Article Text

Abstract
Introduction Severe haemorrhage from the arm that is unresponsive to direct pressure necessitates the application of a tourniquet. Detachable arm protection, referred to as brassards, are used by the UK Armed Forces to protect the upper arm from fragmentation threats. However, the coverage they originally provided was based on limited medical evidence. Medical consensus has determined that the dimensions of arm protection should in future be related to how far up the arm a tourniquet can be applied.
Method CT scans of 120 male Armed Forces personnel were analysed to ascertain the vertical distances from acromion process to the point at which a tourniquet can applied, equating to the anterior axillary fold. These values were statistically compared with those derived from the 2007 UK Military anthropometric survey using a paired t-test. Additional distances were added to account for tourniquet width and slippage, with the total value compared with VIRTUS brassard length.
Results No significant difference (p<0.01) was found in mean acromion to axilla length (114 mm) compared with that found in the anthropometric survey confirming sample validity. The deltoid insertion lay 24 mm below the axillary fold for the 50th percentile value from CT. Essential arm coverage for the 99th percentile male in this study was calculated as 201 mm.
Conclusions Based on this research, a single new brassard for the VIRTUS body armour and load carriage system was recommended and manufactured based on the 99th percentile. This is over 30% shorter than the existing VIRTUS brassard, reducing the overall weight burden for the soldier and improving heat dispersion, integration and interoperability. The new brassard has been issued to Armed Forces personnel since October 2018. The reduced mass of ballistic protective material in conjunction with requiring only a single size of brassard has already saved the Ministry of Defence £20 000 in procurement costs.
- military
- arm
- body armour
- armour
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Severe haemorrhage from the arm that is unresponsive to direct pressure necessitates the application of a tourniquet.
Detachable arm protection, referred to as brassards, are used by the UK Armed Forces to protect the upper arm from fragmentation threats.
The dimensions of a brassard should be determined by how far up the arm a tourniquet can be applied.
The recommended dimensions of the new VIRTUS brassard based from this study is over 30% shorter than the existing VIRTUS brassard.
This has reduced the overall weight burden for the soldier and improved heat dispersion, integration and interoperability.
The reduced mass of required ballistic protective material in conjunction with a single size of brassard is predicted to save £20 000 in procurement costs per year.
Introduction
Requirement for arm coverage
The vast majority of combat casualties with potentially survivable injuries die from haemorrhage.1 Haemorrhage can be controlled in many cases with direct compression in conjunction with a first field dressing and haemostatic agents. Severe haemorrhage from the arm that is unresponsive to the above measures necessitates application of a tourniquet.1 However, there is a limit to how close to the torso that a tourniquet can be applied. Multidisciplinary medical consensus has therefore recommended that the position at which a tourniquet can reliably be applied and tightened should determine the extent that the arm should be covered by ballistic protective materials.2 The limits to how closely tourniquets can be applied to the torso are the anterior and posterior axillary folds of the armpit (Figure 1). However, in practical terms, when tightened the upper margin of the tourniquet will generally slip down the deltoid muscle until it reaches a point level with the insertion of the muscle into the humerus bone.2

The acromion process1 is the recommended landmark for defining the boundary between brassard the outer border of the body armour vest and the upper border of arm protection. A tourniquet can be applied as high as the axillary fold,2 but is likely to slip down the arm to a point level with the deltoid insertion.3
Upper arm protection
Protection of the upper arm from fragmentation threats has been available for use by UK service personnel since the introduction of the KESTREL and OSPREY personal armour systems in 2006.2 This protection has been in the form of integral (non-detachable) brassards for KESTREL and removable brassards that attached using press studs to the body armour vest for OSPREY (Figure 1). In addition, a ‘shoulder guard’ was issued and worn at the back of the brassard to ensure that no projectiles could penetrate between the brassard and vest when the service person had their arms fully extended. Brassards issued as part of the OSPREY body armour system were issued in two sizes.
The VIRTUS personal armour and load carriage system, introduced in 2015, has replaced OSPREY as the personal armour system worn by the high readiness component of the UK Armed Forces.3 VIRTUS uses a single size of brassard, and following recommendations from previous arm coverage work,2 there is no longer a separate shoulder guard component (Figure 2A). However, at the time of procurement, there was no medical evidence to recommend the size of the brassard. The length of the existing VIRTUS brassard (Figure 2B) when first introduced was 300 mm (including the outer carrier material) and 290 mm when excluding the outer carrier but including the soft armour filler and cover (Figure 2C). The length recommendation herein is based on the soft armour length in the brassard as it is the element of the system that provides the fragmentation protection.

Brassard attached to VIRTUS vest (A) brassard cover measured (B) that encloses the ballistic protective material, the ‘soft filler’ which is measured (C).
Anthropometric landmarks
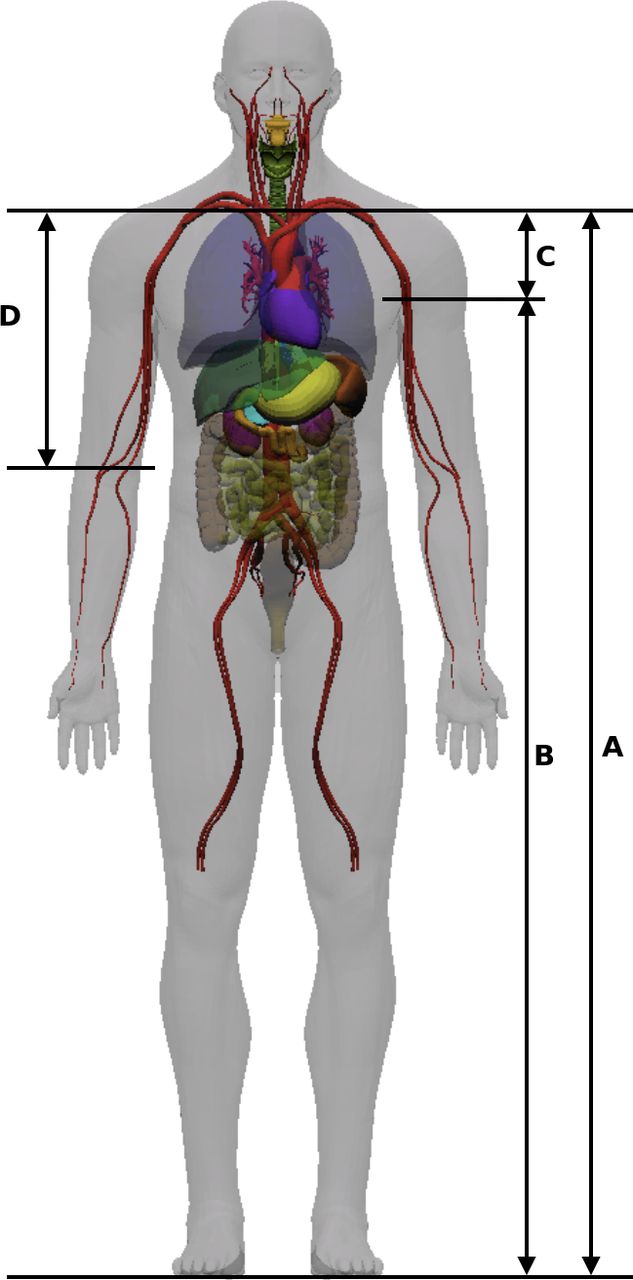
One method of determining the optimal coverage that should be provided by personal armour is to use anthropometric landmarks. These landmarks are stable locations on the human body that are used to delineate the linear measurements required in anthropometry.4–6 These landmarks are also important for accurate sizing and fitting of personal armour.2 4 The acromion of the scapula is a landmark that has been used in previous military anthropometric surveys.7–11 The acromion can be used as the upper border of arm protection, and thereby the junction between it and the body armour vest, as it is one of the points at which the arm and torso articulate. However, previous military anthropometric surveys have generally not measured landmarks applicable to the remainder of arm coverage as they were not deemed a requirement at the time (Table 1). Standing acromion and anterior axilla height were measured in two of the studies, so it is possible to ascertain a limited amount of information on arm coverage by subtracting acromion height from anterior axilla height7 8 (Figure 3).

Linear anthropometric distances measured in military surveys. Acromion height (A) and axilla height (B) can be used to determine vertical acromion to axilla distance (C). Acromion to elbow (D) is of little use in terms of arm coverage.
Deltoid insertion (sometimes termed ‘deltoid point’) was measured in one military survey7 but not in a manner that could be used to determine arm coverage (Figure 4). A single civilian study used an anthropometric measurement of deltoid insertion to acromion length, as part of a segmental measure of upper arm length for assessments of muscle strength12 (Table 1).

Image taken from the 1968 Royal Air Force anthropometric survey7 demonstrating how the value for standing axillary height was determined using a stick held at the level of the anterior and posterior axillary folds (crown copyright). This image demonstrates in particular the difficulty in accurately ascertaining the position of the deltoid muscle insertion clinically (arrowed).
CT scanning
CT scans have the potential to provide information for the sizing of protection and have recently been used successfully for thoraco-abdominal body armour.4 Scans of service personnel taken in recent conflicts will clearly represent a pertinent demographic of those who will potentially be wearing personal armour in the near future. The acromion of the scapula is a readily identifiable bone landmark and can be used as the upper border of arm protection (Figure 5). Both the axillary fold and deltoid insertion can be visualised on CT scans, but the latter is far more subjective.

Screenshots of axial slices from CT scans taken at the levels of potential anthropometric landmarks used to determine arm coverage; acromion process, anterior axillary fold and deltoid insertion.
Rationale for study
The VIRTUS project provided the impetus to define the anatomical coverage provided by arm protection and provide recommendations on how the coverage could be optimised using new medical technology.4 The aims of this research were to use CT scans taken on a pertinent cohort of UK Armed Forces personnel in order to measure the dimensions of anthropometric landmarks on the arm, to recommend sizes of arm coverage and to aid the fitting of brassards onto an individual.
Method
Contrast CT ‘trauma’ scans of 120 consecutive male Caucasian UK Armed Forces personnel evacuated from Iraq and Afghanistan to University Hospital Birmingham (UHB) between 17 June 2009 and 19 March 2013 were identified from the Joint Theatre Trauma Registry. This was supplemented by cross-checking of records held by the Imaging Department of the Royal Centre for Defence Medicine. A total of 156/196 military service numbers identified from these searches could be accurately matched to UHB hospital numbers. 36/156 hospital numbers identified CT scans that could not be accessed from the UHB server. This resulted in 120 scans that were available for analysis.
Distances A and B were measured from CT and distance C was the width of the current Combat Application Tourniquet used by UK forces (Table 2 and Figure 6). Distance A was compared with that derived from the QinetiQ anthropometric UK military survey8 using a paired t-test with a significance level of p <0.05. CT scans were analysed by a single clinician using the IMPAX Dicom imaging program (Agfa, Belgium, V.6.0). This has an intrinsic measuring tool that provides linear distances between two cursor points in millimetres to a single decimal point.
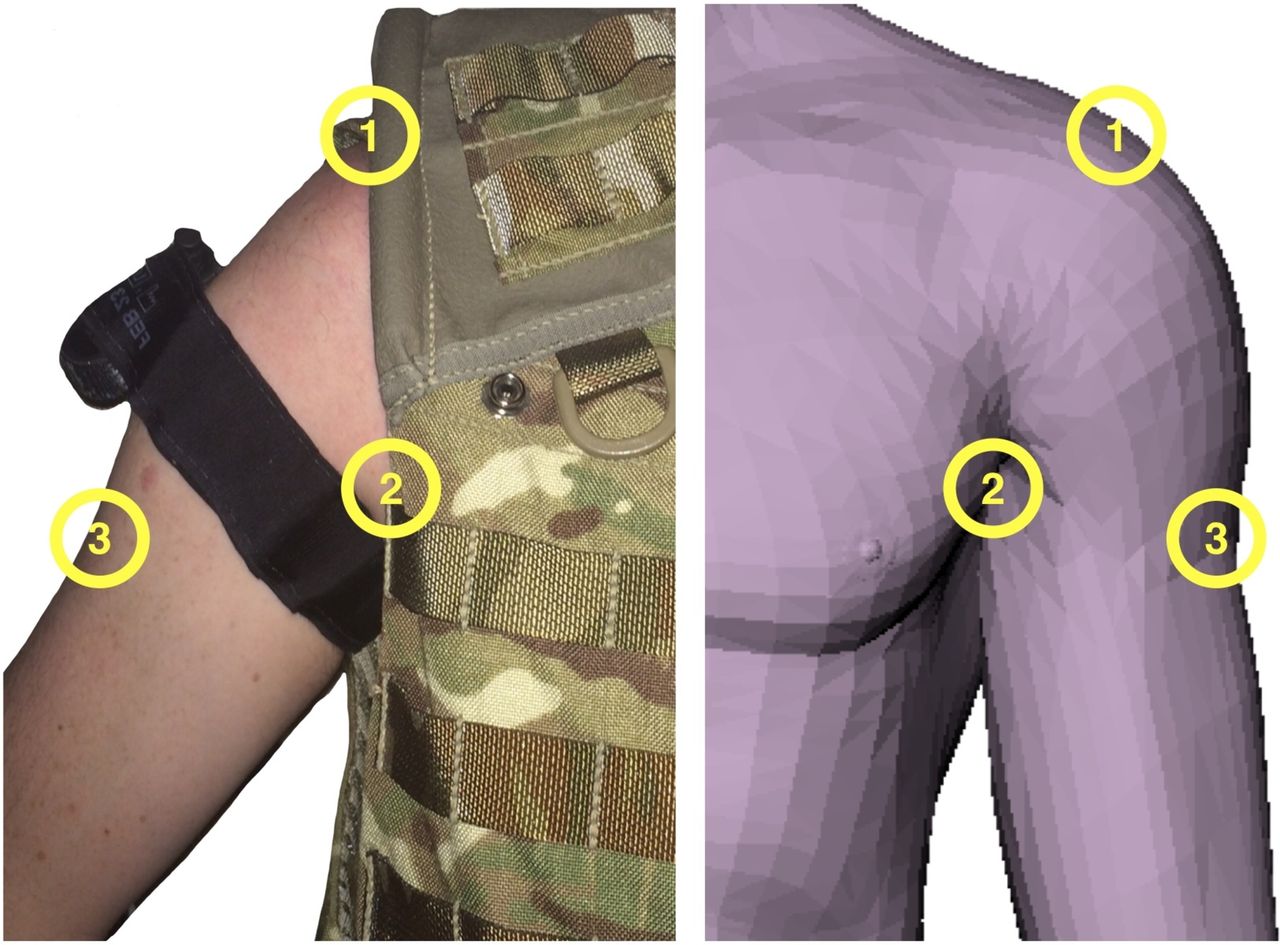
Distances A–C used to determine the recommended length of the brassard (distance D)

Pictorial representation (not to scale) of how distances A–D were ascertained using measurements from CT scans (cross-reference table 2). 1, acromion process; 2, anterior axillary fold; 3, deltoid insertion.
A linear regression from distance A to distance A+B was determined from the CT data. This relationship was then used with the much larger dataset from the UK military anthropometric database8 in order to calculate estimates for distance B for the population as a whole.
Results
No significant difference was found (p<0.05) in the acromion to axillary fold distance derived from the CT scan sample (distance A) compared with the QinetiQ anthropometric study,8 demonstrating that the CT scans were a representative sample (table 3). The anterior axillary fold was visible in all 120 scans but the posterior axillary fold, but the deltoid insertion was only visible in 92 scans (Figure 7).
Arm coverage lengths (in millimetres) for different percentile groups based on CT scans compared with military anthropometric data7 8

Screenshot taken of an axial CT scan demonstrating that the window size used meant that the deltoid muscle insertion and posterior axillary fold was not visible in all scans.
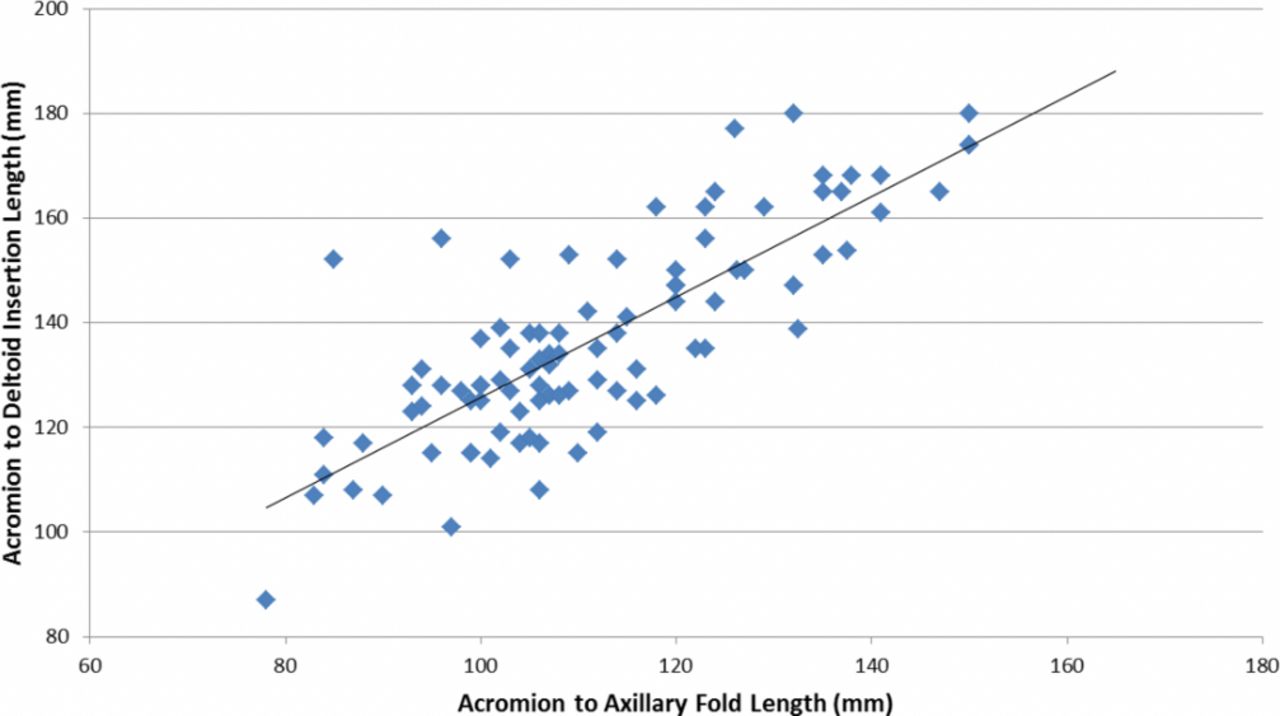
A scatter graph of distance A and distance A+B from the CT data is displayed in Figure 8. A linear regression of distance A to distance A+B was determined from these data and is given by Equation 1:


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatterplot with linear regression fit of distance A compared with distance A+B.
This regression has an R² value of 0.6495, so it shows a reasonable correlation considering human variation. Equation 1 is used in combination with the QinetiQ anthropometric study data to determine the range of percentile coverage lengths for the male population. This is summarised in Table 4.
Coverage lengths determined from the QinetiQ anthropometric study data in combination with Equation 1
Discussion
Anthropometric landmarks to determine essential arm coverage
The aims of this research were to use CT scans taken on a pertinent cohort of UK Armed Forces personnel in order to measure the dimensions of anthropometric landmarks on the arm. The correct sizing and fitting of arm protection requires the identification of anatomical landmarks. Both the acromion process and the anterior axillary fold are important in determining the extent of arm coverage and were measured in the 2007 QinetiQ military anthropometric survey. No significant difference was found in the mean acromion-to-anterior axillary fold distance derived from the CT scan sample compared with the 2007 military anthropometric survey,8 demonstrating that this was a representative sample.
The deltoid insertion is important to measure as it is a useful marker of how far down a tourniquet will slip down the arm in the tactical pre-hospital environment. However, the deltoid insertion can be difficult to measure on a subject both in person and on CT. No pertinent measurements taken using the deltoid insertion have been undertaken in previous military anthropometric surveys likely reflecting this. This coverage analysis has demonstrated the importance of measuring standing acromion height and anterior axilla height and deltoid insertion in future military anthropometric surveys.
Recommendations for arm coverage length
The hypothesis of this paper is that essential coverage of the arm is based on the distance between the acromion and the lower border of the tourniquet, accounting for potential slippage of the tourniquet to the deltoid insertion. It is recommended that this rationale, using standard measurements including tourniquet width, is used in future coverage assessments, including planned consensus regarding coverage of the pelvis and thigh.
Conclusions
Based on this research, a single new brassard for the VIRTUS body armour and load carriage system was recommended and manufactured based on the 99th percentile. This is over 30% shorter than the existing VIRTUS brassard, reducing the overall weight burden for the soldier and improving heat dispersion, integration and interoperability. The first issuing of the reduced sized brassards to UK Armed Forces were in October 2018, with the purchasing of more brassards planned as part of the continued manufacture and issue the VIRTUS system. The reduced area of required ballistic protective material in conjunction with a single size of brassard has already enabled a saving of £20 000 in procurement costs for the Ministry of Defence between October 2018 and the time of submission of this paper in June 2019.
Recommended soft filler length in the brassards based on CT results were compared with those from the QinetiQ anthropometric study for each of the percentile groups (Table 5).
Optimised VIRTUS brassard lengths based on the percentage reduction in length per percentile of the male population
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Approval for undertaking this study was obtained from the Royal Centre for Defence Medicine (reference: 1036.16.0456) and Universities Hospital Birmingham (reference: CARMS-15201). The authors were advised that additional specific Ethical Approval was not required from the Defence Medicine Services Research And Strategy Group (DMS-RASG) as this was a retrospective analysis of data obtained from imaging already undertaken for clinical reasons and no patient-identifiable information was promulgated in the paper.
Footnotes
Contributors All authors were responsible for the design and reporting of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.