Article Text

Abstract
Background To estimate the current number of middle meningeal artery embolization (MMAE) procedures for subdural hematomas (SDH) and project growth compared with endovascular treatments for cerebral aneurysms and acute ischemic stroke (AIS).
Methods Estimates of SDH admissions were obtained from the National Inpatient Sample and Medicare Inpatient 100% Standard Analytic Files for 2019–23. MMAE volumes (2019–23) were estimated by cross referencing international classification of diseases, 10th revision, clinical modification (ICD-10 CM) codes for non-acute, non-traumatic SDH with ICD-10 procedure coding system (ICD-10 PCS) codes for surgical and endovascular interventions during the same admission to approximate MMAE volumes. These estimates were compared with volumes of endovascular cerebral aneurysm and AIS treatments, with projections based on historical growth rates.
Results MMAE procedures increased significantly, from 4014 in 2019 to 20 836 in 2023, representing a 51% compound annual growth rate (CAGR). In comparison, endovascular aneurysm treatments grew from 34 754 to 42 491 (5% CAGR) and AIS procedures from 34 451 to 44 822 (7% CAGR). In the next 5 years, MMAE is projected to surpass other neurovascular procedures, with an estimated 79 483 procedures, compared with 79 405 for AIS and 56 942 for aneurysms, by 2029. Annual SDH admissions remained steady at just over 200 000 from 2019 to 2022, with most (~66%) managed medically. Only an estimated 2% of SDH admissions received an MMAE procedure in 2019, rising to 8% in 2022.
Conclusion MMAE procedures have seen rapid adoption and may become the dominant neurovascular intervention, with potential implications for healthcare infrastructure and workforce planning.
- Embolic
- Meninges
- Statistics
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Emerging evidence suggests that middle meningeal artery embolization (MMAE) is becoming a viable treatment for chronic subdural hematomas, with a growing number of procedures expected.
Recent studies highlight that the potential patient population for MMAE could be substantial.
WHAT THIS STUDY ADDS
The number of MMAE procedures currently being performed and their trend over recent years is unclear.
Estimating these procedure volumes is crucial for forecasting future growth and for comparisons with other significant neurovascular interventions.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
As MMAE rapidly gains traction, following promising early clinical trial data, it is essential to define the procedure’s growth and its impact on existing endovascular practice workloads.
Understanding the expanding role of MMAE can guide workforce planning, infrastructure development, and the allocation of healthcare resources for its broader adoption.
Introduction
Emerging data from randomized clinical trials on middle meningeal artery embolization (MMAE) have shown promising results,1–3 suggesting that MMAE is more effective than standard management alone for treating chronic subdural hematomas. A recent study estimated that a population eligible for MMAE could be 41 patients per 100 000 persons per year or almost 140 000 cases annually (95% CI 121 517 to 1 58 168),4 surpassing the estimates for large vessel stroke patients in the same population.5 This finding is particularly significant for the elderly,6–8 who constitute the fastest growing segment of the national population.9 Although MMAE procedures are likely being performed with increasing frequency across the country, there are currently no estimates of the procedure volume or its growth over recent years. Such data are important for planning logistics, addressing workforce needs, and predicting future trends.
As data from recent randomized clinical trials gets disseminated, and given the non-emergent nature, limited requirement of resources, and relative lack of complexity, rapid adoption and growth of MMAE procedures is a reasonable expectation. The primary objective of this study was to estimate the MMAE procedure volumes and growth over the past few years. A secondary objective was to forecast future growth and compare with other major endovascular procedures, such as treatment of cerebral aneurysms and acute ischemic stroke.
Methods
The methodology involved identifying patients hospitalized with a primary diagnosis of chronic subdural hematoma who also underwent an intracranial embolization procedure during their stay. The national estimates for subdural hematoma admissions were generated from the National Inpatient Sample (NIS) data file (Healthcare Cost and Utilization Project, Agency for Healthcare Research and Quality) triangulated with Medicare Inpatient 100% Standard Analytic Files (2019–23 q1–q4). The NIS approximates a 20% stratified sample of discharges from all community hospitals participating in the Healthcare Cost and Utilization Project, excluding rehabilitation and long term acute care hospitals. The NIS covers all patients, including individuals covered by Medicare, Medicaid, or private insurance, as well as those who are not insured.
Estimation of current MMAE embolization procedure volume was conducted by cross referencing the total annual admissions for subdural hematoma identified by international classification of diseases, 10th revision, clinical modification (ICD-10 CM) codes (table 1). Intracranial embolization procedures and surgical drainage performed on these patients during their hospital stay were identified by ICD-10 procedure coding system (ICD-10 PCS) codes (table 2). The Medicare Severity Diagnosis Related Groups (MS-DRG) file was used to capture the MS-DRGs that aligned with the ICD-10 PCS and ICD-10 CM codes for subdural hematomas (MS-DRG 20–22, 25–27). Cases with non-traumatic, no-acute ICD-CM codes and any of the ICD-10 PCS codes (table 2), separated into surgical (drainage or extirpation) and endovascular (occlusion) represented the estimated count of MMAE cases. Of note, national estimates for total subdural hematoma admissions were available up to 2022, while the MMAE numbers were extracted up to 2023.
Description of international classification of diseases, 10th revision, clinical modification (ICD-10 CM) codes for non-traumatic and traumatic subdural hematomas
Description of international classification of diseases, 10th revision, procedure coding system (ICD-10-PCS) surgical and endovascular procedure codes for subdural hematomas
The MMAE procedure volume was compared with the volumes of endovascular cerebral aneurysm and stroke treatments. The growth rates of these procedures were analyzed from 2019 to 2023, with future trends projected from 2024 to 2030. The projections used the historical growth rate of cerebral aneurysm treatments and the estimated growth rate of endovascular stroke treatments from published literature.5 The projected growth rate for MMAE was informed by the observed trend from 2019 to 2023 and modeled after the adoption pattern of endovascular stroke therapy following the publication of multiple positive thrombectomy trials.
Results
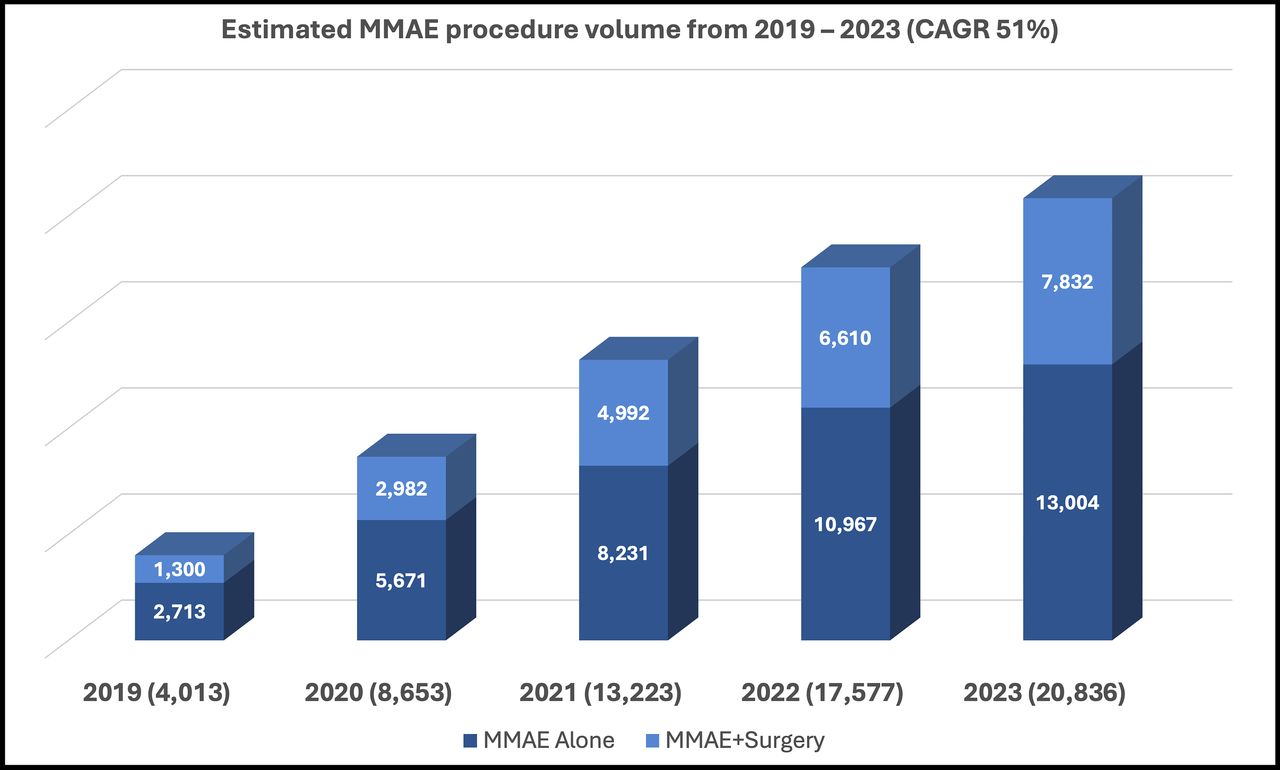
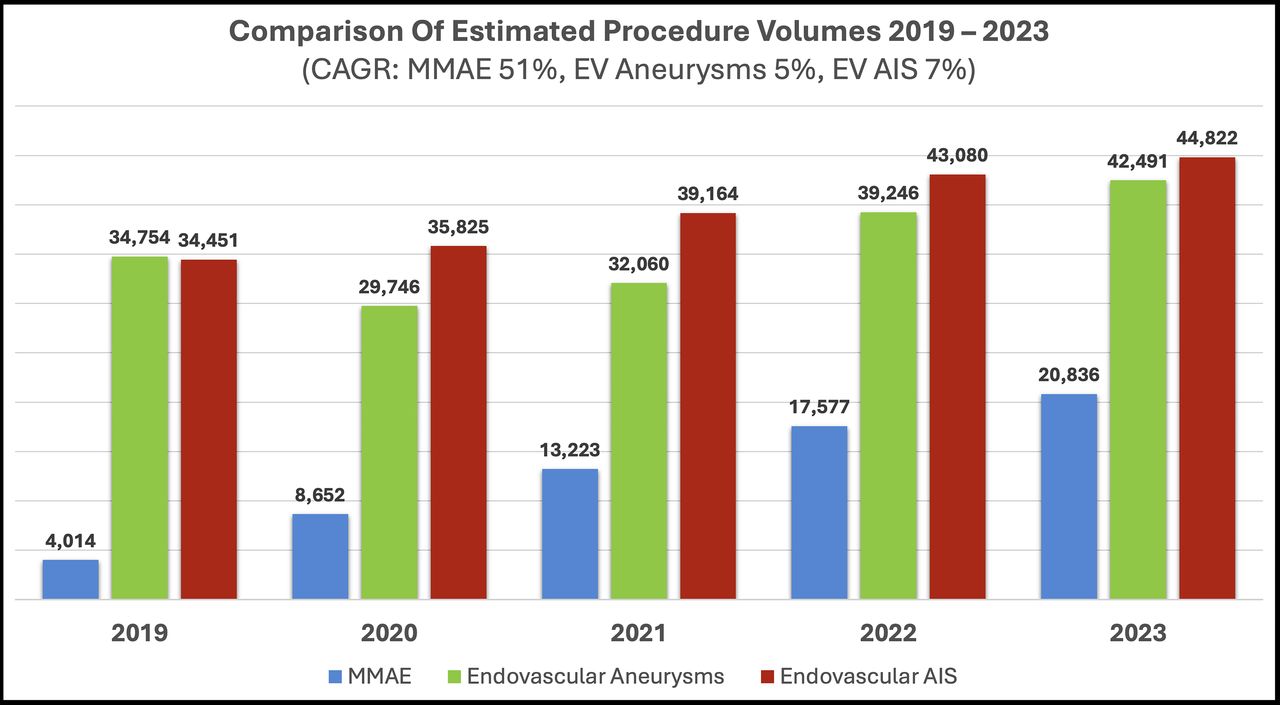
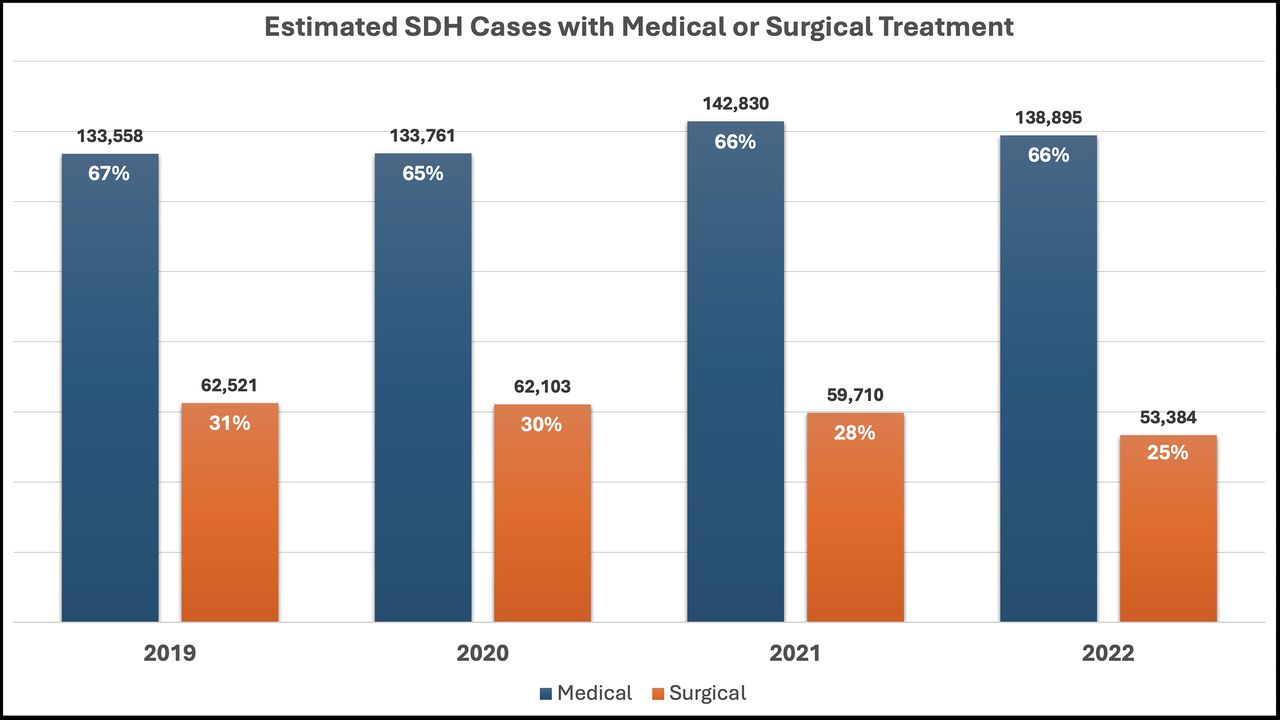
The MMAE procedure volume demonstrated significant growth from 2019 to 2023, both as a standalone therapy and in combination with surgical treatment, achieving a compound annual growth rate (CAGR) of 51% (figure 1). During the same period (2019–23), the estimated volumes of endovascular aneurysm and AIS procedures grew by 5% and 7%, respectively (figure 2). In contrast, the estimated number of all subdural hematoma admissions experienced modest change, with an annual increase of <2% from 2019 to 2022. Most of these patients were managed medically, with approximately one-third undergoing a surgical procedure (figure 3). In 2019, only 2% of all subdural hematoma admissions involved an MMAE procedure, increasing to 4%, 6%, and 8% in 2020, 2021, and 2022, respectively.

Estimated middle meningeal artery embolization (MMAE) procedure volume from 2019 to 2023. Total volume is listed next to the year with the graph showing it broken into either standalone or adjunctive treatment. CAGR, compound annual growth rate.

Estimated volume of middle meningeal artery embolization (MMAE) procedures compared with endovascular (EV) treatment of cerebral aneurysms and acute ischemic stroke (AIS), from 2019 to 2023. CAGR, compound annual growth rate.

Subdural hematoma (SDH) patients undergoing medical or surgical treatment. Total volume of each treatment type and the respective volume as a percentage of all SDH admissions for the given year is listed on each bar.
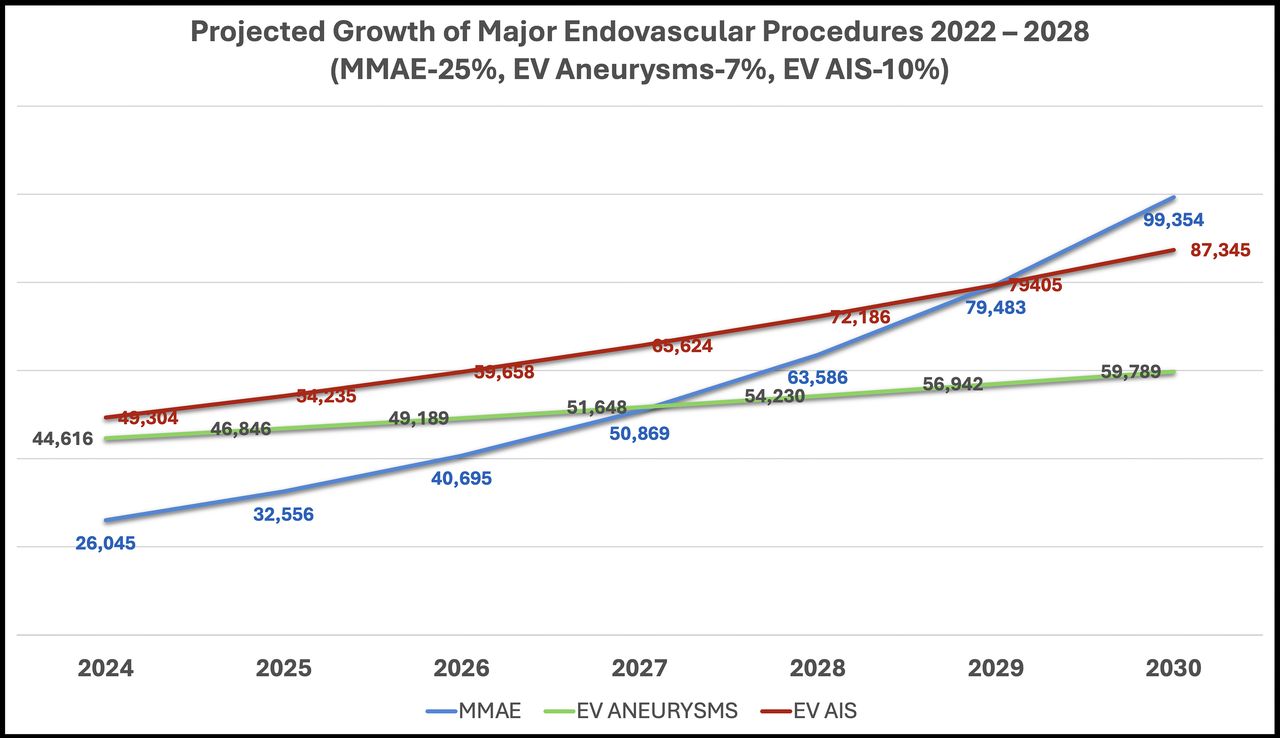
Projected future trends are depicted in figure 4. The 5% annual growth rate for endovascular aneurysm procedures is based on trends observed from 2019 to 2023. This rate is maintained at 5% as no significant treatment breakthroughs or changes in disease incidence are anticipated. In contrast, a 10% growth rate is projected for AIS procedures, up from the 7% observed between 2019 and 2023, to account for potential increases in endovascular treatments for medium vessel occlusions and thrombectomy in patients with large core infarcts. For MMAE procedures, a year-over-year growth rate of 25% is projected, reflecting the rapid increase seen from 2021 to 2023 and modeled after the accelerated growth of AIS procedures between 2015 and 2020 following multiple positive clinical trials.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Projected growth rates of middle meningeal artery embolization (MMAE) compared with endovascular (EV) treatment of cerebral aneurysms and acute ischemic stroke (AIS). An annual growth rate of 25%, 5% and 10% is used for MMAE, EV aneurysms, and EV AIS procedures, respectively.
Discussion
From early reports10–12 to current adoption, MMAE, initially a niche procedure, has now begun to have a more substantial role in neurovascular care. From 2019 to 2023, the estimated number of MMAE procedures increased sharply, both as a standalone treatment and in conjunction with surgical drainage. This increase reflects a shift in practice, where more physicians are considering MMAE as a minimally invasive alternative or adjunct to traditional surgical evacuation. By 2022, 8% of all subdural hematoma admissions received an MMAE procedure, up from just 2% in 2019. As illustrated in the accompanying figures and analysis, the CAGR of MMAE procedures has been impressive between 2019 and 2023. This increase can be attributed to emerging clinical evidence supporting the efficacy of MMAE in treating chronic subdural hematoma, particularly in elderly populations.
In comparison with other major neurovascular interventions, such as endovascular aneurysm and AIS treatments, MMAE has demonstrated a much faster growth rate recently. Projected growth trends suggest this trajectory will continue. Our model used a 25% annual increase in MMAE procedures based on the recent trends in MMAE volume and on the historical growth seen in AIS interventions. It is possible that the growth rate could be lower, and the comparative trajectory with AIS and cerebral aneurysm treatment could be different. Even then, fueled by strong clinical evidence, the relative simplicity of the procedure and its non-emergent nature, the accelerated adoption of MMAE procedures set it up to become the dominant neurovascular intervention in the near future.
The rapid adoption of MMAE may necessitate workforce adjustments for care delivery. The additional volume will need to be absorbed into the workflow of busy neurovascular centers, and the added volume can stress the workforce, especially if cases are pushed to after hours. Staff burnout could lead to attrition and further stress in a vicious cycle. Ensuring adequate coverage in these areas is crucial as the number of procedures increases.
As the figures project, by 2029, the volume of MMAE procedures approaches almost 80 000 annually. This anticipated surge will require healthcare facilities to reassess their capacity and allocate resources accordingly. Hospitals that previously had limited exposure to neurovascular interventions may find it advantageous to invest in expanding their coverage. Additionally, the scalability of MMAE procedures offers opportunities for broader adoption across non-tertiary hospitals, particularly because the procedure is less complex and has lower demands than emergent stroke or aneurysm treatment. The current analysis only tracked inpatient cases, and it is possible that the procedure could be or is being performed as an outpatient treatment, which further adds to the volume. This shift could decentralize neurovascular care, thereby relieving pressure on major stroke centers.
Limitations
This study had inherent limitations due to discrepancies in the coding of subdural hematoma admissions at the hospital level, as well as the lack of specific procedure codes for MMAE. Additionally, while it is theoretically possible that a patient with chronic subdural hematoma received this procedure for another neurovascular condition, it is increasingly likely that the ‘intracranial embolization’ was performed as part of MMAE treatment for the subdural hematoma. These factors may introduce errors in the volume estimates. To minimize these effects, procedure codes pertaining to intracranial embolization procedures were cross referenced with diagnostic codes for non-traumatic, non-acute subdural hematoma admissions. Although it is unlikely that intracranial embolization in subdural hematoma patients was performed for another condition, this possibility remains and could influence the accuracy of the procedure volume estimates. The estimated procedure volume is agnostic to the type of treatment technique or embolic material used and hence does not provide information of these trends. The study was also limited by patients; any outpatient procedures were not accounted for. Lastly, the projected growth was speculative, based on recent trends. It is possible that different growth trajectories could emerge. The data presented here is one estimated scenario of the future neurovascular landscape.
Conclusions
The exponential growth in MMAE procedures reflects both the clinical efficacy and operational feasibility of this treatment for chronic subdural hematomas. As the number of MMAE cases continues to rise, hospitals and healthcare providers must prepare by investing in infrastructure and workforce development. This will be critical to meet the increasing demand and ensure that patients benefit from this advanced, minimally invasive therapy. As MMAE becomes a cornerstone in the management of chronic subdural hematomas, its impact on the neurovascular care landscape is likely to be profound, particularly as it relates to improving outcomes for elderly patients and expanding the scope of neurovascular therapies.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
X @Ansaar_Rai, @dhairyalakhani
Contributors ATR and PSL contributed to the study design and data analysis. PSL contributed to data collection. ATR and DAL contributed to manuscript preparation and review. ATR is the guarantor of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests ATR has consulting agreement with Stryker Neurovascular and Cerenovus.
Provenance and peer review Not commissioned; externally peer reviewed.