Article Text

Abstract
Objectives We aimed to estimate the fraction of deaths from ovarian cancer attributable to asbestos exposure in Lombardy Region, Italy, using a novel approach that exploits the fact that ovarian cancer asbestos exposure is associated with pleural cancer and other risk factors for breast cancer.
Methods This ecological study is based on the Italian National Institute of Statistics mortality data. We formulate a trivariate Bayesian joint disease model to estimate the attributable fraction (AF) and the number of ovarian cancer deaths attributable to asbestos exposure from the geographic distribution of ovarian, pleural and breast cancer mortality at the municipality level from 2000 to 2018. Expected deaths and standardised mortality ratios were calculated using regional rates.
Results We found shared dependencies between ovarian and pleural cancer, which capture risk factors common to the two diseases (asbestos exposure), and a spatially structured clustering component shared between ovarian and breast cancer, capturing other risk factors. Based on 10 462 ovarian cancer deaths, we estimated that 574 (95% credibility interval 388–819) were attributable to asbestos (AF 5.5%; 95% credibility interval 3.7–7.8). AF reaches 34%–47% in some municipalities with known heavy asbestos pollution.
Conclusions The impact of asbestos on ovarian cancer occurrence can be relevant, particularly in areas with high asbestos exposure. Estimating attributable cases was possible only by using advanced Bayesian modelling to consider other risk factors for ovarian cancer. These findings are instrumental in tailoring public health surveillance programmes and implementing compensation and prevention policies.
- Asbestos
- Epidemiology
- Public Health Surveillance
- Statistics
- Environment
Data availability statement
No data are available. Data were provided by the Italian National Institute of Statistics (ISTAT) and cannot be made available by the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Ovarian cancer is among the diseases with a well-established causal association with asbestos exposure.
However, few studies have quantified the fraction of ovarian cancers attributable to asbestos at the population level.
WHAT THIS STUDY ADDS
We present an innovative approach to estimating population-attributable fractions using a Bayesian joint disease model on ecological mortality data.
We exploited the fact that ovarian cancer shares common aetiologies (and hence spatial distributions) with both pleural cancer (asbestos) and breast cancer (reproductive and lifestyle factors).
In a large (10 million people) and highly industrialised area, we estimated an overall population attributable fraction of 5.5%; this proportion was >30% in highly exposed communities.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Targeted public health actions and disease surveillance programmes can be tailored based on these findings.
Introduction
Asbestos is one of the most widespread occupational carcinogens worldwide. Exposure to asbestos causes malignant mesothelioma (MM), cancer of the lung, larynx and ovary.1 The global burden of asbestos-related diseases (ARDs) has been estimated at around 231 000 cases/year.2
Ovarian cancer is the seventh most common cancer in women globally.3 In 2020, 207 252 deaths due to ovarian cancer globally and 319 959 new cases were registered worldwide.4 Exposure resulted in asbestos fibres, which are not degrading and are accumulating in ovarian epithelial cells, and together with results from cohort studies on the association between ovarian cancer and asbestos exposure, establish a potential causal link.1 5 A report estimated that 54% of ovarian cancers among women occupationally exposed to asbestos were attributable to asbestos exposure.6
In Italy, the health impact of asbestos exposure was estimated at 4400 deaths from ARDs each year from 2010 to 2016. Among the ARDs, 16 deaths of ovarian cancers per year were attributed to occupational exposure to asbestos in asbestos-cement plants and glassworks.7 The estimates were based on the meta-analysis of 21 Italian cohorts of former asbestos-cement workers.8 More recently, a mortality update of 52 Italian occupational cohorts, including the main asbestos-exposed sectors, has been published.9 For women, an excess of mortality from ovary cancers was reported (58 observed vs 40.8 expected, SMR=1.42).9 In Italy, an epidemiological surveillance system of mesothelioma incident cases has been developed through a national registry, but the systematic recognition of other asbestos-related neoplasms is still lacking.10
In a recent paper, several Bayesian hierarchical shared models were applied to the bivariate spatial distribution of ovarian and pleural cancer mortality by the municipality in the Lombardy region (northwest Italy) in 2000–2018 to study the spatial co-occurrence of the two diseases. We found evidence of a shared risk factor between ovarian and pleural cancer mortality at a small geographical level. This latent shared factor was interpreted as a proxy of asbestos exposure.11
We extended this model, specifying a trivariate Bayesian spatial shared model and estimating the contribution of asbestos exposure to the occurrence of ovarian cancer at a small geographical scale. To stabilise the estimates, we included a third disease, breast cancer, which is not related to asbestos but may share other risk factors with ovarian cancer.12 This study aimed to estimate attributable fractions (AFs) of ovarian cancer deaths associated with asbestos exposure and to identify hot spots of ovarian cancer attributable to asbestos exposure. The quantification of asbestos-related ovarian cancer cases is substantial information for improving asbestos preventive policies and the effectiveness of occupational disease insurance systems.
Materials and methods
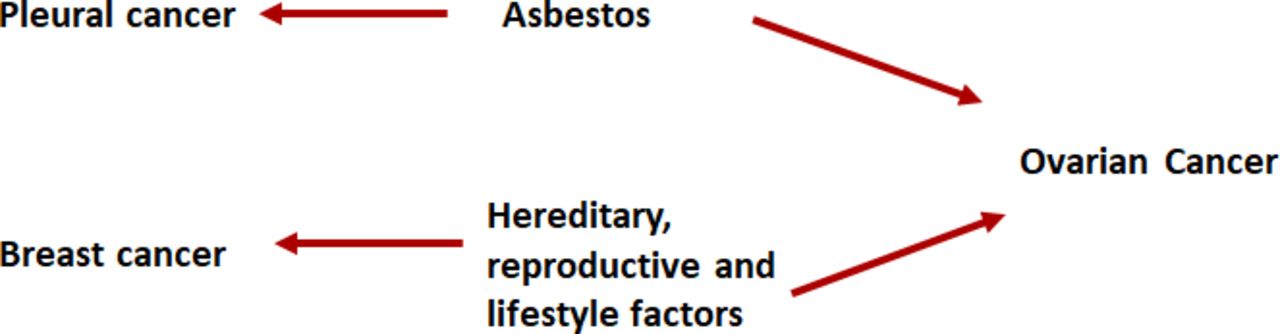
We adopted a Bayesian framework and based our modelling on prior epidemiological literature. Our assumption is that the correlations among different diseases depend on latent shared risk factors.13 From a modelling perspective, such correlation is captured by latently shared spatially structured random terms. Here, in particular, based on the current epidemiological literature, we assumed that pleural and ovarian cancers share asbestos exposure; breast and ovarian cancers share other risk factors linked to lifestyles and reproductive life. A simplified directed acyclic graph of the assumed relationships is reported in figure 1.

A simplified directed acyclic graph of the relationships among pleural, ovarian and breast cancer (see text).
Female death records of pleural, ovarian and breast cancer occurring in the Lombardy region in the period 2000–2018 were extracted by the Statistical Service of the Italian National Institute of Health from the cause-specific mortality database of the Italian National Institute of Statistics (ISTAT). We analysed the death records of the following codes of the ninth and 10th International Classification of Diseases (ICD): ovarian cancer (ICD-9: 183.0 and ICD-10: C56), pleural cancer (including pleural cancer, ICD-9: 163 and ICD-10: C38.4, and pleural mesothelioma, ICD-10: C45.0) and breast cancer (ICD-9: 174 and ICD-10: C50). Population denominators came from the same sources of mortality data (ISTAT).
Following internal indirect age standardisation, year-specific and age-specific reference rates based on the whole Lombardy region in the years 2000–2018 by 18 age classes (0–4, …, 85+) were used to compute the expected number of cases for each of the 1546 municipalities.14 Then, for each ith municipality (i=1,…,1546), we calculated the standardised mortality ratio (SMR=observed/expected number of deaths, summing over all age classes) as an estimate of the relative risk (RR), that is, the disease risk of each area compared with the adopted standard—the overall mortality in the Lombardy region. Implicitly, internal indirect standardisation specifies the same testing procedure for each area.
SMRs show strong random variability, which we filtered out by applying Bayesian smoothing. The spatial pattern of mortality for ovarian, pleural and breast cancer in females at the municipality level is described using hierarchical Bayesian models with spatially structured and unstructured random effects (Besag, York and Mollié (BYM) model).15 Technical and methodological details are described in Stoppa et al.11
Trivariate Bayesian disease models and latent shared component analysis
The trivariate Bayesian disease model is derived from the model selection strategy previously described in Stoppa et al.11
Let OiP, OiO and OiB denote the observed number of deaths in the ith municipality for, respectively, pleural, ovarian and breast cancer. As in the BYM model, the conditional likelihoods for each disease are Poisson (E iP θ iP), Poisson (E iO θ iO) and Poisson (E iB θ iB), where E is the expected number of cases and θ is the RR. We specified the following random effects log-linear model on the RRs θ iP, θ iO and θ iB :
 (1)
(1)
 (2)
(2)
 (3)
(3)
The terms v iP, v iO, v iB and u iB represent the unshared components, the disease-specific heterogeneity and breast cancer-specific clustering, respectively (ie, the set of unique disease-specific random terms).
The latent shared random terms model the correlations among the three diseases. Regarding the shared components between pleural and ovarian cancer, the terms ζ i and φ i denote shared heterogeneity and clustering components aimed to capture risk factors common to the two diseases—interpretable as asbestos exposure, both localised, that is, heterogeneity components, or at large scale, that is, clustering components. The model also includes shared clustering components, the term ψ i, between ovarian and breast cancer, aimed at capturing risk factors (not related to asbestos) linked to large-scale risk components shared by the two diseases.
The parameters δ, ω and γ are tuning parameters that allow for a different impact of the shared components on each disease. In particular, for example, the effect of the latent shared risk factor, that is, asbestos exposure, in our case, is allowed to be different for the two diseases (pleural and ovarian cancer). Indeed, we expect a larger effect of asbestos exposure on pleural than ovarian cancer; then, the tuning parameter δ in our model should be larger than one. We can also express this concept in a different way: algebraically, δ=βP/βO, where β P and β Oare the regression coefficients of the latent shared factor on each of the two diseases (P for pleural and O for ovarian cancer). Then, if the RR of asbestos exposure to pleural cancer is greater than the RR of asbestos exposure to ovarian cancer, the regression coefficients will be β P>β O and the tuning parameter δ>1. By analogy, the same arguments stand for ω and γ.16 The tuning parameters are assumed to be a priori lognormal distributed with zero mean and low precision; in detail, we assumed a normal prior for the log-parameter N(0, σ2) with variance σ2=0.17—a choice that corresponds to a 95% probability interval of the ratio of the two regression coefficients of 0.45 and 2.25. The priors and hyperpriors for the other model terms are the same as specified in Stoppa et al.11
Practical relevance and attributable deaths
AF and attributable cases are helpful in public health and risk communication. They inform about the proportion of diseases associated with specified risk factors.
We modelled the attributable risk of ovarian cancer resulting from asbestos exposure using the formula currently used to report attributable cases in ecological studies.17 Given  be the risk of ovarian cancer (see for comparison formula (2)) having omitted the shared clustering component with pleural cancer,
be the risk of ovarian cancer (see for comparison formula (2)) having omitted the shared clustering component with pleural cancer,  then:
then:
 (4)
(4)
 (5)
(5)
We estimated the attributable risk in the sensitivity analysis, omitting the heterogeneity and clustering components (online supplemental figure 3,4 and table 3). Following our Bayesian framework, the clustering component is expected to be the most important; therefore, we used formula (5) to report our results. We reported in the online supplemental methods to profile areas with a high attributable fraction (see online supplemental figure 2).
Supplemental material
For all the models described, the marginal posterior distributions of the parameters of interest were approximated by Monte Carlo Markov Chain (MCMC) methods. We used WinBUGS software18 for MCMC analyses. For each model, we ran two independent chains; checks for the achieved convergence of the algorithm were performed following Gelman and Rubin.19
Results
The number of deaths from pleural cancer among women in the period 2000–2018 in the Lombardy region (Italy) (study area online supplemental figure 1) was 2070, with the following distribution of ICD codes: ICD-9 (2000–2002): 163 (malignant neoplasm of the pleura), 262 deaths; ICD-10 (2003–2018): C38.4 (malignant neoplasm of the pleura), 271 deaths and ICD-10: C45.0 (mesothelioma of the pleura), 1537 deaths. Across municipalities, SMRs ranged from 0 to 22.14. The expected number of deaths was highly variable, ranging from less than 0.01 to 333.20, reflecting the large variability in municipalities’ population sizes. The municipality of Broni, in the province of Pavia, showed the second highest SMR, equal to 18.3 (observed 51 cases and expected: 2.79); the municipality of Moio de’ Calvi was first ranked (<3 observed cases and 0.05 expected).
We retrieved 10 462 deaths for ovarian cancer, with SMRs ranging from 0 to 19.15; the municipality of Calcio was among the highest (14 observed and 4.87 expected), while Pedesina had the highest (<3 cases and 0.05 expected).
Regarding breast cancer, we collected 37 621 deaths, with SMRs ranging from 0 to 6.12; among the highest was Gravedona, with 17 observed cases and 6.24 expected; the first rank was Morterone (<3 cases and 0.16 expected).
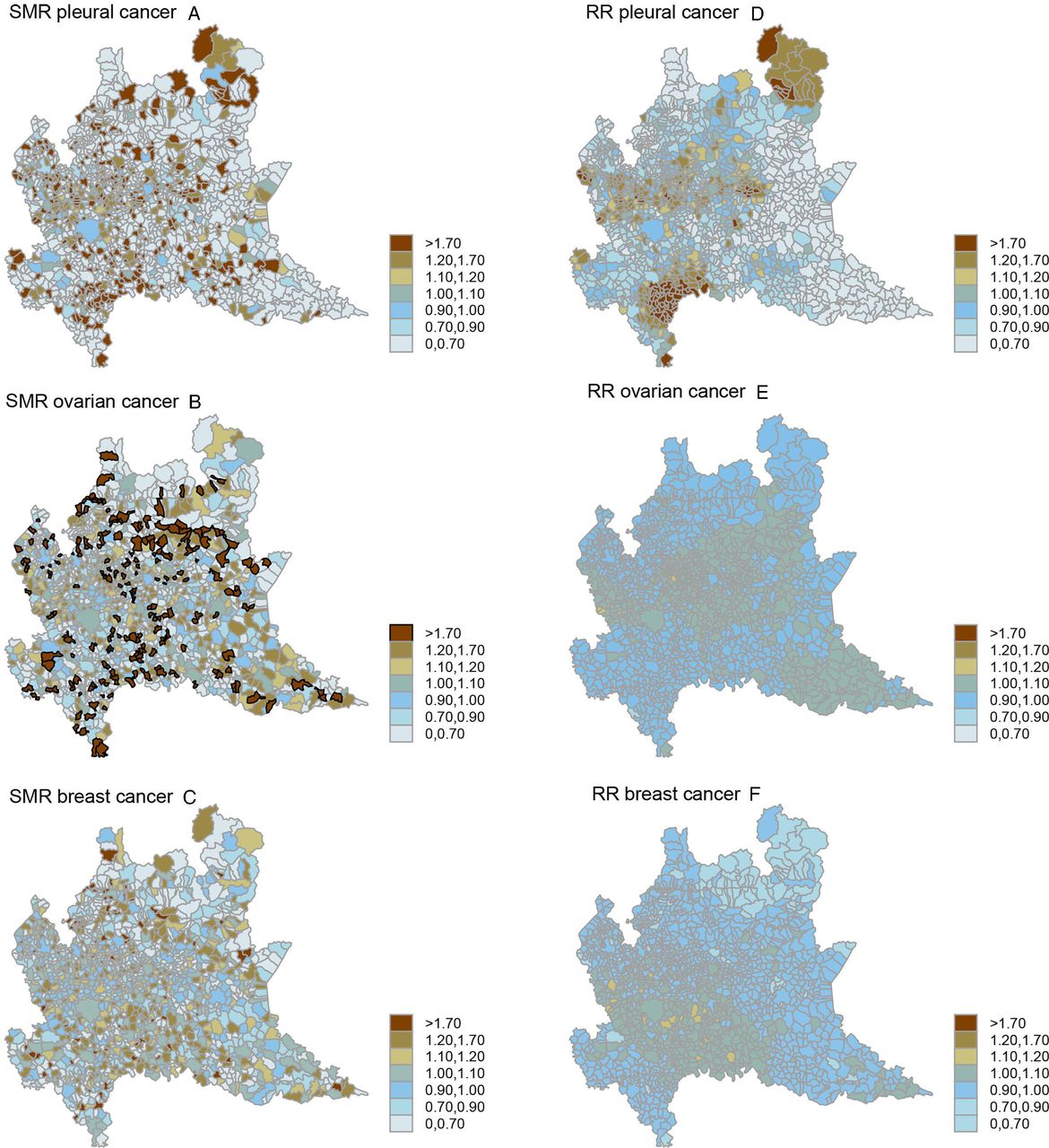
In figure 2, we report the spatial distribution of SMRs (upper panels) and Bayesian smoothed RRs (lower panels) from the BYM model for pleural cancer (left panels), ovarian cancer (centre panels) and breast cancer (right panels). Maps of Bayesian smoothed RRs appeared cleaner compared with SMRs. The geographical pattern was more evident once the RR had been smoothed, and the spatial pattern for pleural cancer was very strong. Well-known asbestos-polluted areas were clearly identified. Specifically, the areas that have been identified are: the Broni area in the Province of Pavia (the southwest part of the region); several areas in the prealpine part of the region corresponding to the highly industrialised provinces of Varese, Monza and Brianza, Bergamo and Brescia and a wide area located in the mountainous northern territories of the Lombardy region, a non-industrialised, mountain area of the Province of Sondrio with low population density.20 21

Spatial choropleth map of raw ((A) SMR pleural cancer, (B) SMR ovarian cancer and (C) SMR breast cancer) and Bayesian smoothed ((D) RR pleural cancer, (E) RR ovarian cancer; and (F) RR breast cancer) SMRs of pleural cancer, ovarian cancer and breast cancer. Lombardy region, 2000–2018. Absolute scale (partially modified from Stoppa et al 11). SMR, standardised mortality ratio.
The spatial pattern for ovarian and breast cancer was less pronounced. The heterogeneity and clustering odds summarise the relative importance of the two sources of variability: the pleural cancer spatial pattern was, as expected, predominant; breast cancer showed a more complex pattern with both random components almost equally represented; ovarian cancer is similar to breast cancer but with a more important clustering component (online supplemental table 1).
Overall, it is difficult to understand the presence and extent of a correlation among the three diseases from these marginal descriptive maps.
Trivariate Bayesian joint disease model
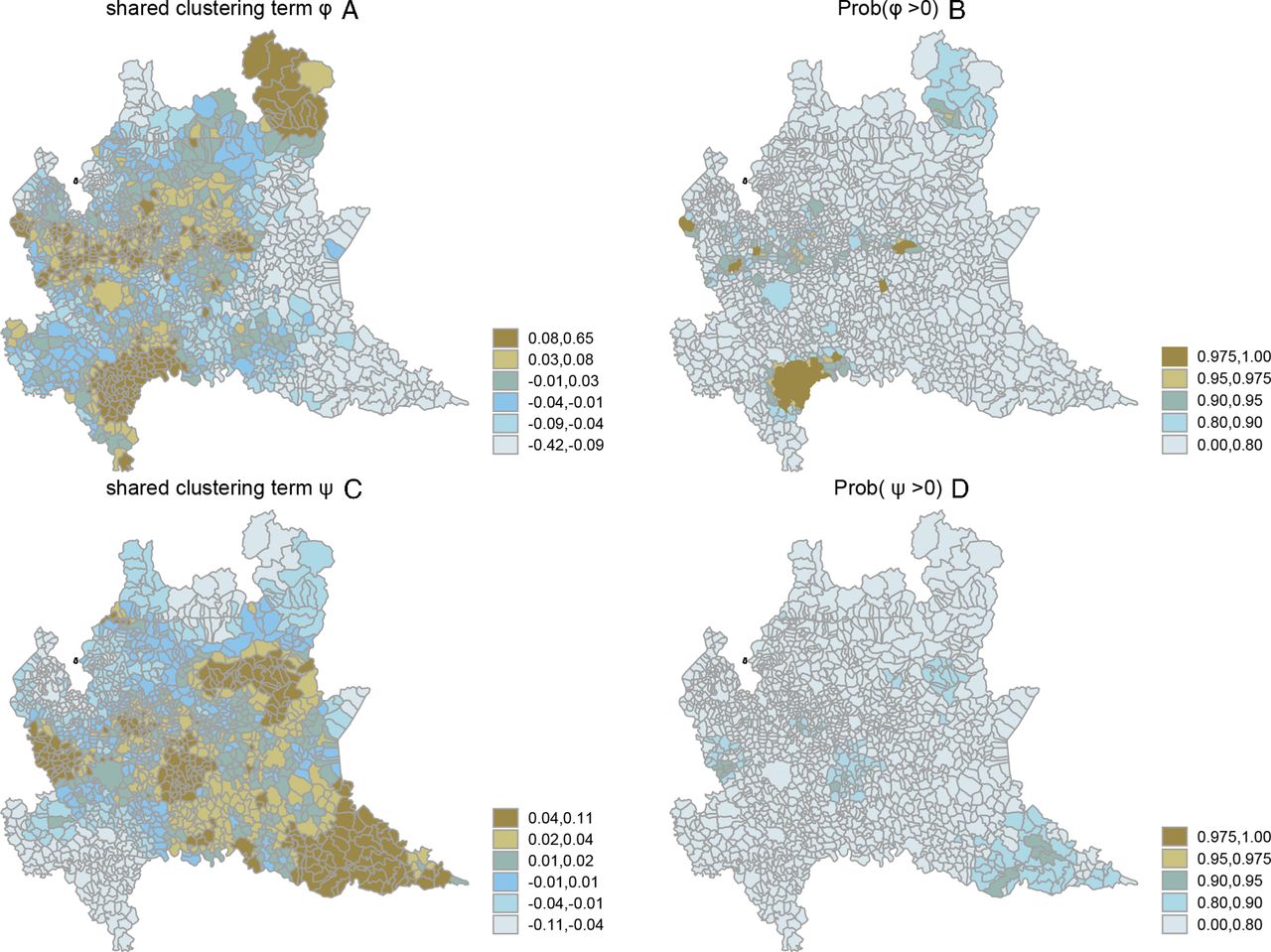
The map of the shared clustering component (panel A) and the map of the posterior probability of the direction of effect of the shared clustering component (panel B) between pleural cancer and ovarian cancer are reported in figure 3. Areas with a common risk factor for the two diseases appear clearly. These areas are the well-known areas where asbestos exposure was documented, and, in particular, in the province of Pavia, the area of Broni, where a cement-asbestos plant was located, and in the province of Bergamo, the area of Calcio, where asbestos textile industries were present. In the prealpine part of the region, occupational risks were documented in the highly industrialised provinces of Varese, Monza and Brianza, Bergamo and Brescia.20 21 The map of the shared spatially structured clustering component between ovarian and breast cancer (ψ)—figure 3 panel (C) and (D)—shows a quite different geographic pattern, highlighting the large urbanised areas around the provincial capital cities of Milan, Monza, Lodi, Cremona, Bergamo, Brescia and Mantova.

Map of the shared spatially structured clustering component between ovarian and pleural cancer (φ) (A) (relative scale). Map of the posterior probability of direction of effect (Prob(φ>0)) of the shared clustering component between ovarian and pleural cancer (B). Panel (C) shows the map of the shared spatially structured clustering components between ovarian and breast cancer (ψ) (relative scale). Map of the posterior probability of direction of effect (Prob(ψ>0)) of the shared clustering component between ovarian and breast cancer (D). Lombardy region, 2000–2018.
The posterior probabilities of the direction of effect reported on an absolute scale in panels (B) and (D) of figure 3 show that the shared components are important for a few selected areas.
Practical relevance
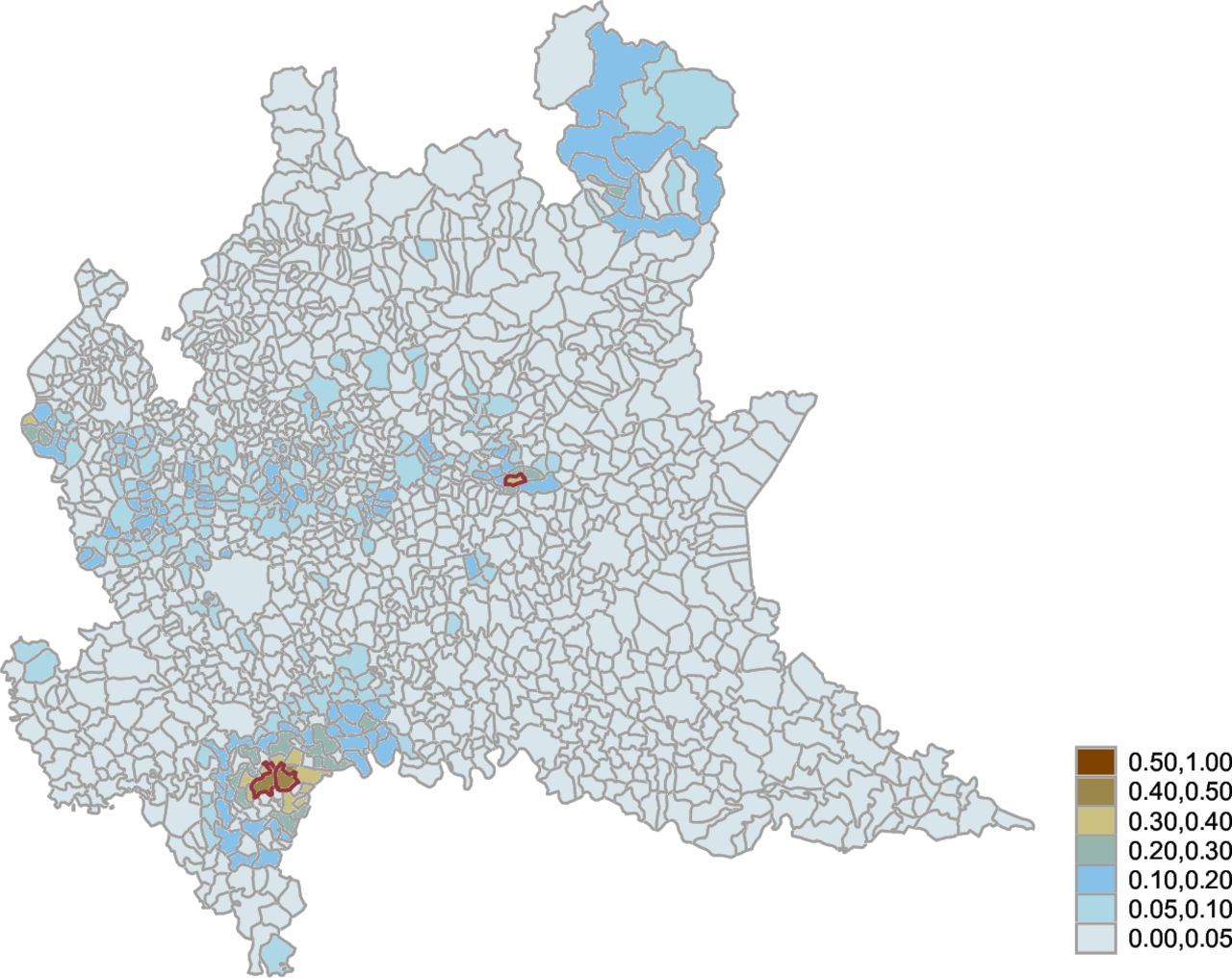
In figure 4, we report the estimated attributable fraction of ovarian cancer by municipality. Two areas are identified: the well-known Broni area22 23 and the area around Iseo Lake (in the Brescia province), where the municipality of Sarnico is located and where a factory operated from 1920 to 1993 producing asbestos textile items (laces, ropes, etc) and rubber and metal gaskets.20 21 24

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Attributable risk proportion of ovarian cancer by the municipality. Lombardy region, 2000–2018. Broni, Stradella and Sarnico are highlighted in red.
Out of 10 462 ovarian cancer deaths, we estimated that 574 (95% credibility interval 388–819) were attributable to shared asbestos exposure (attributable risk 5.5%–95% credibility interval 3.7–7.8). The highest AFs were estimated for Broni and Stradella (a municipality adjacent to Broni) (47%, 6 attributable deaths out of 13 cases in each municipality), followed by Sarnico with an attributable fraction of 34% (3.6 attributable deaths out of 10 observed cases)—see online supplemental table 2, which reports the municipalities with an attributable fraction larger than 30% and three or more deaths for ovarian and pleural cancer.
Discussion
Mortality from pleural cancer, MM and asbestosis is frequently used to quantify the impact of asbestos exposure nationally and internationally25 26 due to the high aetiological fraction associated with asbestos exposure for these diseases. Accordingly, the geographical distribution of MM can be used as a proxy for past asbestos exposure.5 27 28 In the present study, we found evidence of an association between ovarian and pleural cancer mortality at a small geographical level. Consistently, the shared geographical pattern between ovarian and pleural cancers highlights areas with known environmental and occupational sources of asbestos exposure.
Moreover, we found that the impact of asbestos exposure on ovarian cancer cases at the population level can be substantial in selected populations.
Overall, we counted 10 462 ovarian cancers in the Lombardy region in 2000–2018, of which 574 (95% credibility interval 388–819) were attributable to asbestos (attributable risk 5.5%–95% credibility interval 3.7–7.8), about 30 cases per year in a region of about 10 million inhabitants.
A study on ARD mortality in Italy7 estimated at the national level around 16 deaths from ovarian cancer per year attributable to occupational asbestos exposure in the asbestos-cement and glasswork sectors. However, the overall contribution of asbestos to ovarian cancer occurrence was underestimated due to the lack of inclusion of occupational sectors with a high proportion of female workforce (eg, the textile industry). Our results suggest a more widespread asbestos exposure, either occupational or non-occupational.29 30
Several studies estimated that occupational asbestos exposure might cause 1%–3% of ovarian malignancies in Argentina, Brazil, Colombia, Mexico, Korea and France.31–33 High mortality from ovarian cancer was reported in 29 Brazilian municipalities with high use of asbestos compared with the rest of the country.28
In selected populations, occupational asbestos exposure may result in a very high attributable fraction. A recent study, for example, reported an asbestos-attributable fraction of 54% of ovarian malignancies in women occupationally exposed.6 Our study estimated the highest AF in resident populations living in Broni, Stradella and Sarnico municipalities. These high AFs partially depend on the fact that ovarian cancer mortality in these municipalities is the result of a high prevalence of asbestos exposure and a background low incidence of ovarian cancer.
Stradella is a neighbouring municipality of Broni, where the second Italian largest asbestos-cement plant operated from 1932 to 1993, and clean-up actions are ongoing.34 In a recent study in these two towns, exceedingly high MM incidence rates in both genders were observed; in women, standardised incidence ratio (SIR) was 11.1, based on 121 cases. After excluding occupational and familial exposure, SIR were 16.7 in Broni and 13 in Stradella.22 It is remarkable that in Broni and Stradella, previous epidemiological analytical studies have documented environmental contamination and occupational asbestos exposure. A more recent national analysis confirmed the increasing MM mortality clusters among the female population in these areas.27
In Sarnico, one asbestos textile factory and two non-asbestos textile facilities were closely located. In all of them, women constituted the main workforce; the risk of MM incidence and mortality among them was documented.21 35 36 Notably, a high number of MM incident cases in the non-asbestos textile industry in Italy is reported in the seventh Report of the National Registry of Mesothelioma37 and Lombardy is the work sector that causes the greatest number of MM.
The strong environmental and occupational women’s exposure to asbestos in the Broni and Stradella municipalities with a relatively low background risk of ovarian cancer resulted in an attributable fraction of 40%–47%. Also, in Sarnico, despite the background risk of ovarian cancer being higher than average, the attributable fraction resulted in a high of around 34%. For all these municipalities, the AF was close to those estimated for strictly occupationally exposed women.3 38–40
The use of breast cancer in the models as a third disease, aimed at improving the goodness of fit and modelling better the effect of other risk factors that might explain the geographic distribution of ovarian cancer, deserves specific remarks. As specified at the beginning of the paper, breast and ovary cancers share several risk factors, except asbestos, for which the association with ovarian cancer is classified with sufficient evidence by the International Agency for Research on Cancer.1
Apart from well-documented hereditary (BReast CAncer gene (BRCA) mutations) or familiarity, reproductive factors (age at first full-term pregnancy or nulliparity) and lifestyle (overweight or obesity) shared with breast cancer, a specific comment should be made, in particular, regarding oestrogen therapy, postmenopausal and tobacco smoking, which are carcinogenic agents with sufficient evidence for ovary cancer and limited evidence for breast cancers; X-radiations and Gamma-radiations are carcinogens for both diseases (with sufficient evidence for breast and limited evidence for ovary cancers). In addition, ovary cancer is associated with all forms of asbestos (sufficient evidence) and talc-based body powder (perineal use: limited evidence).41
This study is subject to at least the following limitations. First, because of migration, the municipality mortality rates by residence at death may not reflect past asbestos exposure, particularly given the long latency between exposure and disease.
Second, there is some dispute about the potential misclassification between peritoneal mesotheliomas and ovarian cancer.40 Therefore, we restricted our study to pleural cases instead of mesothelioma cases to minimise misclassification.
Third, Lombardy is not covered by a cancer registry; therefore, we had to base our analyses on mortality data. While mortality is a good proxy for MM incidence due to very poor survival, it may be a suboptimal surrogate for ovarian cancer (5 years of net survival of around 40%) and even more so for breast cancer (5 years of net survival of around 88%).42 However, the whole Italian population is covered by a public health system. Moreover, Lombardy is a region with many healthcare facilities of high quality and breast cancer screening is offered for free. For these reasons, we do expect some, but not substantial, geographical variability within the region with regard to the early detection and care (and therefore survival) of breast cancer cases.
Fourth, although we know that the latency time between asbestos exposure and pleural cancer is quite long (about 40 years on average), we do not have this information for ovarian cancer. We could speculate that latency could be more similar to that of lung cancer (about 20–30 years), thus leading to differences in age distributions between pleural and ovarian cancer. However, this would be partially compensated by the higher survival (and thus mortality at a later age) of patients with ovarian cancer. In any case, at issue here are the relative geographical distributions of these diseases, and we have no reason to think that these varied much over the time period covered by our study.
The model used in the present paper could help estimate the burden of ARDs with a low aetiological fraction attributable to asbestos, such as ovarian cancer. Notice that disentangling the specific contribution of all the risk factors—asbestos exposure and the other relevant risk factors—is a complex task that simple geographical correlation studies cannot achieve.
Estimating the number of asbestos-attributable cases is of public concern. The need to estimate the global health asbestos impact, including all pathologies certainly associated with asbestos, was reported for both asbestos-banned and no-ban countries; notably, in the latter, the absence of estimates could determine a low public awareness of the health risk of asbestos and delay the ban of its use.25 In countries where asbestos is banned but its health impact is still high, such as Italy, the estimates of ARD cases at the national and local levels furnish helpful information for planning and implementing interventions. The issue of substantial underreporting of asbestos-related diseases is still a real concern for the scientific community, the workers’ health and safety agencies and the insurance system. Our findings may then be used to target interventions of prevention, healthcare, compensation and social support, in particular, to assess occupational exposure in women affected by ovarian cancer residents in areas with high asbestos exposure.
Data availability statement
No data are available. Data were provided by the Italian National Institute of Statistics (ISTAT) and cannot be made available by the authors.
Ethics statements
Patient consent for publication
Ethics approval
Not required.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Guarantor: AB; conceptualisation: CM, DCo, AB and DCa; methodology: GS, AB and DCa; software: GS, AB and DCa; validation: GS, AB and DCa; formal analysis: GS, AB and DCa; investigation: GS, AB and DCa; resources: GM, LF and VM; data curation: GS, GM, VM and DCo; writing the original draft preparation: DCa, LF, AM, AB and GS; writing the review and editing: all authors; visualisation: GS, AB and DCa; supervision: AB and DCa; project administration: CM, AM and LF; funding acquisition: CM. All authors have read and agreed to the published version of the manuscript.
Funding This work was supported by: Italian Workers' Compensation Authority (INAIL), Rome, Italy: BRiC 66/2022.
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests CM and DCo served as consultants in litigations concerning asbestos-related diseases.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.