Article Text

Abstract
Background Toll-like receptor (TLR) agonists and radiation therapy hold promise for cancer immunotherapy. We conducted a phase I/II trial combining topical imiquimod (IMQ, a TLR-7 agonist) and local radiotherapy (RT) in patients with metastatic breast cancer accompanied by longitudinal transcriptional analysis of tumor biopsies.
Methods The primary objective of the trial (NCT01421017) was to assess systemic responses by immune-related response criteria (irRC) after an 8-week cycle of topical IMQ and concurrent local RT (cohort 1). An amendment to the trial added two cohorts, both received one dose of cyclophosphamide (CTX) administered 1 week before study treatment initiation, IMQ/RT/CTX (cohort 2) and RT/CTX control (cohort 3). Cutaneous metastases were prospectively assigned to treatment with IMQ and RT (area A) or IMQ alone (area B). Secondary objectives were safety (Common Terminology Criteria for Adverse Events criteria) and local response in skin metastases. In all IMQ cohorts, tumors were biopsied before treatment and at 2 and 3 weeks.
Results 31 patients were enrolled (n=12, n=12, and n=7, in cohort 1, 2, and 3, respectively), with 4 out of 24 patients in the IMQ cohorts showing systemic tumor responses (two complete responses (CR) and two partial responses (PR)). No objective responses were observed in the seven patients enrolled in the control arm (RT alone). The treatment was well-tolerated, no grade 4–5 treatment-related adverse events occurred and grade 3 AEs were manageable (anemia, local pain, and local ulceration, n=1 each). Local objective responses were observed in 19/24 (9 CR and 10 PR) and 5/24 (5 PR) in areas treated with combined IMQ-RT and IMQ alone, respectively (p<0.001). All 24 patients treated with IMQ underwent serial biopsies, and 84 samples yielded sufficient material for transcriptional analyses. These revealed that the presence of a T-helper 1 functional orientation of the tumor microenvironment paralleled by the downregulation of DNA-repair genes was associated with CR after IMQ+RT, but not after IMQ alone. No post-treatment activation of immune-effector functions was observed in stable and progressing lesions.
Conclusions Our findings support the safety and clinical efficacy of combining topical IMQ with local RT for recurrent breast cancer, with evidence of local and occasional systemic antitumor activity.
Trial registration number NCT01421017.
- Breast Cancer
- Toll-like receptor - TLR
- Combination therapy
- Radiotherapy/radioimmunotherapy
- Topical
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Gene expression data is available in the NCBI GEO repository under accession ID GSE282443: https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE282443.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Skin metastases of breast cancer and chest wall recurrences are difficult to successfully treat. When they progress, skin metastasis and chest wall recurrences of breast cancer are often compromising patient’s quality of life.
Novel therapies are warranted. Topical imiquimod (IMQ), a toll-like receptor agonist has been tested as an immunotherapy for this clinical setting. It has demonstrated to be safe and trigger some immune response. However, when given alone, it has limited efficacy.
WHAT THIS STUDY ADDS
The study was designed to exploit both cytocidal and immunostimulatory properties of radiotherapy (RT) with IMQ, in the attempt to demonstrate efficacy by converting skin metastases of breast cancer into an immunogenic tumor, thereby augmenting immune-mediated tumor rejection. Our study findings support the safety and clinical efficacy of combining topical IMQ with local RT for recurrent breast cancer, with evidence of local and occasional systemic antitumor activity. The association of a baseline immunologic constant of rejection (ICR) tumor signature with complete local response to IMQ+RT validates the ICR hypothesis, in the setting of metastatic breast cancer.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The significant and often durable local control of skin metastases with IMQ+RT is clinically relevant. In addition, extensive transcriptional immune analyses from serial tumor biopsies from all patients with skin metastases, provide insight into the tumor immune microenvironment and identify potential targets to develop more potent therapies.
Introduction
Toll-like receptor (TLR) agonists are attractive agents for cancer immunotherapy, included in the National Cancer Institute (NCI) immunotherapy priority rank list (TLR3, 4, 7/8 and 9 agonists).1 2 When used locally, the TLR7 agonist imiquimod (IMQ) creates an inflammatory environment that promotes tumor antigen cross-presentation and infiltration by effector cells.
Topical IMQ has been shown to induce regression of spontaneous breast cancers in the neu transgenic mouse model and it is Food and Drug Administration (FDA) approved to treat primary skin basal and squamous cell carcinomas.3 4 IMQ has an established safety profile and is commercially available. Because of their accessibility, chest wall recurrences and skin metastases of breast cancer are an ideal setting to study the immunological effects of local treatment, allowing for non-invasive monitoring of response and are easily accessible to be biopsied for mechanistic studies. Prior studies of topical IMQ as a single agent or combined with intralesional cytokines or systemic chemotherapy have shown promising results.5–8 However, topically delivered IMQ can also be combined with radiotherapy (RT) to treat the typically large, multifocal clinical presentation of a breast or chest wall recurrence. RT is commonly employed as a standard cytocidal modality to treat locally recurrent breast cancer. It has demonstrated multiple pro-immunogenic effects, including enhanced tumor immunogenicity, recruitment of effector T cells, and synergy with various immunotherapy approaches, including TLR agonists.9–15 Optimal dose/fractionation regimens to best exploit these effects of RT were elucidated in preclinical studies16 and have been validated in clinical trials.17 18
We previously demonstrated that local RT potentiates topical IMQ treatment resulting in complete tumor regression and improved survival in the poorly immunogenic TSA murine mammary carcinoma model.12 In this preclinical model the combination therapy enhanced T-cell-mediated inhibition of both treated and unirradiated tumors (abscopal effects). Immune memory responses were improved with the addition of low-dose, immunomodulatory cyclophosphamide (CTX).12 Based on these results we conducted a clinical trial to evaluate the efficacy of the combination of IMQ and RT. We report the safety as well as the efficacy of this combination, with and without CTX. Importantly, the trial enabled the analysis of serial fine needle aspiration (FNA) tumor biopsies from patients, to explore dynamic changes associated with the immune-mediated tumor responses in breast cancer.
Patients and methods
Eligibility
Patients were eligible for the trial if they had biopsy-confirmed breast cancer with measurable disease by RECIST V.1.1. To be eligible for the IMQ-treatment arms their skin metastases needed to be amenable to local treatment and to serial FNAs. Age >18 years, ECOG performance status 0–2, adequate organ function and written informed consent were required. Patients were eligible regardless of tumor receptor status. Estrogen receptor (ER) and progesterone receptor (PR) positivity was defined as at least 10% of carcinoma cells staining by immunohistochemistry (IHC), human epidermal growth factor receptor (HER)-2 positivity was defined as either IHC 3+ or HER2 gene amplification by fluorscence in situ hybridization (FISH.) Exclusion criteria included concurrent brain metastases, unless treated and stable >4 weeks, concurrent treatment with other investigational agents or local therapy (RT, high-potency corticosteroids, intralesional therapy, laser therapy or surgery). A biopsy to the target area within 4 weeks or superficial hyperthermia to the target area within 10 weeks prior to the first dosing of the study agent were permitted. Continuation of the most recent systemic therapy (endocrine, chemotherapy and HER2 biologics) was permitted if no tumor response had occurred in the prior 8 weeks and the regimen was considered safe when concurrently used with study treatments.
Study design and objectives
The trial was approved by the New York University and Cornell University institutional review boards and registered with ClinicalTrials.gov (NCT01421017). The study was designed as a non-randomized open label, multicohort Phase II trial following a brief Phase I run-in (online supplemental file 2). The Phase I portion was conducted to allow dose optimization in the event of unanticipated adverse events (AEs) and included six patients, following a standard 3+3 design.
Supplemental material
The primary objective of the trial was to estimate the systemic antitumor response (partial response (PR) and complete response (CR) by immune-related response criteria (irRC) after an 8-week cycle in patients receiving topical IMQ and concurrent local RT administered to cutaneous metastases of breast cancer, with a planned sample size of 25 patients in the Phase II portion. Secondary objectives were to estimate the local antitumor response in IMQ and IMQ+RT areas, to evaluate safety by CTCAE criteria V.5.0, and to examine the immune signature in metastases treated with IMQ with and without RT. In May 2014, the trial was amended to close the IMQ/RT cohort (cohort 1) after 12 patients were treated, based on emerging preclinical evidence that the addition of immunomodulatory CTX provides additional benefit.19–23 The trial was then amended to continue with two concurrent Phase II arms to evaluate the combination of CTX/IMQ/RT (cohort 2) along with a concurrent control of CTX/RT (cohort 3) and enrolled an additional 12 and 7 subjects, respectively.
For patients enrolled onto the IMQ-treatment arms (cohorts 1, 2), skin metastases were divided into two areas (area A: IMQ and RT) and (area B: IMQ only) for differential treatment and assessment (online supplemental figure 1). The size and location of the area of cutaneous metastases assigned to RT (area A) was designed taking into consideration previously irradiated areas. All cutaneous metastases outside of area A were included in area B. In patients without distant measurable disease present on scans an additional area, designated as control area was contoured, and left untreated. Patients completed the study with the week 9 visit when they were assessed for response. All patients were followed with annual follow-up visits, until death. Additional treatment cycles (with an identical 8-week schedule) were permitted for responders, with RT targeted to a different area.
Supplemental material
Topical IMQ to cutaneous metastases was self-applied 5 days per week for 8 weeks.
At baseline, skin metastases were photographed, outlined on medical graphing paper based on visible and/or palpable borders and IMQ dose was calculated based on surface area (see below, IMQ regimen). RT started on the day before the first IMQ application and was given in five fractions of 6 Gy each, over the course of 10 days (Monday-Wednesday-Friday-Monday-Wednesday). One dose of intravenous CTX at 200 mg/m2 was administered 1-week prior to starting study treatment in cohorts 2 and 3.
Radiation therapy: a direct electron field or a conformal three-dimensional RT set-up were used to target the area to be irradiated (area A, figure 1). RT was administered to a total dose of 30 Gy given at five fractions of 6 Gy each on days 1, 3, 5, 8 and 10 (M-W-F-M-W). This is both a dose and fractionation regimen we have shown to be immunogenic in murine breast carcinoma treated with RT and immunotherapy12 16 and a standard palliation regimen commonly used in re-treatment of breast cancer, where it has shown an acceptable toxicity profile in previously irradiated patients.24–26 After simulation, the target was outlined in the Eclipse planning system. The prescription aimed to deliver at least 95% of the dose to the identified target. Electron beam and/or photon energy were allowed. No bolus was applied, unless required to modify electron beam dose delivery, to assure adequate coverage of the target.

Transcriptomic profiles of pretreatment (baseline) samples. (A) Volcano plot of differentially expressed genes between baseline CR and non-CR (PR+SD+PD) samples in site A; p values are from one-way analysis of variance test and false-discovery rate (FDR) is calculated using the Benjamini-Hochberg method; FDR<0.05 was used as cut-off. Representative immunomodulatory genes are labeled. (B) Hierarchical clustering heatmap of individual pretreatment samples based on differentially expressed genes between site A CR and non-CR samples; the expression of these genes is then portrayed in site B samples. (C) The z-scored values of representative immunomodulatory genes differentially regulated (FDR<0.05) between baseline CR and non-CR samples in site A are displayed in a heatmap. The expression of these genes is then portrayed in site B lesions. (D) Functional annotation analysis by Ingenuity Pathway Analysis of the differentially expressed genes (FDR<0.05) between baseline CR and non-CR samples (A). The top 30 canonical pathways are represented. site A: samples treated with radiotherapy+imiquimod; site B: samples treated with imiquimod alone. CTX: samples from patients treated with cyclophosphamide; non-CTX; samples from patients not treated with cyclophosphamide. Response: CR, complete response; CTX, cyclophosphamide; PD, progressive disease; PR, partial responder; SD, stable disease.
IMQ regimen: the choice of a 5 days/week treatment frequency was based on the FDA-approved regimen for superficial basal cell carcinoma, and the report in two patients with breast cancer who experienced a CR at 6 months, after continued IMQ use.27 The treatment dose was determined by tumor area: one single-use packet of IMQ 5% (250 mg cream) per day was used for tumors <100 cm2, and additional packets were added for each additional 100 cm2 area, not to exceed six packets/day. The protocol included a within-patient de-escalation of IMQ application frequency, in case of toxicity. To monitor and encourage compliance, patients kept a medication diary and received weekly phone calls from the study team.
CTX regimen: CTX dose was 200 mg/m2 based on previous literature.19 28
Response assessment
All patients completing the assessment at 9 weeks were considered evaluable for response. For patients undergoing multiple cycles of therapy responses were recorded after each 8-week cycle, with the best objective response rate (ORR) used for final determination of response.
Local antitumor response was determined for both treatment areas: (1) irradiated metastases, which received IMQ and (2) non-irradiated metastases receiving only IMQ. Tumor surface areas (regions of interest in cm2) were calculated within ImageJ29 after outlines were recorded onto transparent paper and transferred via flat-bed optical scanner into the ImageJ program. As skin lesions could be numerous and/or confluent with irregular borders, the criteria for local response assessment were based on European Organization for Research and Treatment of Cancer definitions for chest wall tumors,30 modified from those established for Kaposi’s sarcoma with skin involvement.31 These response criteria have proven useful in our prior trial for chest wall recurrences.5 Local response, evaluated at week 9, was defined as PR or clinical complete response (CCR) in treated lesions.
The systemic/abscopal antitumor response was evaluated in untreated measurable lesions (skin or distant metastases, if present) by immune response criteria (irRC), specifically adapted for immunotherapies from RECIST criteria.32 33
Immune profiling of tumor microenvironment in patient samples
The immunologic constant of rejection (ICR) described by Wang et al 34 results from a coordinated activation of the innate and adaptive immune responses, including interferon (IFN)-stimulated genes. ICR was validated in IMQ-mediated tumor rejection in basal cell carcinoma.4 The ICR was further refined and harmonized into a fixed 20-gene panel, showing prognostic significance in different cancer types such as colon cancer,35 melanoma,36 bladder cancer,37 breast cancer,37 38 neuroblastoma39 and soft-tissue sarcoma.40 The ICR also correlates with response to immunotherapy across multiple cancer types, including melanoma,36 and non-small-cell lung cancer.41
ICR reflects the gene expression in three main pathways: for CXCR3/CCR5 chemokines: CXCL9, CXCL10, CCL5; for Th1 signaling: IFNg, TBX21, IL12B, STAT1, IRF1 and for effector functions: PRF1, GZMA, GZMB, GZMH.
FNA biopsies were obtained serially from the same lesion in area A (IMQ+RT) and B (IMQ) at baseline, 2 and 3 weeks. At the time of FNA cytological examination was performed by a pathologist (PGL) to confirm that tumor tissue was collected. As FNAs are minimally invasive biopsies they can be safely performed in irradiated areas; serial sampling allows the delineation of dynamic changes associated with the inflammatory switch in the tumor with minimal perturbation of the tumor microenvironment.42 43 SOPs were followed for FNA, sample processing and molecular profiling as established previously.42–44 In brief, two consecutive FNA passages are obtained with a 23 Gy needle, for each area, A and B. The first aspiration was used for cytospin preparation and assessment of cellular content. The second aspiration was re-suspended in 10 mL cold RPMI media (without supplement of antibiotics and serum), and centrifuged at 300×g for 5 min at 4°C. The supernatant was discarded and the cell pellet re-suspended in 5 mL of ACK lysing buffer and incubated at 37°C for 5 min. After centrifugation at 300×g for 7 min at 4°C, the supernatant was discarded and the cell pellet was re-suspended in 1 mL of cold RPMI, transferred to a 1.5 mL Eppendorf tube and spun at 300×g for 5 min in a microcentrifuge.
For long-term storage, after discarding the supernatant, pellets were resuspended in 50–100 µL of RNA protector cell reagent and stored at 4°C for 4 hours before transfer to –80°C storage. For short-term storage and immediate RNA isolation, cell pellets were resuspended in 700 µL of TRIzol. Total RNA was extracted with the Qiagen RNA extraction kits (Catalog number: 217004/74104). Quality and quantity were estimated using NanoDrop (Thermo Scientific, Waltham, Massachusetts, USA) and Agilent 2100 Bioanalyzer (Agilent Technologies, Palo Alto, California, USA). First-strands and second-strands complementary DNA (cDNA) were synthesized from 30 ng of total RNA by using Nugen Ovation Pico WTA System V.2 (Nugen technologies, San Carlos, California, USA) and following manufacturer’s instructions. cDNAs were fragmented and biotinylated by using Nugen Encore Biotin Module (Nugen technologies, San Carlos, California, USA) and hybridized to the GeneChip Human Gene 1.0 ST Arrays (Affymetrix, Santa Clara, California, USA). The arrays were washed and stained on a GeneChip Fluidics Station 450 and scanned by GeneChip Scanner 3000 (Affymetrix, Santa Clara, California, USA).
Bioinformatics analysis
Data were imported into Partek and normalized using the Robust Multi-Chip Average method, probe sets were aggregated into genes and log2-transformed. All subsequent analyses were performed in the R program (V.4.1.3, RStudio). The expression files were then matched by probe ID to gene symbols using the annotation database from library: “hugene10sttranscriptcluster.db”.
Differentially expressed genes and pathway analysis
Differentially expressed transcripts among classes in comparisons were detected by analysis of variance (ANOVA) modeling or paired t-tests for longitudinal analyses at different time points. The FDR (false discovery rate) method of Benjamini-Hochberg was used to provide adjusted p values to account for the multiple statistical tests. Gene Ontology analyses were performed using Ingenuity Pathway Analysis (QIAGEN Bioinformatics). Significant transcripts based on the appropriate cut-off and a fold change (FC) were used to select transcripts for pathway analysis. The proportion of upregulated and downregulated transcripts was represented. The z-score was used to indicate the direction and significance of the pathway activation. Transcripts from the top three pathways in each comparison group were plotted in the corresponding heatmaps.
Leukocyte enrichment score analysis
To estimate the enrichment of various cell types, gene expression deconvolution analyses were performed with single sample Gene Set Enrichment Analysis (GSEA) implemented in the “GSVA package” using 32 specific signatures (990 genes: online supplemental table 1; T cells, CD8 T cells, cytotoxic cells, Th1 cells, Tcm, Tem, T helper cells, TFH, Th2 cells, Th17 cells, Tgd, Treg, NK cells, NK CD56bright cells, NK CD56dim cells, NKT, B cells, macrophages, monocytes,45 DC, iDC, pDC, mDC, neutrophils, eosinophils,46 mast cells, ICR,35 37 38 47 TIS,48 hallmark pathways of IFN signaling, IFN alpha (IFNA), IFN gamma (IFNG), immunogenic cell death (ICD), available from the GSEA Molecular Signatures Database (http://www.gsea-msigdb.org/gsea/msigdb/collections.jsp) were used to estimate the abundance of the corresponding populations. Differentially expressed enrichment scores between pretreatment and post-treatment were detected by ANOVA modeling or paired t-test as appropriate. Heatmap analysis was performed by using the library “Complexheatmap” (https://academic.oup.com/bioinformatics/article/32/18/2847/1743594), Volcano plot and line plot of significant genes/enrichment score were performed by using ggplot (V.3.5.1) from library “ggplot2”.
Statistical considerations
31 patients with metastatic breast cancer enrolled and were treated in this trial. Each arm was evaluated independently (12 in IMQ/RT, 12 in IMQ/RT/CTX, 7 in CTX/RT). The Phase II trial was originally designed to enroll 25 patients in a single-stage optimal design to test the hypothesis that the primary endpoint of interest, systemic tumor response (CR+PR), is less than or equal to 5% versus the alternative hypothesis that the rate is greater than or equal to 30% with alpha=0.05 and power of 80%. If three or fewer patients achieved a systemic CR or PR, the combination would be rejected for further study. The actual alpha level is 0.034; power is 97% (calculations from PASS, NCSS, 2008, J. Hintze, Kaysville, Ut). As described above, due to new data on CTX, the IMQ/RT cohort was closed and two subsequent cohorts were added (each containing CTX). The 2014 amendment to evaluate CTX-containing Phase II cohorts employed an optimal single-stage design with 15 patients planned in each of these two cohorts separately to test the hypothesis in each cohort that the primary endpoint of interest, systemic tumor response (CR+PR), is less than or equal to 10% versus the alternative hypothesis that the rate is greater than or equal to 40.1% with alpha=0.05 and power of 80%. The actual alpha level is 0.012 and the exact CI for 0.401 is 0.164 to 0.678. (calculations from PASS, NCSS, 2008, J. Hintze, Kaysville, Ut). Cohort 2 closed after only one systemic response was observed in 12 patients, and cohort 3 closed with no systemic responses in 7 patients.
Across the trial and within each study cohort, characteristics of patients and their disease status at study entry are summarized using descriptive statistics (including means, SD, quantiles) and graphical displays (eg, boxplots) for quantitative variables and frequency and percentages in specified categories for qualitative variables. ANOVA tests and Fisher’s exact tests were used to compare the distributions of quantitative and qualitative variables among the three cohorts, respectively.
Specific adverse effects were summarized with the number of patients who had possibly, probably, or definitely experienced the specific AEs (highest grade per patient). The maximum grades of the adverse effects (highest grade of all adverse effects experienced by each patient) were also summarized with the number of patients who had possibly, probably, or definitely experienced them.
Clinical response rates (CR, PR, stable disease (SD), progression of disease (PD) for systemic, local area A (irradiated lesion), and local area B (non-irradiated lesion) were estimated in each group and are provided with exact 95% Clopper-Pearson CIs. McNemar χ2 tests were conducted to compare the proportion of ORR between areas A and B within a patient for the CTX+IMQ+ RT and IMQ+RT cohorts individually and combined.
Gene expression analyses. Exploratory gene expression analyses were planned to evaluate differentially expressed transcripts using the Affymetrix Human Gene ST 1.0 Array to distinguish patients with CR and non-CR reference to baseline expression levels. Two sample t-tests with Benyamini-Hochberg (BH) FDR adjustments for multiple comparisons were conducted. Differentially expressed genes (DEGs) were also selected between CR and non-CR patients with FDR<0.1 using the CTX+IMQ+RT data. Hierarchical clustering heatmaps were developed based on these selected DEGs that distinguished between CR and non-CR patients for the CTX+IMQ+RT group only (and also for the CTX+IMQ+RT and IMQ+RT groups combined). Furthermore, from these selected DEGs, we identified the ICR genes and then performed additional hierarchical clustering for the same groups as above. Two-sided paired t-tests were also used to explore the differences in the changes in gene expression over time from baseline to T2 (or T3) between site A and site B.
Data availability
The data is available in the NCBI GEO repository under accession ID GSE282443: https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE282443.
Results
31 patients were enrolled into the trial, 29/31 with proven distant metastasis, 2 patients had chest wall recurrence only. 24 patients with chest wall or skin involvement received topical IMQ and local RT (12 patients with and 12 patients without low dose intravenous CTX). Seven additional patients without chest wall or skin metastases were treated in the control arm of RT to one metastatic site combined with low-dose CTX. The consort diagram in online supplemental figure 2 details the three cohorts as well as treatment assignment. Tables 1 and 2 summarize baseline patient demographic and tumor characteristics by treatment arm. The distributions across the three arms did not significantly differ. Overall, the median age was 60 (range 41–84). 64.5% of the patients were white, 19.4% were Asian and 16.1% were African American. 58%, 23% and 19% of patients had ER-positive, HER2-positive and triple-negative tumors, respectively.
Patient demographic and tumor characteristics at baseline, and treatment history (n=31, qualitative variables)
Patient demographics, tumor characteristics at baseline, and treatment history (n=31, quantitative variables)
Safety
Tables 3 and 4 summarize the AEs that were at least possibly related to study treatment by treatment group. 22 of 31 patients (71%) experienced at least one treatment-related AE, the majority being grade 1 and 2 events. As expected, frequent local IMQ-related reactions included dermatitis, pain and ulceration. The only grade 3 AEs possibly related to treatment were anemia (one patient, at week 1, recovered without intervention), local tumor pain (one patient, at week 2, recovered with IMQ treatment interruption), local skin infection (one patient, at week 2, resolved without treatment interruption) and local tumor ulceration (one patient, at week 6, persisted despite treatment discontinuation). No grade 4 or 5 treatment-related AEs were observed and no patients discontinued the trial because of side effects. 8 of the 24 patients treated with IMQ required treatment interruption and/or dose reduction due to AEs (local pain=4, local ulceration=3, fatigue=1).
Number of patients with possibly, probably, or definitely related specific adverse events (highest grade per patient shown) (IMQ+RT: n=12; CTX+RT: n=7; CTX+IMQ+RT: n=12)
Number of patients with maximum grade (highest grade of adverse events per patient) of possibly, probably, or definitely-related adverse events
Antitumor efficacy
The protocol-specified treatment duration was 8 weeks (one cycle), with the option for additional cycles in case of response. 26 patients completed at least one cycle of therapy and 5 patients received a second cycle; 5 patients discontinued treatment during the first cycle due to disease progression (table 1).
Systemic tumor responses were observed in 4/24 patients (ie, 17% with 95% CI: 5%, 37%) who received combination therapies with IMQ (table 5). These consisted of two CR (one each in cohort 1 and 2) and two PR (both in cohort 1). Responses were observed only in skin, soft tissue or lymph nodes, not visceral organs. Online supplemental figure 3 demonstrates a patient with complete and durable remission of treated and untreated metastases. No objective responses (0/7) were seen in patients treated on the cohort 3 (CTX/RT).
Efficacy analysis: response rates by treatment arm
Local tumor responses (only assessable for the 24 patients with skin involvement and treated with IMQ) were frequent at site A (IMQ/RT), with both PR and CR seen in 19/24 patients (79%, 95% CI: 58%, 93%) with 9/12 patients (75% with 95% CI: 43%, 95%) in the CTX+IMQ+ RT group and 10/12 patients (83% with 95% CI: 52%, 98%) in the IMQ+RT group. Metastases treated with topical IMQ alone (site B) showed partial regression in 5/24 patients (21%, 95% CI: 7%, 42%) with 1/12 patients (8% with 95% CI: 0.2%, 38%) in the CTX+IMQ+RT group and 4/12 (33% with 95% CI: 10%, 65%) patients in the IMQ+RT group: no CRs were observed. The addition of low-dose CTX did not increase local response rates.
Local ORR was significantly higher in area A than that in area B (McNemar’s p<0.001), indicating that the addition of local RT improved the response to IMQ (table 5). No responses were observed in area B in patients without response in area A.
Tumor microenvironment analysis
All 24 patients treated with IMQ underwent serial FNAs. Biopsies were obtained at baseline, 2 and 3 weeks from both sites A and B. 84 samples were sufficient for transcriptional analysis (online supplemental table 2). Within this subset, four patients achieved CR (all local, in field).
Baseline comparison of gene expression between sites A and B
No differences were seen in baseline gene expression when comparing sites A and B within patients (with BH adjusted p values≤0.05).
Baseline differentially expressed genes and functional analysis associated with CR
By applying an FDR of 0.05, 2,195 DEGs were detected by comparing CR versus non-CR (PR+SD+PD) samples (figure 1A). This list of genes precisely segregates site A samples according to the clinical response (figure 1B). Interestingly, nine samples in site B displayed a transcriptional profile like the ones of site A CR samples. Among the four patients achieving CR, three of them had similar transcriptional profile in both site A and site B (Pt27, Pt6, and Pt20) while the profile of Pt22 dramatically differed between site A and B. An additional six samples in site B were molecularly similar to the ones of site A CR, including two unpaired samples (for which no material was available from the site A counterpart) and four site A-matched samples (Pt 16, Pt 17, Pt 30, and Pt 23).
Among the genes with the top FC for the comparison of CR versus non-CR samples, several transcripts associated with natural killer (NK) cells and T/NK cytotoxic functions were present, including GNLY, NKG7, GZMA and GZMB (figure 1A,C). Other immune-related genes upregulated in CR samples include TNF, TLRs, cytokine receptor (eg, IL6R, IL17RA, IL2RB, IL10RA, IL7R, IL5RA and IL118R1), IFN-signaling genes (eg, IRFs and STAT4), genes related to inflammasome (NLRPs, NLRC4 and IRAK3), B cell and T-cell markers (CD19, CD3s, CD27, ZAP70), monocyte-macrophage markers (CD14, TREM1), Th1 transcription factors (TBX21), and CCR5 chemokines (CCL4-5) (figure 1C).
The list of 2,195 DEGs was applied for functional analysis using Ingenuity Pathway Analysis. The large majority of enriched pathways comparing site A baseline samples from patients achieving CR with the ones that did not were related to immunologic processes (figure 1D), with the top canonical pathways being related to NK cells and Th1/Th2 activation. Conversely, downregulated pathways in baseline CR samples were associated with DNA-damage repair processes (eg, mitotic role, mismatch repair, and BRCA pathway, figure 1D), including MLH1, MSH2, MSH6, FANCL, FANCM, PARP1 and PMS2 genes. However, archived tumors available from two of the patients with CR were tested, all four stains MLH1, MSH2, MSH6 and PMS2 show preserved nuclear staining in the tumor cells, indicating microsatellite stable status.
Single sample Gene Set Enrichment Analysis
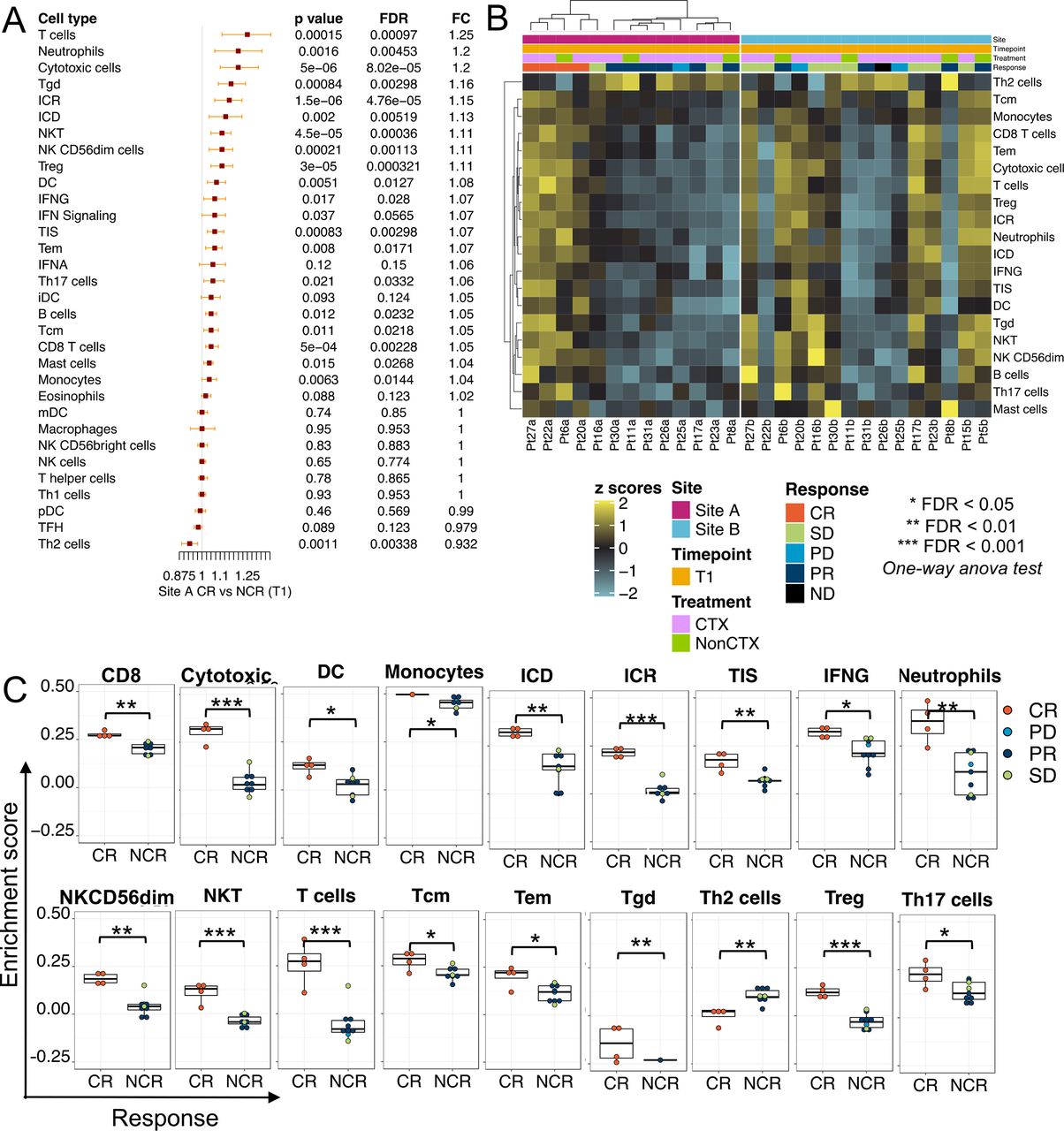
We then proceeded to compare Arm A CR versus non-CR baseline samples in terms of the functional orientation of the tumor microenvironment, by estimating leukocyte subset enrichment scores (LSES) and the enrichment of representative immunologic pathways such as IFNA signaling, IFNG signaling, ICD and signatures previously associated with responsiveness to immunotherapy (ICR and tumor inflammation signature, TIS). Among the 32 immune traits analyzed, 20 were differentially expressed in CR versus non-CR samples at an FDR of 0.05 (figure 2A,B).

Leukocyte subpopulation and immune signature enrichment scores of pretreatment (baseline) samples. Differences of leukocyte subpopulation and immune signature enrichment scores were estimated by single sample Gene Set Enrichment Analysis. (A) Forest plots based on fold changes of leukocyte subpopulation and immune signature enrichment scores in site A CR versus NCR samples. Fold changes (FC) are calculated as the ratio of anti-loge of the enrichment scores. FC>1 consists of increased enrichment score in pretreatment CR versus pretreatment NCR samples. P values are from one-way analysis of variance test and false-discovery rate (FDR) is calculated using the Benjamini-Hochberg method. (B) The enrichment scores of differentially regulated immune signatures and leukocyte subpopulations between baseline CR and non-CR samples in site A are displayed in a heatmap. The expression of these enrichment scores is then portrayed in site B lesions. (C) Box plots of differentially expressed immune signature and leukocyte subpopulation enrichment scores between site A complete responders (CR) and non-complete responder samples (NCR=PR+SD+PD) related to panel A. PD, progression of disease; PR, partial response; SD, stable disease.
Among LSES, T cells LSES showed the highest FC in CR versus non-CR samples, followed by neutrophils and cytotoxic LSESs (figure 2A,B). ICR enrichment score was the top upregulated immunologic pathway (figure 2A,B). Other LSES higher in CR versus non-CR include Tcm, Tem, CD8 T cells, T reg, DC, Tgd, NK CD56 dim, B cells, Th17 cells, and mast cells. Interestingly, Th2 cell LSES were downregulated in CR samples (figure 2B). Differences in global transcriptomic profile between matched lesions within the same patients were mirrored in terms of LSES and immunologic signaling enrichment score. Individual samples LSES are plotted in figure 2C.
Longitudinal analysis
When paired analysis across the same treatment group was performed at different time points (ie, T2 vs T1, T3 vs T1, and T3 vs T2) within Arm A and B, only a few genes were differentially expressed using a nominal p value of 0.005 (29, 106, and 88 in Arm A, and 24, 63, and 23 in Arm B, respectively, online supplemental table 3), with no genes below the FDR p value cut-off of 0.05. In fact, the major factor associated with time-dependent changes was the clinical response.
When analysis at different time points based on clinical response applied, clear differences emerged in immune-related genes (figure 3A) and LSES or immune-related pathway enrichment scores (figure 3B,C and online supplemental figure 4). CR samples, characterized at baseline by a high level of immune activation followed by immune oscillation, contraction at T2 and reactivation at T3. SD samples showed modest changes following treatment, limited to an increase of macrophage LSES and a decrease of Th2 LSES, while LSESs and immunologic pathway enrichment scores, including IFNA and IFNG signaling, tend to decrease at the two post-treatment time points in the PD samples.

{kind=link}
{kind=link}
{kind=link}
Post-treatment immune perturbations according to clinical response. At each time point and within each response category, differentially regulated immunomodulatory genes (A) and leukocyte subpopulations or immune signatures identified in pretreatment site A CR versus non-CR comparison are averaged (site A and B combined) and portrayed at different time points; T1: pretreatment, T2: 2 weeks post-treatment, T3: 3 weeks post-treatment. (C) Time-dependent coherent changes of immune signature and leukocyte subpopulation enrichment scores in combined site A and site B samples are represented within each response category as aggregate scores. *=p<0.05 and **=p<0.01 in T3 versus T1 and T2 versus T1 comparison; *=p < 0.05 and **=p<0.01 in T3 versus T2 comparison; unadjusted p values. The color of the asterisk is based on each response category. CR, complete response; PD, progression of diseases; PR, partial response; SD, stable disease.
Conversely, a sharp increase in IFNA and IFNG signaling, ICR, TIS, with a dramatic and progressive increase of B cells, neutrophils, DC, iDC, Th1, Th17 NK CD56 dim, T-reg, LSES and a decreased Th2 LSES was observed in PR samples. Similar trends were detected when the analysis was stratified by treatment modalities.
Discussion
This trial examined a novel combination of two local modalities (IMQ, a TLR-7 agonist administered topically, and focal RT) for the treatment of metastatic breast cancer. The combination therapy was well-tolerated; expected local side effects due to IMQ were transient, often preceding tumor response.
The study was designed to exploit both cytocidal and immunostimulatory properties of RT with IMQ, to convert skin metastases of breast cancer into an immunogenic tumor, thereby augmenting immune-mediated tumor rejection. RT enhances tumor infiltration by immune cells and antigen cross-presentation by inducing an ICD, and can also enhance recognition of cancer cells by effector T cells.9 49 TLR7 stimulation via the topically applied agonist IMQ induces dendritic cell activation and antigen-specific immunity to co-administered tumor antigens50 but also has profound immunomodulatory effects on the tumor microenvironment,51 leading to immune-mediated clearance of primary skin and mucosal malignancies4 as well as metastases.52 53 This study was based on our promising prior clinical and preclinical data in breast cancer.5 12
Similar to Brody et al in a trial of intralesional TLR-9 agonist and local RT in patients with lymphoma,13 we observed abscopal effects of this combination. The patient shown in online supplemental figure 3 as an example had poorly differentiated, triple-negative breast cancer with skin-only metastases. She underwent two cycles of the IMQ+RT treatments without other concurrent therapies and experienced complete remission of treated and untreated skin metastases, which never recurred. However, 6 months after completion of the trial, while off therapy, she developed lymph nodal recurrences and later died of disease progression.
We asked whether IMQ treatment was associated with a tumorous transcriptional profile of immunological rejection (ICR, immunologic constant of rejection) predicting CR as shown previously in patients with basal cell carcinoma.4 The analyses of specimens collected at baseline revealed distinct transcriptional repertoires associated with the development of CR in chest wall metastases treated with IMQ+RT. Among them, ICR genes such as CCL5, GZMA, GZMB, GZMH, PRF1, GNLY and TBX21 were overexpressed at baseline in tumors that achieved CR. Furthermore, enriched pathways were related to immunologic processes, with the top canonical pathways being related to NK cell and Th1/Th2 activation. Due to the limited number of responses in area B and absence of samples with CR, response prediction analyses were not performed for area B. Notably, the baseline favorable immune profile in lesions achieving CR after treatment with IMQ+RT, coincided with low expression of genes involved in DNA damage repair processes. This observation may imply the coexistence of dysregulated mechanisms in DNA repair within those lesions, potentially leading to the accumulation of more ds-DNA in micronuclei that activate innate immune signaling via cGAS/STING and increased mutational neoantigens, overall contributing to a spontaneous, although suboptimal, antitumor response. This interpretation is consistent with data linking the DNA repair gene expression level with tumor infiltration by T cells.54
We observed significant intrapatient tumor heterogeneity, but at the same time baseline analyses suggested that the transcriptional profile associated with CR following radiation therapy and IMQ is not sufficient to result in CR following IMQ alone. The inability to mount a Th-1, -sustained antitumor immune response was observed in samples of persistent or progressing lesions.
A high number of CRs were observed locally when RT was combined with topical IMQ; although only a small portion of patients with CR in area A demonstrated systemic tumor regression, suggesting that the immune response generated by one or two treatment cycles was not adequate for systemic tumor control. However, the significant and often durable local control of skin metastases with IMQ+RT is clinically important, as chest wall metastases remain a debilitating experience for the patient and a therapeutic dilemma for the treating physician. These tumors warrant treatment (even in the absence of other metastatic disease) as quality of life is often impaired, by PD with skin ulceration, bleeding and superinfection.55 56
Limitations of our trial included the small numbers of patients per cohort, heterogeneity of breast cancer subtypes treated, and different sites and burden of metastatic disease. The lesion to be irradiated was generally selected as distant from site B, to minimally expose site B to radiation. While partial inclusion of the tumor target has demonstrated to enable abscopal responses in selected patients treated by RT and anti-PD-1,57 58 no patients in cohort 1 received systemic immunotherapy. Despite systemic CTX no abscopal responses were observed in cohort 3. Another limitation of this study is the lack of systemic immunomonitoring, since the trial did not include PBMC collection during the course of the treatment. Recent studies have shown the emergence of potential biomarkers of response to focal RT and immune checkpoint blockade, like an increase of circulating IFN among patients with responding tumors17 or the detection of higher baseline levels of CD103+T cells.59
Despite these limitations, the results from this pilot trial support both safety and clinical efficacy of topical IMQ combined with local RT for recurrent breast cancer with frequent local and occasional systemic antitumor activity. The association of a baseline ICR tumor signature with complete local response to IMQ+RT validated the ICR hypothesis in metastatic breast cancer and warrants further prospective exploration in trials of radioimmunotherapy.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Gene expression data is available in the NCBI GEO repository under accession ID GSE282443: https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE282443.
Ethics statements
Patient consent for publication
Ethics approval
Approved by the NYU Institutional Review Board, all patients provided written consent for the study NYU 11-00598.
Acknowledgments
We thank all participating patients and their families, the Clinical Trials Office of the NYU Perlmutter Cancer Center, Valeant Pharmaceuticals North America LLC/Graceway Pharmaceuticals for providing IMQ at no cost. We wish to thank the late Dr Franco Muggia for his guidance in the design and conduct of this study. We also thank Dr Cristina Hajdu for help with the immunostains (MLH1, MSH2, MSH6 and PMS2).
References
Footnotes
SA and SD contributed equally.
Contributors Conception (SA, SCF), design (SA, SCF, SD, EW, FM, JG, DB), trial conduct/provision of patients/treatment (SA, YN, RO, MF-K, PGL, SCF), specimen acquisition/cytology analysis (SD, PGL), statistical analyses (XL, JG), specimen preparation/transcriptomic profiling and analyses (EW, DS, DB), manuscript writing (SA, SD, DB, JG, SCF), manuscript editing/approval (all). SCF is the guarantor.
Funding This work was supported by the National Cancer Institute (1R01CA161891, SA and SCF), the NCI Cancer Center Support Grant (5P30CA16087, JG and XL).
Competing interests DB and DR are currently employees of Kite Pharma, a Gilead company. FM is currently employee of Sonata Therapeutics. EW is currently employee of Craftsman Bio, South San Francisco, California, USA. SD: Research funding to Institution from Lytix Biopharma and Boehringer-Ingelheim, and compensation for consultant/advisory services from Lytix Biopharma, EMD Serono, Genentech, and Johnson & Johnson Enterprise Innovation Inc. SA: Research funding to Institution: Genentech, Merck, Celgene, BMS, Amgen, Gilead. Consultant: Cogent Biosciences. SCF: Research funding to Institution from Bristol Myers Squibb, Varian, Regeneron, Merck, Celldex, Arcus, NIH U54 CA 27429 ; and compensation for consultant/advisory services from Bristol Myers Squibb, Varian, ViewRay, Elekta, Regeneron, Eisai, AstraZeneca, MedImmune, Merck US, EMD Serono/Merck, Boehringer Ingelheim, Genentech/ROCHE, Nanobiotix, EMBioSys, Telix.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.