in such tests,18 so identifying which patients with abnormalities require further investigation or referral may actually be more challenging in organisations which undertake more non-specific tests. While Akter et al demonstrated wide variation in testing, the existence of variation can not necessarily be assumed to be ‘unwarranted’. Substantial increases in testing,7 in addition to evidence that recommended testing often does not take place,10 suggest that complex patterns of overtesting and undertesting are present. As Akter et al point out, research to determine what should be considered optimal levels of testing to facilitate comparison between services is needed. The difficulty in persuasively linking different levels of testing to patient outcomes and cost-effectiveness will be a barrier to the interpretation of such research. Even if achieved, clinicians will continue to face the difficulty of decision-making for individual patients, a process which will continue to rely to some extent on subjective judgement. Such decision-making may not necessarily be improved by putative optimal levels of testing, since such benchmarking will be more informative when considering whole practice populations rather than for individual patients.
Understanding testing behaviour that benefits patients
Akter et al examined testing behaviour only in those who had been diagnosed with cancer and the reasons for testing were not available. However, high-volume testing particularly with non-specific blood tests used without clear understanding as to how their results should inform decision-making could well be considered an indicator of lower quality care. Given the costs of such testing and the poor patient experience resulting from inadequate communication about tests, broad-brush policies or interventions to increase testing in general are unlikely to yield benefit overall. By consuming additional resources, such measures might even lead to further deteriorations in access to care. Greater promise lies in focusing on developing interventions which increase specific investigations or referrals in appropriate patient groups, such as those with specific symptoms,10 19 alongside further research to identify associations between testing rates and patient outcomes.7
In the mean time, electronic health record vendors and bodies responsible for underused resources, such as England’s Diagnostic Imaging Dataset, should enable access to basic deidentified data on volumes of testing to facilitate reflection and understanding on how tests are currently being used within and between general practice services. In many instances, such data are collected but are not being effectively shared.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Professor Willie Hamilton for comments which helped them improve this editorial.
Footnotes
Contributors SB drafted the initial manuscript with revisions contributed by JW. SB is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SB has undertaken observational research examining lung cancer outcomes and volume of chest X-rays undertaken by general practices, which is currently under peer review.
Provenance and peer review Commissioned; internally peer reviewed.