Article Text

Abstract
Background The prevalence of MLH1 constitutional epimutations in the general population is unknown. We sought to analyse the prevalence of MLH1 constitutional epimutations in unselected and selected series of patients with colorectal cancer (CRC).
Methods Patients with diagnoses of CRC (n=2123) were included in the unselected group. For comparison, a group of 847 selected patients with CRC who fulfilled the revised Bethesda guidelines (rBG) were also included. Somatic and constitutional MLH1 methylation was assayed via methylation-specific multiplex ligation-dependent probe amplification of cases lacking MLH1 expression. Germline alterations in mismatch-repair (MMR) genes were assessed via Sanger sequencing and methylation-specific multiplex ligation-dependent probe amplification.
Results Loss of MLH1 expression occurred in 5.5% of the unselected series and 12.5% of the selected series (p<0.0001). No constitutional epimutations in MLH1 were detected in the unselected population (0/62); five cases from the selected series were positive for MLH1 epimutations (15.6%, 5/32; p=0.004).
Conclusions Our results suggest a negligible prevalence of MLH1 constitutional epimutations in unselected cases of CRC. Therefore, MLH1 constitutional epimutation analysis should be conducted only for patients who fulfil the rBG and who lack MLH1 expression with methylated MLH1.
- Clinical genetics
- Cancer: colon
- Epigenetics
Statistics from Altmetric.com
Introduction
Lynch syndrome (LS) is an autosomal-dominant disorder that is caused by germline mutations in one of the mismatch repair (MMR) genes (MLH1, MLH2, MSH6 or PMS2).1 No pathogenic mutations in MMR genes have been detected in a variable proportion of suspected LS cases,1 ,2 perhaps due to constitutional epigenetic inactivation of the MMR gene MLH1 in some of these cases.3–5 Constitutional epimutations are characterised by the methylation of cytosine bases located at CpG island in the MLH1 promoter as well as by transcriptional silencing of the affected allele in normal tissues.6 To date, the vast majority of diagnoses of constitutional epimutations have come from selected population recruited from cancer family clinics; no published studies have reported the prevalence of constitutional MLH1 epimutations in non-selected cases of colorectal cancer (CRC). We aimed to investigate the prevalence of MLH1 constitutional epimutations as a cause of LS in unselected consecutive cases of CRC. We compared these data with data from a selected population fulfilling the revised Bethesda guidelines (rBG).
Methods
Patients and samples
The unselected group included 2123 patients with diagnoses of CRC. Of these, 671 patients came from the nationwide multicentre study, EPICOLON II,7 which included all consecutive patients with CRC, newly diagnosed between March 2006 and December 2007; EPICOLON II seeks to investigate various aspects of the diagnosis of hereditary CRC. The other 1452 patients were consecutive patients with diagnoses of CRC from the Hospital General Universitario de Alicante Biobank (1999–2011). For comparison, we also included a group of 847 selected patients with CRC fulfilling the rBG who came from the Hereditary Cancer Program of the Valencian region (Spain) and were recruited between 2005 and 2013. Written informed consent was obtained from all subjects. This study was approved by the Hospital General Elche and Hospital General Alicante Ethics Committees (Spain).
DNA from formalin-fixed, paraffin-embedded material (colorectal tumours, normal colorectal tissue, bladder cancer and normal small bowel tissue), oral epithelium and peripheral blood leucocytes was extracted using the QIAamp DNA Mini Kit and the QIAcube (QIAGEN, Germany). DNA from saliva was collected and extracted with the Oragene-DNA kit (DNA Genotek, Canada).
Analysis of MMR protein expression, microsatellite instability, BRAF mutation in tumours and MMR germline mutations
Immunohistochemical analysis of MLH1, MSH2, MSH6 and PMS2 was performed in all tumours as previously described.8 A panel of five quasimonomorphic mononucleotide repeat markers was amplified in a single multiplex PCR to detect microsatellite instabilities (BAT25, BAT26, NR21, NR24 and NR27). Cases that displayed an altered pattern in at least two of the markers were considered to harbour microsatellite instabilities.
BRAF_V600E mutation analysis was conducted via real-time PCR for the unselected series as previously described9 and via Sanger sequencing of BRAF exon 15 for the selected series. A standard diagnostic algorithm was applied for screening and germline mutation analysis of MLH1, MSH2, MSH6 and PMS2.8
MLH1 methylation
MLH1 somatic methylation was evaluated in tumour tissue from cases lacking MLH1 expression. In cases with somatic methylation of MLH1, putative constitutional epimutations were sought in DNA from blood cells. All available tissue types from positive cases were tested to confirm the constitutional nature of this epimutation. MLH1 methylation was analysed via methylation-sensitive multiplex ligation-dependent probe amplification using the SALSA MS-MLPA Kit ME011 for MMR genes (MRC-Holland, The Netherlands) according to the manufacturer's protocols.
Analysis of MLH1 promoter sequence
Sanger sequencing of the MLH1 promoter was assessed in cases with constitutional epimutations in order to identify promoter variants associated with this particular molecular phenotype. Primers and conditions for PCR are available upon request.
Statistical analysis
Continuous variables are reported as mean±SD for normally distributed data. Categorical variables are reported as frequencies or percentages. Analysis of variance was applied to analyse differences between group means. Significant differences between groups were assessed using the χ2 test for categorical data and the non-parametric Mann–Whitney U test for quantitative data. The Wilcoxon rank test was applied to identify significant differences between the two groups of patients. All reported p values are two-sided, and p<0.05 was considered significant. All calculations were performed using IBM SPSS V.21.0 (USA).
Results
Epidemiological, clinical and pathological data for the unselected and selected series are shown in online supplementary table S1.
MLH1 epimutation analysis in the unselected series
A total of 2123 patients with CRC were included in the unselected group (figure 1A). The median patient age was 71.5 years (IQR: 62.28–78.09 years) and 58% of patients were male.

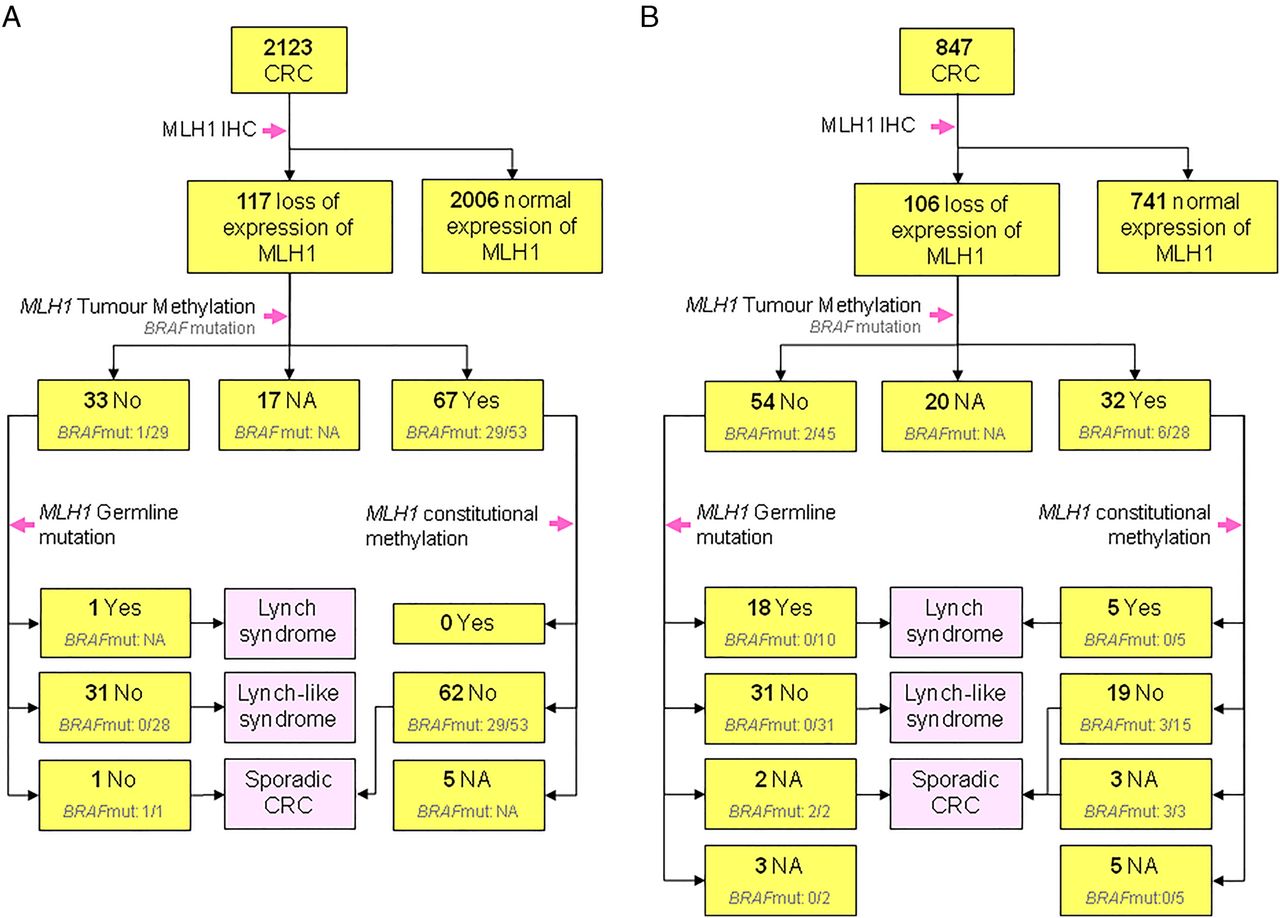{kind=link}
Flow diagram of patients from (A) the unselected group of patients with CRC and (B) the selected group of patients with CRC fulfilling the rBG. CRC, colorectal cancer; IHC, immunohistochemistry; NA, not applicable; rBG, revised Bethesda guideline.
Immunohistochemical analysis of MMR was performed in all tumours. One hundred and seventeen unselected patients (5.5%) did not express MLH1 in their tumours. Of these patients, 67 patients (57.3%) showed somatic MLH1 methylation and 33 patients (28.2%) were considered negative for somatic MLH1 methylation. Tumour samples were not available for 17 patients (14.5%). In 33 cases without somatic MLH1 methylation, 1 germline mutation was found (3%), 1 BRAF mutation was detected (1/33, 3%) and was classified as a sporadic tumour and the other 31 patients (31/33, 94%) were classified as Lynch-like syndrome (loss of MLH1 expression with neither somatic MLH1 methylation nor germline mutation). No constitutional epimutations were found in normal tissue from cases with somatic MLH1 methylation.
MLH1 epimutation analysis in the selected series
The average methylation percentages for MLH1 promoter regions C and D in methylated tumours were 40.62% (SD: 13.33%) and 49.5% (SD: 19.02%), respectively, while the methylation ratios in non-methylated tumours were 4.54% (SD: 8.29%) for region C and 4.35% (SD: 7.88%) for region D (p<0.001; Student's t test).
Eight hundred and forty-seven cases from the Hereditary Cancer Program of the Valencia region in Spain were included (figure 1B). All cases were probands with CRC who fulfilled the rBG. The median age in this group was 49 years (IQR: 43–62 years) and 49.7% were male. One hundred and six selected patients (12.5%) exhibited loss of MLH1 expression in their tumours. Somatic MLH1 methylation was evident in 32 of these patients (30.2%), was not detected in 54 of these patients (50.9%), and analysis was not performed for 20 patients (18.9%) because the BRAF_V600E mutation was previously detected or because the quality of tumour DNA was inadequate. In the group of patients who lost MLH1 expression without exhibiting somatic MLH1 methylation, 18 germline mutations were found (33.3%), 31 patients (57.4%) were classified as Lynch-like syndrome, and 2 patients (3.7%) were considered to be cases with sporadic tumours.
Of the 32 cases with somatic MLH1 methylation, five patients (15.6%) displayed methylation in normal tissue (peripheral blood, normal colorectal mucosa, small bowel normal epithelia and oral mucosa; table 1). All of these cases harboured tumours in the right colon. The age at first diagnosis of CRC in four out of these five cases was below 45 years; all of these patients were male. No first-degree relatives of these four cases had any LS-associated tumours. Case #1 was diagnosed with multiple LS-associated tumours: bladder cancer at 60 years, CRC at 62 years, endometrial cancer at 63 years and pancreatic cancer at 66 years. This case had a sister with gastric cancer diagnosed at 60 years. All five cases had microsatellite instability and no BRAF_V600E mutations in their tumours. The average methylation ratio of the MLH1 promoter (regions C and D) was approximately 50% or above in normal tissues in all cases. No genetic variants were found in the promoter region sequence, with the exception of case #5, who was heterozygous for the polymorphism −93G>A (rs1800734) (table 1).
Characteristics of patients with constitutional epimutations
Comparison of series and comprehensive analysis
The two series significantly differed in terms of age, sex, loss of MLH1 expression in tumours and somatic and constitutional MLH1 methylation. The unselected series was older than the selected series (median 71.5 vs 49 years, respectively; p<0.0001; Mann–Whitney U test) and had a higher proportion of males (58% vs 49.7%, respectively; p=0.001; χ2 test). A lower proportion of tumours with loss of MLH1 expression (OR: 0.408; 95% CI 0.31 to 0.54; p<0.0001; χ2 test) and a higher frequency of somatic MLH1 methylation (OR: 3.43; 95% CI 1.79 to 6.57; p<0.0001; χ2 test) occurred in the unselected series. The median age of patients with MLH1-methylated tumours was higher in the unselected series than in the selected series (77 vs 52 years, respectively; p<0.0001; Mann–Whitney U test). In this subset of cases, 53% and 50% of patients were male in the selected and unselected series, respectively.
No patient with somatic MLH1 methylation in tumour tissue showed constitutional epimutation in the non-selected group (n=62), whereas 5/32 patients (15.6%) in the selected group had constitutional silencing of MLH1 due to methylation (p=0.004, χ2 test).
Discussion
No constitutional epimutations were found in the unselected group of patients with CRC in this investigation. However, 15.6% of patients referred to a genetic counselling clinic due to fulfilment of the rBG with loss of MLH1 expression and somatic methylation of MLH1 in tumour tissue showed constitutional MLH1 epimutation. Constitutional epimutations have been recently described as a rare cause of hereditary non-polyposis CRC.3 ,10 To date, the study of this type of epigenetic alteration has been restricted to patients with CRC with high-risk phenotypes. No study has investigated the prevalence of this genetic alteration in a large series of patients with CRC. This condition was extremely rare in our non-selected CRC population (figure 1A). However, this condition's prevalence was remarkable within a group of selected patients with CRC who fulfilled the rBG and lacked MLH1 expression according to immunohistochemistry (figure 1B).
Family history of cancer in our epimutated cases was scarce, and only one patient had a first-degree relative with LS-associated cancer (table 1). Moreover, none of the relatives of our index cases exhibited MLH1 methylation in their blood, suggesting a de novo mechanism (table 1). Constitutional epimutation is reversible during meiosis and therefore displays non-Mendelian inheritance, in contrast to the autosomal-dominant inheritance pattern associated with mutations in MMR genes.3 ,11 Moreover, some degree of mosaicism has been described in most cases of constitutional MLH1 epimutation.11 However, transgenerational inheritance of cancer susceptibility has also been described.12 In this scenario, risk assessment for relatives is complex; thus, recommendations should be established for the clinical management of all individuals at risk.
In view of the methylation ratio in the core MLH1 promoter (regions C and D) found here, we conclude that all of our cases harbour constitutional monoallelic methylation (table 1). To our knowledge, only one case has been reported to have constitutional biallelic methylation,13 and few cases have been associated with the presence of constitutional hemiallelic methylation.5 Cases #3 and #4 of the present investigation had apparent monoallelic methylation in their tumours, while cases #1, #2 and #5 can be considered to have biallelic methylation due to somatic methylation of the other allele in the tumour (table 1). Somatic point mutations or large rearrangements may account for inactivation of the second allele in cases #3 and #4.
To the best of our knowledge, no previously reported cases with constitutional epimutation carried a BRAF mutation in their tumours. The evidence gathered so far strongly indicates that the presence of a BRAF mutation may exclude the occurrence of MLH1 constitutional epimutation.
It has been suggested that the analysis of constitutional epimutations in MLH1 should be included in the diagnostic algorithm for LS. However, analysis of this type of alteration is not routine in regular genetic clinics, and therefore, constitutional epimutations are likely underdiagnosed. The low frequency of constitutional epimutations, analytical limitations and uncertainty regarding the penetrance of these epimutations, their expression and their mode of inheritance may underlie such suboptimal diagnosis. Our results confirm previous reports of a prevalence of constitutional epimutations of approximately 10% in cases fulfilling the rBG with loss of MLH1 expression and no pathogenic mutations according to standard genetic testing.4 ,5 ,11 ,13 These findings strongly support the routine evaluation of constitutional epimutations in cases fulfilling the rBG that lack MLH1 expression and display MLH1 hypermethylation before considering them to be sporadic CRC cases.
Various studies have suggested the convenience of universal immunohistochemistry for MMR proteins.8 ,14 These analyses improve LS diagnosis, but also lead to an increased number of cases with loss of MLH1 expression and promoter methylation in tumour tissue. However, all previous reports of constitutional MLH1 epimutations were carried out in selected population from high-risk-based registries; this possibility should be investigated in the general population. Our results suggest that the prevalence of constitutional epimutation is negligible in patients with CRC who do not fulfil the rBG, rendering this testing unnecessary in members of the general population who lack cancer history or are aged at the time of diagnosis. However, constitutional epimutation must be included in LS screening of patients who fulfil the rBG, have lost MLH1 expression and harbour somatic hypermethylation of MLH1 in their tumours.
Acknowledgments
We are deeply grateful to the patients who participated in this investigation. We thank the Hereditary Cancer Program of the Valencian region and the EPICOLON consortium.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
AC and EH-I contributed equally to this work and share first authorship.
J-LS and RJ have contributed equally to this work and share senior authorship.
Contributors Conception and design: RJ, J-LS. Development of methodology: AC, EH-I, LP-C, CE, VMB, M-IC, CG, ZG-C, CR-P, AB-F, MJ. Acquisition of data: MR-S, EM-d-D, M-JJ, A-BS-H, LB, JC, XL, MA, AC, AC, CA, AP. Analysis and interpretation of data: AC, EH-I, CA, AP, RJ, J-LS. Writing, review and/or revision of the manuscript: all authors. Study supervision: RJ, J-LS.
Funding This work was supported by the Instituto de Salud Carlos III (PI08/0726, INT-09/208, PI11/2630, INT-12-078, INT13-196, UGP-13-221) and the Asociación Española contra el Cáncer (Fundación Científica GCB13131592CAST). EH-I received a grant from Instituto de Salud Carlos III (FI12/00233) and CG received a predoctoral grant from Conselleria d'Educació de la Generalitat Valenciana (VALi+d. EXP ACIF/2010/018).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethical Committee of the Alicante University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.