Article Text

Statistics from Altmetric.com
Introduction
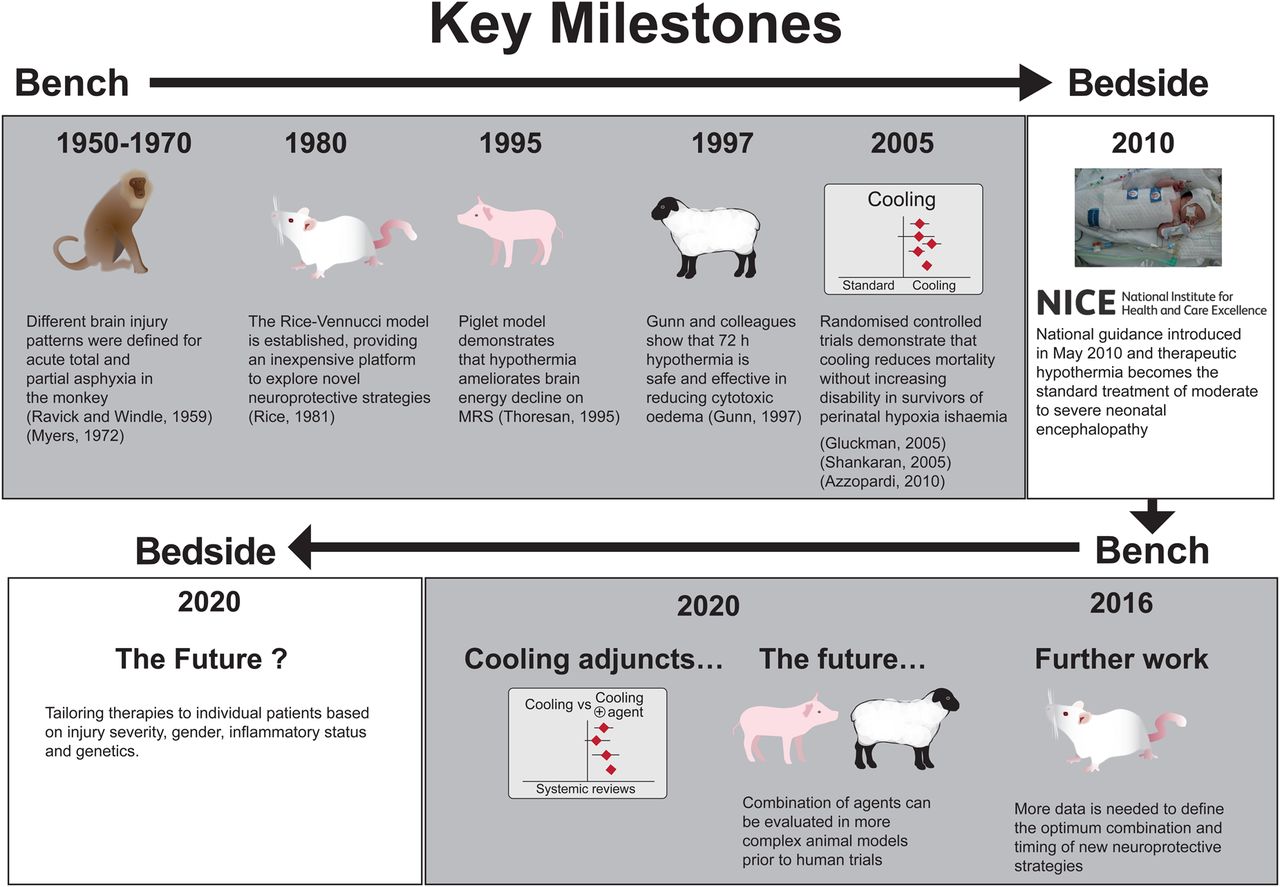
Neonatal encephalopathy (NE) is responsible for a significant burden of disability and death worldwide.1 The use of animal models in the study of perinatal hypoxia-ischaemia (HI) has a history of over 200 years; studies initially showed that the premature animal is more tolerant of asphyxia than a term animal, which is in turn more resistant to asphyxia than an adult.2 ,3 In the 1950s to the 1970s, studies in the primate model showed that the pattern of brain injury was clearly influenced by the severity and type of HI; these studies led to a description of two patterns of injury, namely acute total asphyxia4 and chronic partial asphyxia.5 In the last 30 years, progress was made by using animal models of NE to understand the timing and evolution of brain injury after HI. Triggered by the observation in human babies that brain energy metabolism on phosphorus-31 (31P) magnetic resonance spectroscopy (MRS) transiently recovered after birth and declined in the subsequent hours and days after birth despite intensive care support,7 studies in the newborn piglet8 and rat9 allowed pathophysiology and timing of events after HI to be studied more precisely than in the human fetus and neonate. Establishing the timing of this ‘secondary’ energy failure led to the concept that a window of opportunity existed whereby an intervention started after the primary insult could alter the trajectory of brain damage. The translation of the ideas and questions from bedside to bench moved therapeutic hypothermia from a research hypothesis to standard clinical care6 (figure 1). Optimising neonatal neuroprotection beyond therapeutic hypothermia requires further preclinical research with careful thought in using appropriate animal models to ensure efficacy, safety and translatability of the findings.

Key milestones. MRS, magnetic resonance spectroscopy.
Factors to consider for translation of animal studies to humans
There has been recent criticism of animal research10 because of overoptimistic conclusions and inadequate control of bias especially in relation to compounds that may, in reality, have little or no therapeutic potential. Magnesium sulfate, for example, has yielded disappointing results in the treatment of adult stroke11 in spite of promising animal data.12 In other cases, animal studies indicated futility, which was later borne out in clinical studies. For example, animal studies suggested the futility of deeper cooling following perinatal HI;13 this was seen in the randomised controlled trial of deeper and longer therapeutic hypothermia for NE, which was subsequently stopped due to safety concerns14 There are calls for more systematic reviews of animal studies and higher standards of research conduct and reporting.10
Dobbing and Sands used rates of brain growth to make cross-species comparisons and provided the foundation for the use of animal models to study neonatal brain injury.15 Such models need to take into account the timing of the brain growth spurt in relation to the injury and whether the animal is altricial, born at a relatively underdeveloped stage with many neurogenic events occurring postnatally (rodents, cats, dogs, rabbits, humans), or precocial, where the young are relatively mature and mobile from the moment of birth (guinea pig, rhesus monkey, piglet, sheep). This is important because cellular and regional vulnerability of the brain varies by developmental stage. Differences in brain complexity and white to grey matter ratios are also important factors.16 The rodent brain is lissencephalic with a much smaller proportion of white matter than in humans and a different focus of neurogenesis and timing of myelination. The rate of rodent maturation is accelerated compared with humans with each day of development in a rat corresponding to more than a week in humans.17 However, in studies of acute HI the timing of the cellular response to injury appears to be similar in rodents and humans. Examples of studies relevant to NE are summarised in table 1.
Advantages and limitations of commonly used animal models
Rodents
The Rice–Vannucci rodent model was established in 198118 and remains one of the most commonly used models of neonatal HI. Rat pup brains on postnatal days (P) 7 and 10 are developmentally similar to a 32-week gestation and term human infant, respectively. The classic Rice–Vannucci model involves unilateral carotid artery ligation and subsequent inhalation of 8% oxygen for 90 min. This model, however, has considerable injury variability and frequently produces cerebral infarction ipsilateral to the ligation, closely resembling a perinatal stroke rather than the global HI seen in NE.
Since its initial description, this model has been adapted for ongoing use, including younger and older rats and mice, showing the different vulnerabilities of different ages and species.19 Rodents in early postnatal life (P2–5) have been shown to have oligodendrocyte lineages with particular vulnerability to white matter injury, analogous to the extreme preterm infant and the development of periventricular leukomalacia.20 ,21
Sheep
Several models of in utero HI in fetal lambs have been developed, including umbilical cord occlusion at different gestational ages22 ,23 and bilateral carotid artery occlusion.24 In landmark studies in the 1990s, Gunn and colleagues used near-term fetal sheep to evaluate the pathophysiology of NE. Romney/Suffolk sheep between 117 and 124 days gestation (77–82% of full term) were instrumented with umbilical catheters, carotid artery occluders and intracerebral EEG probes before being returned to the intact uterus. Cerebral ischaemia was induced by carotid occlusion and confirmed by EEG. Cytotoxic cell swelling and accumulation of excitotoxins were observed. Gunn and colleagues later evaluated the efficacy of selective head cooling by inserting a scalp cooling coil at the time of surgery. They demonstrated that 72 h of hypothermia reduced cortical oedema, cortical infarction and neuronal loss.24
Non-human primate
Ranck and Windle4 and Myers5 developed monkey models of NE from the 1950s to the 1970s. Acute total asphyxia was induced at term by detaching the placenta at hysterotomy. Also, 11–16 min later the fetuses were delivered from their membranes and resuscitated.4 The pattern of injury was very similar to that seen in infants with basal ganglia and thalamus injury following a sentinel event.25 In the partial asphyxia model, full-term pregnant monkeys were ventilated with halothane to induce maternal hypotension and cause intrauterine fetal asphyxia. Each fetus was exposed to asphyxia for 1–5 h and then delivered, resuscitated and ventilated for 2 days. The pattern of injury was parasagittal, affecting the watershed areas.5 A primate model is currently in use to evaluate the efficacy of combined hypothermia and high-dose erythropoietin. This model involves prenatal cord occlusion for 15–18 min with extended MRI, MRS and neurodevelopmental follow-up to 9 months.26
Piglet
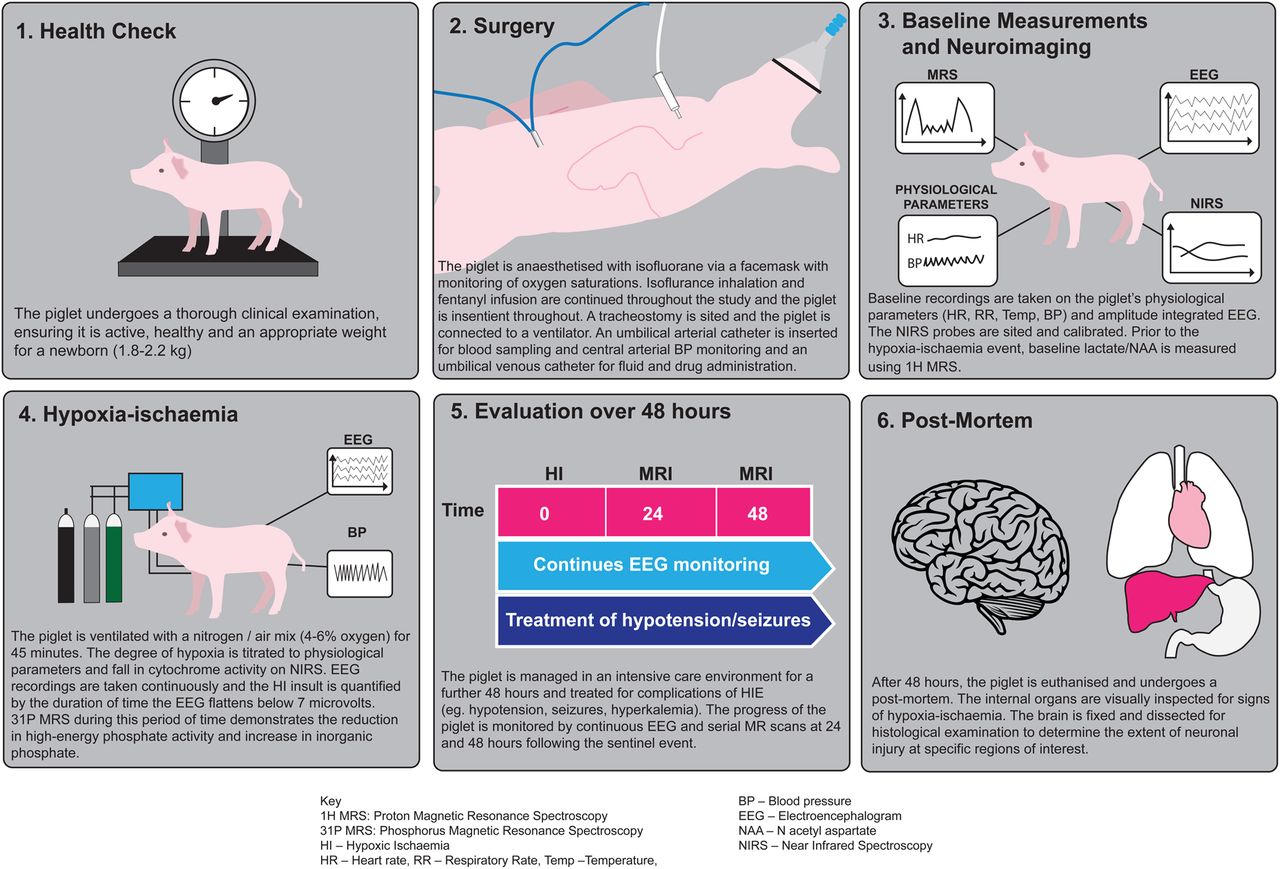
The piglet model of HI was developed in the early 1990s and has involved either a global hypoxic insult by inhalation of 4–6% oxygen28 or combined hypoxia with selective cerebral ischaemia. Until recently, our model at the University College London involved the latter, using bilateral carotid artery occlusion in combination with hypoxia over 25 min to assess efficacy and safety of neuroprotective interventions.13 ,29 ,30 We quantify the HI insult using 31P MRS, enabling standardisation across groups and smaller group sizes. A typical experimental protocol is shown in figure 2.

{kind=link}
{kind=link}
A piglet model protocol of perinatal asphyxia.
Piglets are a suitable non-primate model of NE due to their relatively large size and anatomical similarities to man. Unlike rodents, their brain size more closely reflects the white/grey matter ratio seen in humans and is at a comparatively similar developmental age at term.27 Piglets express similar neurometabolic changes on MRS and EEG abnormalities seen in asphyxiated term human infants. These similarities in outcome biomarkers assist the transition of this preclinical model to human clinical trials. Other outcome measures include assessing neuronal apoptosis, necrosis and inflammation using immunohistochemistry as well as gene expression studies.
Conclusion
Animal models have been central to the development of neuroprotective interventions for the human neonate in the last 25 years. The routine use of therapeutic hypothermia for moderate to severe NE was a significant milestone; however, further work is needed as, despite treatment, 25% of infants die and 20% of survivors have major neurodevelopmental sequelae including sensorimotor and cognitive deficits.31 Further work is needed to evaluate the efficacy of neuroprotective drugs both as single agents and in combination. Studies in small animal models (eg, rodents, mice) will be required to define the optimal combinations and timing of therapies before moving down the pathway of more complex ‘large’ animal models (eg, piglet, sheep) prior to human studies. Furthermore, there is increasing evidence from both preclinical32 and clinical studies33 ,34 that concurrent infection and inflammation has a significant deleterious effect on neurological outcomes in HI. Data from rodent studies suggest that therapeutic hypothermia may be less effective in infection-sensitised HI brain injuries.35 Therefore, there is an urgent need to further explore the relationship between infection, inflammation and HI. The ‘neuroprotection Holy Grail’ may lie in developing tools to rapidly distinguish pure HI from infection-sensitised NE, thereby allowing the initiation of patient-specific neuroprotective strategies to maximise clinical benefit.
Animal welfare is of course a priority in all preclinical research. All models aim to replace animal use where possible, refine the methodology and reduce animal numbers to a minimum (known as the three ‘R's). Through developing experimental models with clinical translation in mind and applying the same scientific rigour as human trials, we hope to safely and effectively implement new and innovative therapies to improve patient care in the future.
References
Footnotes
Contributors All authors have seen the final version and took part in the drafting of the manuscript. IL and NJR drew the figures.
Funding This work was undertaken at University College London Hospitals/University College London, which received a proportion of funding from the UK Department of Health's National Institute for Health Research Biomedical Research Centers funding scheme.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.