Article Text

Abstract
Objective The 2004 amendment to the Control of Substances Hazardous to Health 2002 regulations (COSHH 2004) introducing workplace exposure limits (WELs) was enacted in the UK in 2005. This study aimed to determine whether introducing this legislation coincided with a reduction in the incidence of work-related short latency respiratory disease (SLRD) attributed to the agents with a WEL. The second objective was to determine whether changes in legislation, WELs and market forces coincided with a reduction in the incidence of SLRD attributed to glutaraldehyde and latex.
Method Reports of SLRD made to the Surveillance of Work-related and Occupational Respiratory Disease scheme were used to estimate the change in incidence within reporters between two time periods (interrupted time series design) using a longitudinal, negative binomial regression model with β distributed random effects. A statistical interaction term was included in the model to make comparisons between the groups defined by suspected causal agent and/or occupation, essentially comparing two interrupted time series. Time periods were defined prospectively representing the changes in legislation or market forces.
Results The introduction of the COSHH 2004 legislation in the UK coincided with a significant reduction in reports of SLRD attributed to agents with a WEL relative to those without a WEL (ratio of incidence rate ratios: 0.70; 95% CI 0.52 to 0.93) and a significant reduction in SLRD attributed to glutaraldehyde in healthcare workers (0.20; 0.07 to 0.57) and latex in all workers (0.37; 0.16 to 0.85).
Conclusions These data are consistent with a beneficial effect of legislation aiming to reduce workplace exposures.
Statistics from Altmetric.com
What this paper adds
-
Over the last decade, there have been a number of events, such as legislation, market forces and interventions, aiming to reduce the incidence of workplace respiratory disease in the UK coinciding with a steady decline in reports of workplace respiratory disease to the Surveillance of Work-related and Occupational Respiratory Disease (SWORD) scheme.
-
We have compared changes in the incidence of work-related respiratory disease reported to SWORD attributed to specific agents and/or occupational groups within prospectively defined periods specified according to changes in legislation, market forces or interventions.
-
The introduction of Workplace Exposure Limits (WELs) through the 2004 amendment to the COSHH 2002 regulations coincided with a significant reduction in short latency respiratory disease and asthma attributed to agents with a WEL compared with those without a WEL.
-
Significant reductions in the incidence of short latency respiratory disease and asthma attributed to glutaraldehyde or latex relative to all other agents coincided with changes in legislation, mandatory advice from the Medical Devices Agency, setting new exposure limits and the removal of a glutaraldehyde-based disinfectant from the market.
-
Studies of interventions aiming to reduce work-related respiratory disease are relatively rare; therefore, the application of surveillance data to evaluate interventions is a useful tool.
Introduction
Work-related asthma (WRA) is of worldwide concern accounting for 16%–18% of adult-onset asthma.1 The UK is no exception where it is estimated that 1500–3000 people develop WRA every year.2 The lifetime cost stream of WRA to the UK is between £70 and 100 million per year, the majority of which is borne by the taxpayer and the affected worker, not the employer.3 Over the past decade, changes in legislation aiming to reduce the incidence of WRA have been implemented in the UK.
An important piece of UK legislation introduced in response to EC Directive (98/24/EC) was the 2004 amendment to the Control of Substances Hazardous to Health (COSHH) 2002 regulations (2004 COSHH amendment) effective from April 2005.4 This amendment aimed to reduce exposure to hazardous substances by focusing on adequate control measures, but was backed up by a workplace exposure limit (WEL) for all the listed agents.5 Prior to April 2005, hazardous substances had either an occupational exposure standard (OES) or a maximum exposure limit (MEL). For metal working fluids (MWFs), the MEL was withdrawn but not replaced with a WEL. The justification was that MWFs are variable in composition; therefore, the identification of a no-adverse effect level was not possible.6 This decision was probably influenced by a series of outbreaks of extrinsic allergic alveolitis and asthma attributed to MWF despite adherence to the existing guidelines occurring during the consultation process for the 2004 COSHH amendment.7 ,8
Glutaraldehyde is a long-recognised occupational asthmagen used as a disinfectant since the 1960s. In 1988, it was endorsed by the British Society of Gastroenterology as a first-line disinfectant for endoscopes.9 Although adverse effects on the user's health were recognised at the time, contemporary opinion was that no suitable alternative was available and efforts should be directed towards complying with the exposure limits stated in the 1988 COSHH regulations.9 This view was reiterated in 1993 although the health problem was now recognised as significant.10 The 1999 COSHH regulations introduced a MEL for glutaraldehyde resulting in increased costs prompting some health service organisations to seek alternative disinfectants.11 Eventually in 2002, one of the most commonly used glutaraldehyde-based disinfectants (Cidex), supplying approximately 70% of the UK market, was withdrawn and replaced by a non-glutaraldehyde-containing product.12 A further incentive to seek alternatives to glutaraldehyde was the emergence of variant Creutzfeldt–Jakob disease; glutaraldehyde-based disinfectants are ineffective against prions.13 Since 2002, most health service organisations have replaced glutaraldehyde-based disinfectants with alternatives, but no independent information regarding the extent to which glutaraldehyde-based disinfectants are currently used within the healthcare sector is available.14 In 2005, the existing MEL was replaced by a WEL.4 ,5
Another long-standing cause of WRA is the proteins found within the latex gloves; this exposure also particularly affects those working in the healthcare sector. We recently published data to show that two national level interventions (mandatory advice issued by the UK Medical Devices Agency in 1998 aiming to reduce exposure to latex in gloves and a court case in 2002) coincided with a decline in the incidence of allergic contact dermatitis attributed to latex and rubber glove allergens relative to other agents in healthcare workers.15 ,16 In 2000, the UK Health and Safety Executive published guidance aiming to increase awareness of the risks associated with latex glove use.17 Furthermore, the 2004 COSHH amendment required the use of latex gloves to be restricted ‘so far as is reasonably practicable’ and published an approved code of practice (ACOP) for latex gloves (effective 2005), but stopped short of introducing a WEL for latex.4
The Surveillance of Work-related and Occupational Respiratory Disease (SWORD) scheme collects reports of medically certified work-related respiratory disease seen by respiratory physicians in the UK. Data collection began in 1993 as part of the Occupational Disease Intelligence Network, and it has been part of The Health and Occupation Research Network since 2002.18 Approximately 70% of the eligible respiratory physicians were registered as SWORD reporters in 2005.19 Since 1999, the incidence of asthma reported to SWORD has been declining.20 ,21
The aim of this paper is to examine whether these changes in legislation and market forces coincide with the changes in the incidence of all work-related short latency respiratory disease (SLRD) or asthma only reported to SWORD as outlined below.
-
Following the introduction of the 2004 amendment to the COSHH 2002 regulations in April 2005 did the incidence in SLRD or asthma attributed to agents with a WEL decline relative to those without a WEL?5 ,10
-
Has the incidence of SLRD or asthma attributed to glutaraldehyde declined relative to all other causal agents consistent with the above changes in legislation and in response to market forces?
-
Has the incidence of SLRD or asthma attributed to latex declined relative to all other causal agents consistent with the above interventions and changes in legislation?
A key feature of the design is the use of a comparison group rather than the absolute change in incidence in the selected group, that is, the change is relative to the change in the comparison group in order to mitigate some of the bias arising from the nature of voluntary reporting.
Methods
The SWORD methodology has been described previously.18 ,19 Briefly, respiratory physicians return reports of work-related respiratory disease to SWORD specifying the suspected causal agent(s). Reports of SLRD (sum of reports of asthma, allergic alveolitis, rhinitis and inhalation accidents) or asthma alone spanning the period 1996–2010 were analysed. Some respiratory physicians were asked to report each month (core reporters) and others during a randomly allocated month each year (sample reporters). Since 2006, the time from symptom onset to consultation with the reporting respiratory physician was recorded.
For each event (changes in legislation or market forces) anticipated to impact on the incidence of SLRD or asthma, key dates were defined with the authors being ‘blind’ to the corresponding incidence data (table 1). These key dates were used to define time periods representing the time before, during and after the intervention, or simply before and after when a single cut point was appropriate as described below (table 2).
-
Amendment to the COSHH 2002 regulations (2004) and introduction of WELs4 ,5: the main analysis compared the change in incidence for agents with or without a WEL using a single-cut point of April 2005 (1a A, table 2). A second analysis, including an intermediate time period based on the median delay between symptom onset and consultation, was undertaken in order to make an allowance for the lag in reporting the case (1b A, table 2). The analysis was also repeated excluding one reporter who investigated the outbreak of asthma attributed to MWF described in the introduction because these cases were actively sought by the reporter investigating the outbreak rather than arising from the usual referral route.7 ,8 Causal agents reported for SLRD from 2003 to 2008 were coded according to whether or not a WEL was introduced in April 2005 using the EH40/2005 list,5 irrespective of any pre-existing previous exposure limit (OES or MEL). Reports of agents with insufficient information for categorisation were omitted from the analysis. The post-intervention period was terminated in December 2008 because later changes in legislation or events may have affected the incidence reported to SWORD.
-
Events potentially impacting on exposure to glutaraldehyde-based disinfectants: the key dates were the introduction of a MEL, the removal of Cidex from the market and the introduction of a WEL.4 ,11 ,12 These dates were used to define four periods (table 2). All reports attributed to glutaraldehyde from 1996 to 2008 were included. An occupational group designated as healthcare workers was selected according to Standard Occupation Classification 2000 codes as defined previously.16 This included medical practitioners, psychologists, pharmacists, pharmacologists ophthalmic opticians, dental practitioners, nurses, midwives, paramedics, medical radiographers, chiropodists, dispensing opticians, pharmaceutical dispensers, medical and dental technicians, therapists, nursing auxiliaries and assistants, ambulance staff, dental nurses and hospital porters. The analyses compared the changes in incidence of SLRD or asthma attributed to glutaraldehyde over time with cases attributed to all other agents, both in all workers (C, table 2) and within healthcare workers (D, table 2).
-
Interventions potentially impacting on exposure to latex gloves. The key dates—the publishing of mandatory advice by the UK Medical Devices Agency in June 1998, the publishing of guidance by the UK Health and Safety Executive in April 2000 and the 2004 COSHH amendment effective as of April 2005—were used to define four periods (table 2).15–17 All cases attributed to latex from 1996 to 2008 were included. The analysis compared the changes over time in incidence of SLRD or asthma attributed to latex with cases attributed to all other agents, in all workers (E, table 2) and within healthcare workers (F, table 2).
Summary of interventions and events expected to impact on work-related short latency respiratory disease investigated using SWORD data
Statistical interactions expressed as RIRRs representing an estimate of the ratio of the individual incidence rate ratios for the defined groups (A–F) for the stated periods as defined in the ‘Methods’ section
The statistical methods have been described previously.16 ,20 Monthly counts of cases per reporter (including zero reports) were analysed using a two-level negative binomial, that is, overdispersed regression model with β distributed random effects (Stata V.8). The two-level model assumed a hierarchical structure with time nested within reporter. Time was treated as a categorical variable, with categories defined above (table 2); dummy variables representing all categories except the earliest were included in the model. The model also controlled for seasonal variation, reporter type (core or sample), first month as a core reporter and first month as a new reporter as described previously.20 In order to make comparisons between the changes in incidence according to inclusion or exclusion within a group (defined by occupation and/or suspected causal agent), statistical interaction terms representing the product of the dummy time variables and group (0/1) were included in the model. Each interaction term measures the ratio of two incidence rate ratios (RIRRs) for the time periods specified: one for the target group and one for the non-target group.
 where a=target group and b=non-target group
where a=target group and b=non-target group
The 95% CIs were calculated for each RIRR and considered significant when the CI did not include one. Alternative models in which time was represented by yearly dummy variables (with 2005 as the reference) and with annual interaction terms (annual RIRR) corresponding to the product of the target group membership and each year were also fitted, allowing a more detailed description of the evolution over time of group differences.
Results
Between 2003 and 2008, 1190 cases of SLRD, including 855 (72%) asthma diagnoses, were reported to SWORD. The other major diagnostic categories included within SLRD besides asthma were inhalation accidents (55, 5%), rhinitis (149, 13%) and allergic alveolitis (79, 7%). Of these SLRD cases, 598 out of 1190 (50%) were attributed to an agent with a WEL and 79 (7%) reports did not include sufficient information to assign; for asthma diagnoses, 487 out of 855 (57%) were attributed to an agent with a WEL and 48 (6%) reports remained unassigned. The most frequently reported agents without a WEL were MWFs (143, 30%), animal fur/feather/excrement (93, 19%), food-related agents (33, 7%), cleaning products (19, 4%) and enzymes (18, 4%). Between 2006 and 2010, the delay between symptom onset and consultation was reported in 715 of 816 (88%) SLRD cases (median 19 months; range 0–338) and in 514 of 591 (87%) asthma cases (20 months; 0–338).
All comparisons between the groups were made by including an interaction terms in the model, which are expressed as the RIRRs (eqn (1)). For example, the RIRR in 1a A, table 2, compares the incidence rate ratio (IRR) from May 2005 to December 2008 (time 2)/January 2003 to April 2005 (time 1) for SLRD or asthma attributed to agents with a WEL (numerator in (eqn (1)) with the IRR for the same periods attributed to agents WITHOUT a WEL (denominator in (eqn (1)). Therefore, the RIRR for SLRD (1a A, table 2) of 0.70 (95% CI 0.52 to 0.93) can be interpreted as a significantly greater reduction in the incidence of reported SLRD attributed to agents with a WEL introduced in 2005 relative to those without the introduction of a WEL. The corresponding RIRR for asthma of 0.71 (0.50–1.02) is similar. When the analysis included an intermediate period corresponding to the median delay between symptom onset and consultation (1b A, table 2), there was a significantly greater reduction for SLRD and asthma attributed to agents with a WEL relative to those without a WEL during the intermediate period (1b A, table 2, time 2/time 1), but not during the post-intervention period (1b A, table 2, time 3/time 1). Exclusion of the reporter who investigated the outbreaks of respiratory disease attributed to MWF did not substantially alter the results (compare B with A, table 2). The annual changes relative to 2005 in the incidence of asthma attributed to agents with or without a WEL introduced during 2005 are shown in figure 1, but these annual IRRs were calculated only after the main analysis by periods was completed to ensure unbiased selection of the periods representing the interventions. A decline in the incidence for asthma attributed to agents with a WEL can be seen compared with those without a WEL, but there was also a (smaller) decline after 2007 in the incidence of cases attributed to agents without a WEL. The analysis shown in figure 1 was repeated excluding the reporter investigating the outbreaks of respiratory disease attributed to MWF (see online supplementary figure S2).

Annual trends in the incidence of asthma attributed to agents with or without a workplace exposure limit introduced during 2005 as reported to the Surveillance of Work-related and Occupational Respiratory Disease (SWORD) scheme. Incidence rate ratios are relative to 2005.
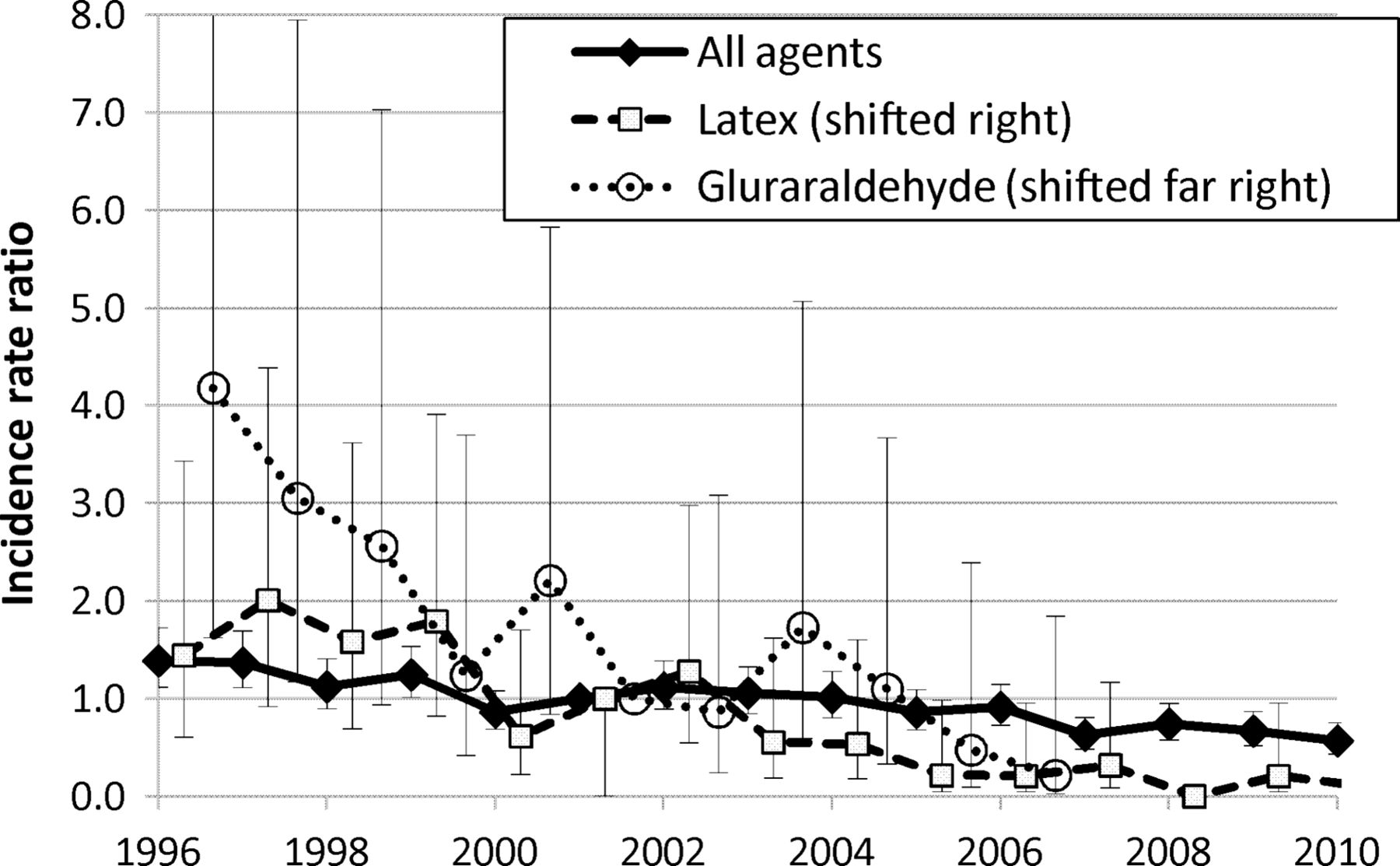
Between 1996 and 2008, there were 94 reports of SLRD with glutaraldehyde as the suspected causal agent. Most were employed in the healthcare sector (77; 82%) and only seven reports specified the source of the glutaraldehyde (six disinfectants and one developing fluids). Most workers were likely to have contacted glutaraldehyde via disinfectants (73 worked in endoscopy or operating theatre), but some workers were likely to be exposed to developing fluids (four in radiography and four in photographic processing). Over the entire period of the analysis (1996–2008), the estimated incidence of SLRD or asthma attributed to glutaraldehyde declined significantly relative to all other agents (SLRD annual RIRR: 0.95; 0.91–0.99 (figure 2) or asthma annual RIRR: 0.87; 0.81–0.94). The introduction of a MEL for glutaraldehyde in 1999 taken as a single cut point coincided with non-significant reduction in the incidence of SLRD and asthma attributed to glutaraldehyde relative to all other agents (2C, table 2, time 2/time 1); however, if an intermediate or lag period is included, then the reduction is significant (2 C, table 2, time 3/time 1). Restricting this analysis to those employed in the healthcare sector and using a single cut point, the reduction was significant (2 D, table 2, time 2/time 1). The removal of Cidex from the market and introduction of a WEL for glutaraldehyde both coincided with significant reductions in the incidence of SLRD and asthma when compared with the preintervention period (2 C, table 2, time 3/time 1 and time 4/time 1). As the effect of these interventions or events would have been cumulative, comparisons were also made between consecutive periods to pinpoint the effects of individual interventions (table 2). The removal of Cidex did not coincide with a significant reduction in SLRD or asthma attributed to glutaraldehyde when compared with the preceding period (2C, table 2 time 3/time 2), whereas the introduction of a WEL did coincide with a significant reduction for SLRD and a non-significant reduction for asthma (2 C, table 2 time 4/time 3).

{kind=link}
{kind=link}
Annual incidence rate ratios relative to 2001 for short latency respiratory disease reported to Surveillance of Work-related and Occupational Respiratory Disease (SWORD) attributed to all agents, glutaraldehyde and latex.
Between 1996 and 2008, there were 108 reports of SLRD, 99 of which were asthma, attributed to latex. The majority occurred in healthcare workers (SLRD 71 (66%); asthma 65(66%)). The only other occupation with multiple reports was laboratory workers including animal technicians (15 (14%)). Over the entire period of the analysis (1996–2008), the estimated incidence of SLRD or asthma attributed to latex declined significantly relative to all other agents (SLRD annual RIRR: 0.88; 0.83–0.94 (figure 2) or asthma annual RIRR: 0.89; 0.84–0.95). The mandatory advice issued by the Medical Devices agency did not coincide with a decline in SLRD or asthma attributed to latex relative to all other agents in all workers (3 E time 2/time 1) or within the healthcare sector (3 F, time 2/time 1). The publication of guidance by the Health and Safety Executive did not coincide with a change in SLRD or asthma attributed to latex relative to all other agents (3 E, time 3/time 2), but the 2004 COSHH amendment did coincide with a significant decline (3 E, time 4/time 3).
Discussion
The continuous decline in incidence of asthma reported to SWORD since 1999 is encouraging (figure 2).21 However, downward trends in reporting to SWORD should be interpreted cautiously; behavioural changes in reporters such as reduced reporting after a long membership time (reporter fatigue) will reinforce a downward trend.20 Using this study design that compares two interrupted time series analyses by means of an RIRR addresses bias in reporting behaviour that occurs equally across all reports (ie, equally distributed across causal agents or types of ill health) such as reporter fatigue. This is a major advantage of this method over a simple time series design, since reporter fatigue is known to be a significant source of bias within this voluntary reporting scheme.20 However, this design does not address bias arising from differential reporting behaviour (ie, varies according to the type of ill health or causal agent). An intervention or change in legislation might result in increased reporting of a causal agent or ill health due to increased awareness of the problem in patients and physicians. Depending on whether this occurs in the case or control groups, the RIRR will increase or decrease, respectively. Another potential source of bias occurs if a physician changes her/his opinion on the work-relatedness of a causal agent/ill-health combination over time, or if a reorganisation of service provision alters the distribution of types of work-related disease seen by a reporter. However, within-reporter comparison aspect of the model mitigates the effect of individual reporters changing their reporting habits.
The 2004 amendment to the COSHH 2002 regulations coincided with a decline in incidence of SLRD and asthma attributed to agents with a WEL relative to those without a WEL suggesting that the new legislation had a beneficial effect (1a A, table 2). Furthermore, differential reporting bias, such as increased reporting of agents with a WEL due to increased awareness or reduced reporting of agents without a WEL due to perceived decreasing importance, would have an effect in the opposite direction, that is, towards an increase in incidence for causal agents with a WEL relative to those without a WEL. A delay between the changes in legislation and the observed effect was postulated corresponding to the lag between symptom onset and consultation with a respiratory physician. However, when the analysis included an intermediate period (1b A, table 2), the decline was not lagged by the median delay between symptom onset and reporting to SWORD. New workplace legislation is generally preceded by a period of consultation, indeed the UK Health and Safety Commission consultation on the proposed changes to occupational exposure limits occurred during 2003,6 followed by advance notice and promotion of awareness of the impending change. Therefore, it is possible that some workplaces made changes to comply with the new legislation before the final deadline, thereby diminishing the expected lag in observing the effect on SWORD reporting. This hypothesis of anticipation of new legislation bringing about early changes is supported by the observation that the decline in asthma attributed to agents with a WEL begins during 2004 (figure 1), but other explanations such as an increase in the delay between symptom onset and reporting since 2006 cannot be ruled out. The concomitant increase in the incidence of asthma attributed to agents without a WEL suggests that conversely the control of agents no longer the focus of attention becomes neglected (figure 1). However, this increase is partly explained by the outbreaks of SLRD attributed to MWF discussed earlier investigated by one reporter (see online supplementary figure S2). Generally, it would be inappropriate to exclude any reporters from a trends analysis, but it is offered here because the timing of the outbreaks is probably unrelated to, but favours, the argument for a positive effect of the introduction of WELs. Furthermore, the cases from the outbreaks of asthma and allergic alveolitis attributed to MWF returned by just one reporter might result from workplace visits rather than arising through normal clinical practice.8 Reassuringly, the exclusion of this reporter resulted in only a small change to the results (1a and 1b compare A and B table 2), suggesting that the observed decline in the incidence of SLRD or asthma attributed to agents with a WEL relative to those without a WEL was not simply due to this single unusual event.
The consistent significant decline in SLRD attributed to glutaraldehyde relative to all other agents from 1996 onwards provides evidence of the effect of consecutive changes in legislation and market forces. The significant reduction in SLRD attributed to glutaraldehyde in healthcare workers consistent with an effect of the introduction of a MEL (2 D, table 2, time 2/time 1) may reflect a higher level of concern within the healthcare sector and/or anticipation of the change in legislation leading to an earlier response in the healthcare sector. Using the date of withdrawal of Cidex from the market as a single cut point for the comparison between glutaraldehyde and all other agents did not show a significant reduction for glutaraldehyde (2 C, table 2, time 3/time 2), whereas using the single cut point for the introduction of a WEL showed a significant reduction (2 C, table 2, time 4/time 3). However, this could also represent a lag in the effect of the removal of Cidex from the market. Pinpointing the effect of individual interventions may not be feasible for the groups with small numbers of cases and several consecutive events, but the combination of the withdrawal of Cidex and the introduction of a WEL showed a greater decline (2 C, table 2, time 4/time 2) than either of the individual events. Occasional reports of asthma attributed to substitutes for glutaraldehyde highlight the need to ensure that replacement products are indeed safer.
The significant decline in SLRD attributed to latex relative to other agents from 1996 onwards supports similar conclusions to SLRD attributed to glutaraldehyde, that is, suggests a beneficial effect of consecutive interventions and changes in legislation. Interestingly, the healthcare sector seemed to respond more positively to the introduction of a MEL in respect of glutaraldehyde than to the mandatory advice issued by the Medical Devices Agency in respect of latex; yet, both are legally binding. The 2004 COSHH amendment coincided with a significant decline in the incidence of SLRD attributed to latex relative to all other agents suggesting that this had been effective (3 E, time4/time3). However, the publication of guidance by the HSE in 2000 accompanied by an ongoing campaign might also have contributed to this decline, although the HSE guidance alone did not coincide with a significant reduction (3 F, time 3/time 2).
Overall, these data are consistent with a beneficial effect of the introduction of a WEL through the 2004 COSHH amendment and the introduction of a MEL for glutaraldehyde. The beneficial effect of the 2004 COSHH amendment on SLRD attributed to latex would have been through publishing the ACOP and drawing attention to the HSE list of asthmagens,4 ,22 since the 2004 amendment did not specify a WEL for latex. Removal of Cidex from the market in combination with the introduction of new WELs also had a beneficial effect, but it was not possible to identify which of these events had the most impact from these temporal associations. In general, identifying a significant decline in incidence relative to the declining overall trend requires either a large effect of the intervention or a large number of cases. An effect cannot be ruled out in the smaller groups where significant differences were not observed. Conversely, a decline in reports can only ever be consistent with a beneficial effect, rather than direct evidence, since other events occurring in the same time may also make a significant contribution.
Studies of interventions aiming to reduce work-related SLRD or asthma are relatively rare and few have a prospective design.23 The use of health surveillance data allows a prospective study design to be used retrospectively and allows the analysis of unplanned events. However, voluntary reporting introduces bias; the use of a comparison group goes someway towards alleviating this problem but we cannot exclude the possibility of events unrelated to the intervention affecting the control group differently to the intervention group thereby reinforcing or diminishing the difference.
Acknowledgments
Thanks are due to all physicians reporting to SWORD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Footnotes
-
Contributors SJS designed the study, undertook the analysis and wrote the manuscript. RM developed the statistical methods and commented on the manuscript. ST commented on the manuscript. MC managed the data collection. RMA commented on the manuscript.
-
Funding The SWORD project is partly funded by the UK Health and Safety Executive. Any opinions and conclusions expressed herein are solely those of the authors and not of the funding body.
-
Competing interests None.
-
Ethics approval NRES Committee North West—11/NW/0832.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data request may be made in by writing to the Health and Occupation Reporting Network to melanie.carder@manchester.ac.uk.