Article Text

Abstract
Objective Despite proven effectiveness, participation in traditional supervised exercise-based cardiac rehabilitation (exCR) remains low. Telehealth interventions that use information and communication technologies to enable remote exCR programme delivery can overcome common access barriers while preserving clinical supervision and individualised exercise prescription. This meta-analysis aimed to determine the benefits of telehealth exCR on exercise capacity and other modifiable cardiovascular risk factors compared with traditional exCR and usual care, among patients with coronary heart disease (CHD).
Methods CINAHL, The Cochrane Library, Embase, MEDLINE, PubMed and PsycINFO were searched from inception through 31 May 2015 for randomised controlled trials comparing telehealth exCR with centre-based exCR or usual care among patients with CHD. Outcomes included maximal aerobic exercise capacity, modifiable cardiovascular risk factors and exercise adherence.
Results 11 trials (n=1189) met eligibility criteria and were included in the review. Physical activity level was higher following telehealth exCR than after usual care. Compared with centre-based exCR, telehealth exCR was more effective for enhancing physical activity level, exercise adherence, diastolic blood pressure and low-density lipoprotein cholesterol. Telehealth and centre-based exCR were comparably effective for improving maximal aerobic exercise capacity and other modifiable cardiovascular risk factors.
Conclusions Telehealth exCR appears to be at least as effective as centre-based exCR for improving modifiable cardiovascular risk factors and functional capacity, and could enhance exCR utilisation by providing additional options for patients who cannot attend centre-based exCR. Telehealth exCR must now capitalise on technological advances to provide more comprehensive, responsive and interactive interventions.
Statistics from Altmetric.com
Introduction
Cardiac rehabilitation (CR) is an essential part of contemporary coronary heart disease (CHD) management that aims to optimise cardiovascular risk reduction, facilitate adoption and adherence to healthy behaviours, reduce disability and promote an active lifestyle.1 International guidelines recommend a multidisciplinary approach that includes patient evaluation, medical and lifestyle risk factor management, cardioprotective therapies, psychosocial management, exercise training and health behaviour change education.1 ,2 While programmes comprising exercise training alone are not considered CR, exercise training remains a core component.1 Exercise-based cardiac rehabilitation (exCR) is traditionally delivered in clinical or community settings by physicians, nurse specialists, physiotherapists or clinical exercise specialists,3 and should include individualised and progressive aerobic and strength training. ExCR reduces mortality,1 ,4 can concurrently improve several modifiable cardiovascular risk factors5–8 and is more cost-effective for increasing life expectancy than many common pharmacotherapies and surgical interventions.9
Despite these benefits, referral and uptake of supervised centre-based exCR are inadequate.10 ,11 Common participation barriers include limited programme availability, transport restrictions, inconvenient programme scheduling and domestic or occupational responsibilities.12 ,13 Among those who undertake centre-based exCR, short-term and long-term adherence are poor.14 ,15 Traditional centre-based exCR does not meet the needs of many eligible patients, and innovation is required to enhance utilisation.
Home-based programmes overcome traditional participation barriers12 and provide comparable effects on mortality, recurrent coronary event risk and cardiovascular risk factors,16 but do not provide supervision during exercise or optimally individualised exercise prescription.
Use of information and communication technologies (ICTs) to augment home-based programmes, termed telehealth CR, enables provision of additional feedback, education and counselling. Systematic reviews indicate telehealth CR improves cardiovascular risk factors, health-related quality of life, adverse events and cost-effectiveness;17–19 however, few studies have used telehealth to deliver or monitor structured, individualised, prescriptive exercise training in a manner similar to centre-based exCR.
A recent meta-analysis that compared centre-based exCR with telehealth interventions that included exercise components reported comparable effects on mortality, cardiovascular events, cholesterol, blood pressure, body mass and exercise capacity.20 While promising, telehealth exercise components were predominantly limited to periodic assessment of exercise adherence and high-level exercise prescription, and lacked delivery or monitoring of structured individualised exercise prescription.
Telehealth can combine the accessibility of home-based exCR with the specialist monitoring, interaction and support of centre-based programmes, but the effectiveness of telehealth exCR is not well established. Therefore, the aim of this systematic review and meta-analysis was to determine the effectiveness and safety of structured telehealth exCR on maximal aerobic exercise capacity and modifiable cardiovascular risk factors compared with traditional centre-based exCR and usual care. We did not examine the effects of telehealth exCR on psychosocial well-being.
Methods
Criteria for identifying and selecting study reports, outcomes of interest, methods of data extraction, methods for assessing risk of bias and methods for statistical analysis were prespecified (a protocol was not published).
Eligibility criteria and search methods
Eligible studies were randomised controlled trials (RCTs) comparing secondary prevention outpatient (home-based or community-based) telehealth exCR with usual care or non-telehealth centre-based exCR, among adults (≥18 years) with diagnosed CHD (atherosclerosis, angina pectoris, myocardial infarction or coronary revascularisation). Telehealth exCR interventions used ICT (eg, telephone, mobile/smartphone, mobile application [app], portable computer, Internet, biosensors) to deliver or monitor structured exercise training that included prescriptive components such as frequency, level of intensity and duration. Telehealth and centre-based exercise could be delivered alone or as part of comprehensive CR. Usual care could include standard medical care but not structured, prescriptive exercise training.
Outcomes of interest included maximal aerobic exercise capacity, modifiable cardiovascular risk factors, exercise adherence, mortality and clinical events.
Electronic databases (CINAHL, The Cochrane Library, Embase, MEDLINE, PubMed, PsycINFO) were searched from inception to 31 May 2015 for studies combining three subject areas, telehealth, CHD and exercise. A search strategy was developed for MEDLINE and adapted for other databases (see online supplement 1). Searches were limited to human studies published in English. Conference abstracts and dissertations were ineligible, but authors were contacted to request full-text peer-reviewed manuscripts. Reference lists of included studies and relevant systematic reviews, meta-analyses and conference proceedings identified by the search strategy were hand searched to identify additional studies.
Supplemental material
Data extraction and analysis
Search results were assessed by independent reviewers (JCR and AD), and underwent full-text review if the title or abstract identified the specified population and intervention components. Data describing eligibility, study design, participant characteristics, treatment characteristics, outcome variables, results, risk of bias and sources of funding were extracted by independent reviewers (JCR, AD and CB) using a standardised form. Differences in eligibility assessment or outcome data were resolved by discussion.
Where multiple reports of a single study were included, relevant data were extracted from all reports. Authors were contacted to request information not presented in study reports. When possible, continuous outcomes were transformed onto uniform measurement scales. Metabolic equivalent of task (MET) was transformed to oxygen consumption (1 MET=3.50 mL/kg/min). Cholesterol, triglyceride and glucose concentrations were transformed to mmol/L (1 mg/dL=0.02586 mmol/L, 1 mg/dL=0.01129 mmol/L, and 1 mg/dL=0.05556 mmol/L, respectively). Body mass was transformed to kg (1 lb=0.45359 kg).
Risk of bias was evaluated (JCR and CB) using methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Section 8.5) for assessing the risk of selection, detection, attrition and reporting biases.21 Performance bias was not assessed as participants and treatment delivery personnel could not be blinded to treatment allocation. Published study protocols and clinical trial registry data were sought and, when available, informed risk of bias assessment.21 Blinding and incomplete data handling were assessed at the outcome level if required; remaining domains were assessed at the study level. Risk was judged as high, low, or unclear if data were insufficient or uncertain. The number of included studies was insufficient to detect publication bias via funnel plot asymmetry21 or the influence of risk of bias on pooled outcomes. Heterogeneity was explored qualitatively by comparing study characteristics, and quantitatively using the χ2 test and the I2 statistic.
Data synthesis and analyses were conducted using Review Manager (V.5.3.5, The Nordic Cochrane Centre, Copenhagen) in accordance with the Cochrane handbook.21 Outcome data were sought at post-intervention and long-term follow-up time points. When appropriate, results were pooled across studies using a fixed effect meta-analysis model to yield overall estimates of treatment effects comparing telehealth exCR and usual care, and comparing telehealth and centre-based exCR. Differences between means and 95% CIs were calculated for continuous outcomes. Outcomes that could occur more than once per participant (ie, counts) were treated as continuous outcomes. When unable to obtain continuous data on exercise adherence, methods outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Section 9.4.6)21 were used to combine dichotomous and continuous outcomes.
Differences between standardised means were calculated when pooling outcomes with non-uniform measurement scales. A random effects model was used if statistically significant heterogeneity was identified. This review includes several small trials, which can be overweighted by a random effects model.4 Therefore, if effect estimates remained statistically significant using a random effects model, the fixed effect estimate was reported. Sensitivity analyses to explore heterogeneity and potential treatment effect modifiers were considered inappropriate due to the small number of included studies.
Meta-analyses were stratified by type of comparison group to differentiate effects between actively and passively controlled studies. The threshold for statistical significance was set at α<0.05. Where meta-analysis was inappropriate, individual study findings are summarised narratively. If required, data describing statistical comparisons were calculated manually following accepted methods.21
One multireport study22 re-consented participants for extended follow-up. Due to attrition, subsequent study reports23 ,24 describe subsets of the original sample. This review includes data from the earliest possible report to include the largest proportion of the original sample. The risk of introducing selection bias was low as randomised allocation was maintained throughout, and number and reasons for attrition were balanced.
Results
Description of studies
Database searches identified 1555 study reports. Eleven additional reports were identified by hand searching identified systematic reviews and bibliographies of included studies, and correspondence regarding abstracts and dissertations. After removing duplicates, 102 reports underwent full review; 13 reports,22–34 describing 11 studies (n=1189), met the eligibility criteria and were included in the review and meta-analysis (figure 1). Characteristics of included studies and reasons for exclusions are presented in online supplements 2 and 3, respectively.

Summary of the study selection process. exCR, exercise-based cardiac rehabilitation; RCT, randomised controlled trial.
Telehealth exCR was compared against usual care in six studies,27 ,29–32 ,34 and centre-based exCR in five studies.22 ,25 ,26 ,28 ,33 Nine studies used a two-arm, parallel RCT design.22 ,25 ,27–33 Zutz et al34 included parallel telehealth exCR and usual care arms, plus a matched historic centre-based exCR arm. The non-randomised arm did not meet eligibility criteria and was excluded. Gordon et al26 included centre-based exCR, physician-supervised nurse-case managed and community-based arms. The latter arm did not meet telehealth exCR eligibility criteria and was excluded.
Studies were conducted in Canada,22 ,31 ,34 Australia,33 Belgium,25 Brazil,32 France,27 Korea,29 the Netherlands,28 New Zealand30 and the USA,26 and published between 2002 and 2014. Sample sizes varied from 1534 to 242.22 Mean participant age was 58 years (range=53 to 63 years), and most were male (75%). Participants were recruited via CR programmes,22 ,25 ,28 ,34 hospitals/medical centres29–33 and previous exCR studies.27 Study enrolment occurred 1–222 ,25 ,33 or 3–2430 months after admission for acute coronary syndrome or revascularisation, or after completing a CR programme.27 Six studies did not specify post-event enrolment duration.26 ,28 ,29 ,31 ,32 ,34 Median treatment duration was 3 months (range=1.5–12 months). Only two studies reported longer-term follow-up data at 6 months,33 or 1.5 and 7.2 years post randomisation22; these data are presented narratively.
Commonly used telehealth technologies were fixed-line telephone,22 ,26–29 ,32 ,33 biosensors (accelerometry,25 ,27 ,33 heart rate)28 ,29 ,34 and websites.25 ,28 ,30 ,31 ,33 ,34 Biosensor data were asynchronously uploaded to websites for review by doctors or clinical exercise specialists. Four interventions used computers25 ,27 ,28 ,34 and mobile or smartphones,25 ,29 ,30 ,33 respectively. One intervention used mobile apps.33
Seven telehealth exCR interventions delivered exercise prescription and monitored exercise performance or adherence,22 ,25 ,27–29 ,31 ,34 two delivered exercise prescription only26 ,30 and two monitored exercise adherence only.32 ,33 Among studies that described exercise prescription parameters,22 ,26 ,28 ,29 ,32 ,33 telehealth interventions comprised ≥2 to ≥5 sessions per week, lasting 30–60 min per session. Exercise intensity level typically increased from moderate (40–60% peak capacity) to vigorous (70–85% peak capacity) throughout telehealth exCR programmes, and the predominant exercise mode was walking.
In addition, all telehealth exCR interventions included feedback, education, psychosocial support and/or behaviour change components delivered via fixed-line telephone, short message service (SMS), email, website, online tutorial or online chat. Two telehealth interventions were explicitly designed to emulate traditional models of comprehensive CR.33 ,34 Six interventions included face-to-face consultations before25 or during22 ,26 ,28 ,29 ,32 the programme.
Centre-based exCR programmes comprised 2–3 supervised sessions per week, lasting 30–60 min per session, at light (rating of perceived exertion (RPE)=6–10) to moderate (RPE=11–13; 60–85% peak capacity) levels of intensity. Centre-based exCR programmes were predominantly aerobic in nature; only one study explicitly reported a strength training component.33
Description of usual care varied but typically included encouragement to be physically active without participation in supervised exCR, self-initiated access to CR education classes and psychosocial support.
Assessment of risk of bias
Limited methodological reporting impaired risk of bias assessment in several studies. Five studies were registered in a clinical trials registry25 ,28 ,30 ,31 ,33 and two referred to peer-reviewed protocols.28 ,30 Judgements about risks of bias are presented in online supplement 4.
Six studies described methods for generating and concealing the allocation sequence.22 ,28 ,30–33 Two studies reported blinded outcome assessors,30 ,31 one reported an unblinded design33 and remaining studies provided insufficient information.22 ,25–29 ,32 ,34 Loss to follow-up varied considerably (0–60%). Two studies included 100% follow-up,27 ,32 two conducted intention-to-treat30 ,31 or modified intention-to-treat analyses,25 ,33 four analysed complete cases26 ,28 ,29 ,34 and one multireport study specified intention-to-treat analyses but only described missing data handling procedures in the final study report.22 Missing data handling procedures included multiple imputation after confirming data were missing at random,31 imputation of primary outcome data only22 ,30 ,33 and imputation for participants who were lost to follow-up but not those who withdrew.25
Four studies reported all specified outcomes,26 ,29 ,32 ,34 six did not report all specified outcomes25 ,27 ,28 ,30 ,31 ,33; two did not report all outcomes at all specified time points31 ,33 and one reported unspecified outcomes.22
Additional risks of bias included progressive attrition throughout longer-term follow-up,22 not reporting the primary outcome specified in the study protocol,28 altering a secondary outcome measurement instrument28 and altering the primary outcome.33
Effects of interventions
Maximal aerobic exercise capacity
Seven studies reported maximal aerobic exercise capacity as maximal oxygen consumption ( O2max) or MET. Telehealth exCR was compared with centre-based exCR in four studies22 ,25 ,26 ,28 and usual care in three studies.30 ,32 ,34
O2max) or MET. Telehealth exCR was compared with centre-based exCR in four studies22 ,25 ,26 ,28 and usual care in three studies.30 ,32 ,34
 O2max did not differ between telehealth and centre-based exCR (random effects weighted mean difference (WMD)=0.85 mL/kg/min, 95% CI −1.36 to 3.05, figure 2) or usual care (random effects WMD=3.72, mL/kg/min, 95% CI −1.96 to 9.39, figure 2). There was evidence of statistically significant heterogeneity in the centre-based (I2=78%, χ2=13.87, d.f.=3, p<0.01) and usual care analyses (I2=76%, χ2=8.27, d.f.=2, p=0.02).
O2max did not differ between telehealth and centre-based exCR (random effects weighted mean difference (WMD)=0.85 mL/kg/min, 95% CI −1.36 to 3.05, figure 2) or usual care (random effects WMD=3.72, mL/kg/min, 95% CI −1.96 to 9.39, figure 2). There was evidence of statistically significant heterogeneity in the centre-based (I2=78%, χ2=13.87, d.f.=3, p<0.01) and usual care analyses (I2=76%, χ2=8.27, d.f.=2, p=0.02).

Forest plot for maximal aerobic exercise capacity.
Over the longer term,  O2max was statistically significantly higher 1.5 and 7.2 years after randomisation to telehealth exCR compared with centre-based exCR.22
O2max was statistically significantly higher 1.5 and 7.2 years after randomisation to telehealth exCR compared with centre-based exCR.22
Physical activity level
Five studies reported objective (daily step count,25 ,31 weekly energy expenditure)27 or self-reported physical activity level.30 ,34 Telehealth exCR was compared with centre-based exCR in one study25 and usual care in four studies.27 ,30 ,31 ,34
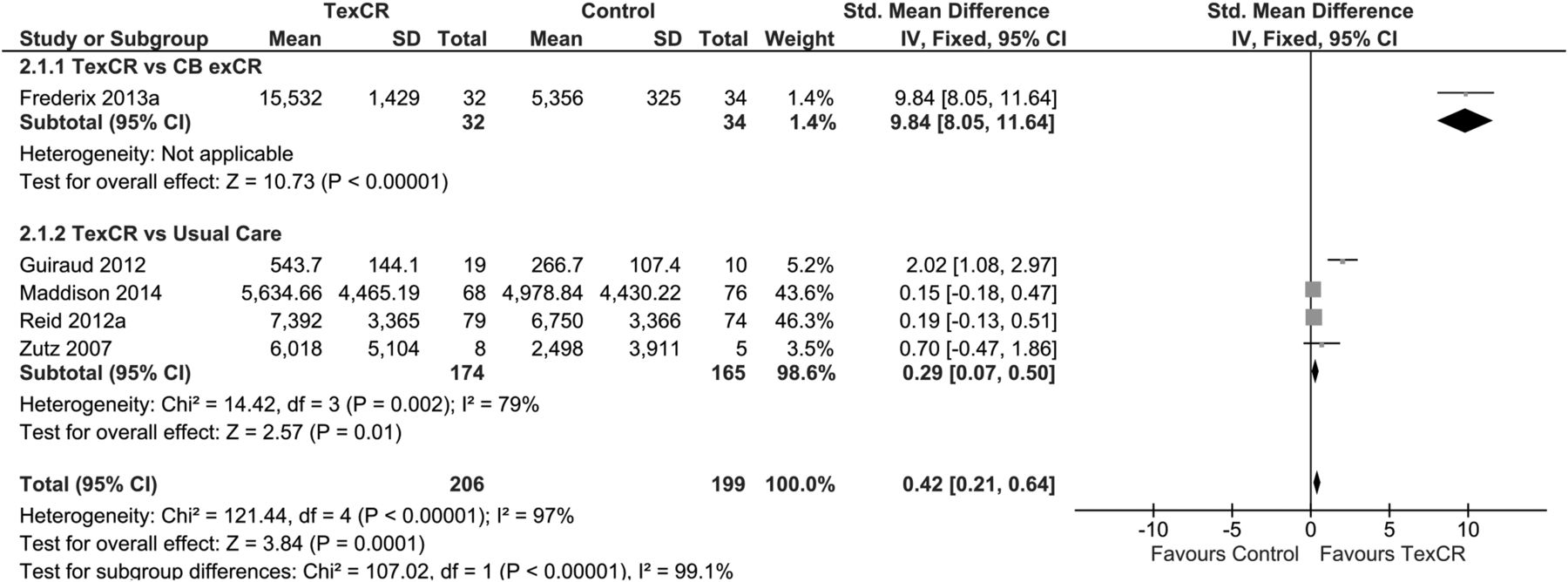
Physical activity level was statistically significantly higher following telehealth exCR compared with centre-based exCR (fixed effect standardised mean difference (SMD)=9.84, 95% CI 8.05 to 11.64, figure 3) and usual care (fixed effect SMD=0.29, 95% CI 0.07 to 0.50, figure 3). There was evidence of statistically significant heterogeneity in the usual care comparison (I2=79%, χ2=14.42, d.f.=3, p<0.01) but the difference remained in a random effects model.

Forest plot for physical activity level; TexCR and CBexCR, telehealth and centre-based exercise-based cardiac rehabilitation, respectively. CBexCR, centre-based exercise-based cardiac rehabilitation; TexCR, telehealth exercise-based cardiac rehabilitation.
At longer-term follow-up, physical activity level was statistically significantly higher at 1.5 years but not 7.2 years after randomisation to telehealth exCR compared with centre-based exCR.22
Exercise adherence
Three studies reported exercise adherence as mean weekly exercise session completion,22 the proportion of participants completing ≥8/12 scheduled exercise sessions33 and the number of exercise sessions completed.28 All studies compared telehealth and centre-based exCR.22 ,28 ,33
Exercise adherence was statistically significantly higher following telehealth exCR (fixed effect SMD=0.75, 95% CI 0.52 to 0.98, figure 4). There was no evidence of heterogeneity (I2=0%; χ2=1.16, d.f.=2, p=0.56).

Forest plot for exercise adherence. CBexCR, centre-based exercise-based cardiac rehabilitation; TexCR, telehealth exercise-based cardiac rehabilitation.
Over the longer term, exercise adherence did not differ between telehealth and centre-based exCR 7.2 years post randomisation.22
Blood pressure
Seven studies reported systolic and diastolic blood pressure. Telehealth exCR was compared with centre-based exCR in three studies25 ,26 ,33 and usual care in four studies.29 ,30 ,32 ,34
Systolic blood pressure did not differ between telehealth and centre-based exCR (random effects WMD=−0.25 mm Hg, 95% CI −3.63 to 3.13, figure 5) or usual care (random effects WMD=−1.97 mm Hg, 95% CI −11.03 to 7.09, figure 5). There was evidence of heterogeneity in the usual care analysis only (I2=75% χ2=12.14, d.f.=3, p=0.01).

Forest plots for systolic (A) and diastolic (B) blood pressure. CBexCR, centre-based exercise-based cardiac rehabilitation; TexCR, telehealth exercise-based cardiac rehabilitation.
Diastolic blood pressure was statistically significantly lower following telehealth exCR compared with centre-based exCR (fixed effect WMD=−4.59 mm Hg, 95% CI −6.91 to −2.27, figure 5) but not usual care (fixed effect WMD=−1.08 mm Hg, 95% CI −3.32 to 1.17, figure 5). There was evidence of moderate heterogeneity in the usual care analysis only (I2=56%; χ2=6.80, d.f.=3, p=0.08).
At longer-term follow-up, blood pressure did not differ between telehealth and centre-based exCR 6 months post randomisation.33
Blood lipids
Four studies reported total cholesterol (total-C), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C), and triglyceride concentrations in mmol/L or mg/dL. Telehealth exCR was compared with centre-based exCR in three studies25 ,26 ,33 and usual care in one study.34
When comparing telehealth and centre-based exCR, there were no differences in total-C (fixed effects WMD=0.03 mmol/L, 95% CI −0.16 to 0.22, figure 6), HDL-C (fixed effects WMD=−0.00 mmol/L, 95% CI −0.08 to 0.07, figure 6) or triglyceride concentrations (fixed effects WMD=−0.03 mmol/L, 95% CI −0.14 to 0.21, figure 6). There was no evidence of heterogeneity for these analyses. LDL-C concentration was statistically significantly lower following telehealth exCR compared with centre-based exCR (fixed effects WMD=−0.15 mmol/L, 95% CI −0.29 to −0.01, figure 6); there was evidence of heterogeneity (I2=68%; χ2=6.21, d.f.=2, p=0.04).

Forest plots for total cholesterol (A), high-density lipoprotein cholesterol (B), triglyceride (C) and low-density lipoprotein cholesterol (D) concentrations. CBexCR, centre-based exercise-based cardiac rehabilitation; TexCR, telehealth exercise-based cardiac rehabilitation.
When comparing telehealth exCR and usual care, there were no differences in total-C (fixed effects WMD=−0.49 mmol/L, 95% CI −1.00 to 0.02, figure 6), HDL-C (fixed effects WMD=0.07 mmol/L, 95% CI −0.30 to 0.44, figure 6), LDL-C (fixed effects WMD −0.38 mmol/L, 95% CI −0.81 to 0.05, figure 6) or triglyceride concentrations (fixed effects WMD=−0.53 mmol/L, 95% CI −1.27 to 0.21, figure 6).
In the longer term, blood lipid concentrations did not differ between telehealth and centre-based exCR 6 months post randomisation.33
Body composition
Six studies reported body composition as body mass index (BMI), body mass, waist and hip circumferences and waist-to-hip ratio. Telehealth exCR was compared with centre-based exCR in four studies22 ,25 ,26 ,33 and usual care in two studies.30 ,34 BMI and body mass were pooled, with BMI in preference to body mass as it is the preferred indicator of cardiovascular risk.35 Additional body composition data are presented in online supplement 5. One study26 reporting changes from baseline could not be included in the pooled analysis of SMDs.21
Body composition did not differ between telehealth and centre-based exCR (random effects SMD=0.15, 95% CI −0.47 to 0.76, figure 7) or usual care (random effects SMD=−0.05, 95% CI −0.34 to 0.41, figure 7). There was evidence of heterogeneity in the centre-based analysis only (I2=86%; χ2=14.22, d.f.=2, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for body composition. CBexCR, centre-based exercise-based cardiac rehabilitation; TexCR, telehealth exercise-based cardiac rehabilitation.
Two studies compared body composition between telehealth and centre-based exCR at longer-term follow-up; Arthur et al22 reported statistically significantly lower body composition 1.5 but not 7.2 years post-randomisation to telehealth exCR; Varnfield et al33 reported no differences between groups 6 months post randomisation.
Blood glucose
Only one study compared blood glucose and glycated haemoglobin (HbA1c) concentrations between telehealth and centre-based exCR.25 There were no differences between groups (see online supplement 5).
Clinical events
Six studies reported clinical events including mortality,31 coronary events,32 cardiac events,30 revascularisation,30 ,31 ,33 rehospitalisation25 ,30 ,31 and total adverse events.28 Telehealth exCR was compared with centre-based exCR in three studies25 ,28 ,33 and usual care in three studies.30–32 Given the heterogeneity of outcomes, a meta-analysis across all studies was not appropriate; individual study data are summarised in online supplement 5; conclusions about treatment effects were not drawn due to the small numbers of events in each study.
Discussion
To our knowledge, this is the first systematic review and meta-analysis to examine the use of telehealth specifically for delivering and monitoring structured, individualised, prescriptive exercise in a CHD population. Eleven RCTs (n=1189) were included in the review. The main findings were that telehealth exCR appears to be at least as effective, and in some cases more effective, for improving cardiovascular risk factors and functional capacity, although there was some evidence of heterogeneity between studies. Characteristics of the telehealth platforms likely influence the intensity of telehealth exCR interventions and may contribute to the variability; the influence of telehealth platform characteristics on intervention delivery and effectiveness warrants further consideration.
Telehealth exCR versus usual care
Compared with usual care, telehealth exCR appears more effective for improving physical activity level, but no differences were observed for other outcomes. As beneficial effects of exCR on exercise capacity, blood pressure, blood lipid concentrations and body composition are well documented8 ,36 ,37 these null meta-analytical effects were unexpected, though not without precedent in the literature.38 The unexpected findings may be partly accounted for by the small number of usual care-controlled studies and characteristics that influence the intensity of telehealth exCR interventions. The small number of included studies may have been insufficient to detect intervention effects. Further, exercise-induced physiological adaptations are usually dose-dependent39 and intervention intensity is likely affected by study-specific characteristics such as exercise prescription, choice and implementation of different telehealth technologies, and intervention engagement or appeal. Characteristics of telehealth exCR interventions in usual care-controlled studies may have provided insufficient intervention intensity to augment the beneficial effects of secondary prevention medications that are routinely prescribed to patients with CHD.
Telehealth exCR versus centre-based exCR
Compared with centre-based programmes, telehealth exCR appears more effective for improving physical activity level, exercise adherence, diastolic blood pressure and LDL-C concentration. No statistically significant differences were observed for other outcomes. These findings are largely consistent with previous comparisons of telehealth CR20 and home-based exCR3 ,38 ,40 against centre-based exCR and provide promising early evidence that telehealth exCR may be a suitable and effective alternative option for patients who are unable or unwilling to attend centre-based programmes.
Higher physical activity and exercise adherence reinforce the potential for telehealth to transform exCR accessibility and promote positive lifestyle behaviour change. Structured, individualised, prescriptive exercise training has traditionally been provided by exercise specialists via centralised clinical facilities; telehealth exCR reverses this paradigm by distributing specialists’ expertise from clinical centres to any location with fixed and/or mobile communications. This simultaneously overcomes common participation barriers, provides opportunities to augment existing home-based interventions and enables scaling of programme availability to meet the needs of many more patients. This is particularly important for rural and remote regions that have difficulty accessing centre-based exCR,41 but will also benefit metropolitan areas by reducing or eliminating travel requirements and allowing more flexible delivery of programme content. Centralised programme delivery may also have economic benefits, but this has yet to be examined.
While the results of this review at times favour telehealth exCR, it is important to note telehealth should be viewed as a complement to existing home- and centre-based exCR rather than as a replacement. Researchers have questioned whether telehealth should become the new standard,42 but there remains demand for centre-based programmes.43 Telehealth exCR is best viewed as an additional option for patients whose needs are not met by existing services. As a complementary option, telehealth exCR can augment home-based programmes, help to broaden the reach of exCR and may also assist patients’ transition from supervised centre-based exCR into sustainable, independent exercise.
Opportunities for future development
By shifting exCR out of clinical settings, telehealth exCR faces substantial challenges to provide monitoring and support that align with international exCR guidelines. Technological advances can enable more comprehensive, responsive and interactive telehealth exCR programme delivery,42 ,44 yet characteristics of the studies included in this review suggest there has been little technological innovation since an early review of telehealth CR in 2009.17 Most interventions were based on telephone counselling, with some use of SMS and email. The utility of biosensors was constrained by asynchronous data uploading that prevented timely monitoring and feedback from exCR specialists. Asynchronous monitoring augments early models of home-based exCR, but technological advances that align with centre-based exCR monitoring practices, enhance safety and guide optimal individualisation of exercise prescription have yet to be capitalised on. Mobile sensor and communication (eg, smartphones) technologies enable real-time remote monitoring of physiological responses and provision of instantaneous feedback during exercise. The capability for exCR specialists to measure exercise parameters and prompt modification of exercise behaviour while participants are exercising would provide substantially greater opportunity to individualise exercise prescription, optimise intervention intensity and enhance dose-dependent health outcomes. Further, patients’ knowledge they were being monitored in real time by exCR specialists may provide reassurance, enhance exercise self-efficacy and enhance social support; this may be particularly beneficial for individuals with low-exercise self-efficacy or anxiety about returning to exercise after a cardiac event.
Some latency can be expected between technological advances, deployment in intervention studies and appearance in the published literature. Several studies have demonstrated the feasibility of real-time remote monitoring technologies for telehealth exCR,13 ,45 ,46 but effectiveness, usability and safety have yet to be assessed in intervention studies. Evaluation studies are currently in progress,47 but realising the potential of existing and emerging technologies remains a priority for the future development of telehealth exCR.
Limitations
Interpretation of the review findings is limited by the small number of included studies, small sample sizes in several studies and methodological limitations of the included studies. Telehealth is a young and rapidly evolving field, and the number of studies evaluating telehealth exCR interventions is likely to increase as technology platforms mature; at least three trials are currently in progress,47–49 although not all include real-time remote exercise monitoring or feedback. Emerging research may help to substantiate the promising findings of this review.
Study methods were often not well described. Several studies were judged to have high risks of bias, although some flaws were unlikely to affect outcomes of interest in this review. Only English-language studies were included; however, language restriction does not bias estimates of intervention effectiveness.50 Several meta-analyses were affected by statistical heterogeneity, possibly due to varying intervention length, frequency and intensity, and telehealth technology utilisation.
Few studies reported longer term follow-up data and the sustainability of telehealth exCR effects remains unclear; however, promising results from individual studies indicate telehealth exCR is at least as effective for sustaining several outcomes of interest. As participants were predominantly male, low-to-moderate risk and relatively young, generalisability to female, higher risk and older-aged individuals is limited.
Conclusions
Telehealth exCR appears to be at least as effective as centre-based exCR for supporting improvements in factors that contribute to cardiovascular risk and functional capacity, and simultaneously overcomes common barriers that limit participation in centre-based programmes. Telehealth exCR could enhance exCR utilisation by providing additional options for patients whose needs are not met by existing services. The challenge is now to capitalise on advances in mobile sensor and communication technologies that enable more comprehensive, responsive and interactive intervention delivery.
References
Footnotes
Twitter Follow Jonathan Rawstorn at @jrawstorn
Contributors JCR, NG and RM designed the review. JCR, AD and CB screened articles and extracted the data. JCR analysed the data. All authors contributed to the interpretation of results, manuscript preparation and final approval. RM and JCR are co-authors on one included study.30 Decisions regarding eligibility for inclusion, risk of bias and data extraction were verified independently by AD and CB. We (authors) accept accountability for all aspects of the work.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This review summarises results from previously published research. Individual study data can be extracted from original publications; some unpublished data were obtained from study authors.