Article Text

Abstract
Objective To assess the benefit of arthroscopic partial meniscectomy (APM) in adults with a meniscal tear and knee pain in three defined populations (taking account of the comparison intervention): (A) all patients (any type of meniscal tear with or without radiographic osteoarthritis); (B) patients with any type of meniscal tear in a non-osteoarthritic knee; and (C) patients with an unstable meniscal tear in a non-osteoarthritic knee.
Design Systematic review and meta-analysis.
Datasources A search of MEDLINE, Embase, CENTRAL, Scopus, Web of Science, Clinicaltrials.gov and ISRCTN was performed, unlimited by language or publication date (inception to 18 October 2018).
Eligibilitycriteria Randomised controlled trials performed in adults with meniscal tears, comparing APM versus (1) non-surgical intervention; (2) pharmacological intervention; (3) surgical intervention; and (4) no intervention.
Results Ten trials were identified: seven compared with non-surgery, one pharmacological and two surgical. Findings were limited by small sample size, small number of trials and cross-over of participants to APM from comparator interventions. In group A (all patients) receiving APM versus non-surgical intervention (physiotherapy), at 6–12 months, there was a small mean improvement in knee pain (standardised mean difference [SMD] 0.22 [95% CI 0.03 to 0.40]; five trials, 943 patients; I2 48%; Grading of Recommendations Assessment, Development and Evaluation [GRADE]: low), knee-specific quality of life (SMD 0.43 [95% CI 0.10 to 0.75]; three trials, 350 patients; I2 56%; GRADE: low) and knee function (SMD 0.18 [95% CI 0.04 to 0.33]; six trials, 1050 patients; I2 27%; GRADE: low). When the analysis was restricted to people without osteoarthritis (group B), there was a small to moderate improvement in knee pain (SMD 0.35 [95% CI 0.04 to 0.66]; three trials, 402 patients; I2 58%; GRADE: very low), knee-specific quality of life (SMD 0.59 [95% CI 0.11 to 1.07]; two trials, 244 patients; I2 71%; GRADE: low) and knee function (SMD 0.30 [95% CI 0.06 to 0.53]; four trials, 507 patients; I2 44%; GRADE: very low). There was no improvement in knee pain, function or quality of life in patients receiving APM compared with placebo surgery at 6–12 months in group A or B (pain: SMD 0.08 [95% CI −0.24 to 0.41]; one trial, 146 patients; GRADE: low; function: SMD −0.08 [95% CI −0.41 to 0.24]; one trial, 146 patients; GRADE: high; quality of life: SMD 0.05 [95% CI −0.27 to 0.38]; one trial; 146 patients; GRADE: high). No trials were identified for people in group C.
Conclusion Performing APM in all patients with knee pain and a meniscal tear is not appropriate, and surgical treatment should not be considered the first-line intervention. There may, however, be a small-to-moderate benefit from APM compared with physiotherapy for patients without osteoarthritis. No trial has been limited to patients failing non-operative treatment or patients with an unstable meniscal tear in a non-arthritic joint; research is needed to establish the value of APM in this population.
Protocol registration number PROSPERO CRD42017056844.
- knee
- arthroscopy
- meniscus
- meniscectomy
- arthroscopic
- systematic review
- meta-analysis
- meniscal
Statistics from Altmetric.com
Introduction
The meniscus is a fibrocartilaginous structure within the knee joint and is important for load distribution and knee stability.1 2 More than one-third of people over the age of 50 years without any radiographic evidence of osteoarthritis have meniscal pathology detectable on MRI, rising to over 60% for individuals with osteoarthritis.3 Meniscal tears may be stable or unstable mechanically and may be symptomatic or asymptomatic.3–6 When a meniscal tear is considered the cause of symptoms, surgical treatment to excise the unstable meniscal tissue is frequently recommended.7 This procedure, arthroscopic partial meniscectomy (APM), has become the most commonly performed orthopaedic surgical procedure worldwide and approximately 2 million cases are performed each year, with combined costs of several billion US dollars.8
Although the rate of knee arthroscopy being performed for osteoarthritis has decreased over the last 20 years, there has been an overall increase in the rate of APM being performed in patients (with or without osteoarthritis) over the same period.9–14 The intervention rate has been challenged following the publication of recent clinical effectiveness studies, especially as meniscectomy is not an entirely benign procedure and may be associated with rare but serious complications.15–20 Some have recommended against arthroscopy in ‘nearly all patients’ with ‘degenerative knee disease’ and suggest that further research is not required.21 However, given the heterogeneity of the population, others have highlighted the importance of patient selection criteria to achieve treatment success with APM, as symptoms may often be caused by an underlying degenerative process and not the meniscal tear.3 22 23 In this situation, symptoms would not be expected to be relieved by APM, and surgery should only be targeted at meniscal tears that are believed to be the direct cause of pain.23 24 However, does any evidence exist to suggest that treatment in the latter case would be effective or ineffective?
There is international consensus from specialist knee societies regarding the patient selection factors that are important in the management of patients with meniscal tears in contemporary practice.23 25 Arthroscopy in patients with significant or end-stage osteoarthritis is not advised.23 25 APM is now only recommended in patients with an ‘unstable’ pattern of meniscal tear visible on MRI that corresponds with meniscal (‘mechanical’) type symptoms.23 25 Furthermore, the current recommendation is that in nearly all cases, APM should only be performed in patients who have failed a period of non-surgical treatment.18 23 26 Previous systematic reviews have evaluated undifferentiated ‘arthroscopy’ (combining lavage, debridement and APM trials) for the degenerative knee.16 27–29 This evidence supports the current view that this approach to treatment is outdated and no longer recommended.23 25 Nevertheless, specifically for APM, there appears to be some conflict when considering published guidelines: on one side, the view that APM in the right patient is effective, and on the other side, the view that APM in all patients with degenerative meniscal tears is ineffective.21 23
In light of the differing views and the impact of this clinical condition on such a large number of patients, there is a need to appraise the evidence for APM in the management of meniscal tears with specific emphasis on areas of uncertainty.30 The aim of this systematic review is to analyse the current evidence regarding the comparative effectiveness of APM with stratification by comparator intervention and the key clinical and radiological assessment criteria.
Methods
This systemic review was conducted following the methods of the Cochrane Handbook for Systematic Reviews and reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement.31 32 The protocol for this review was published on PROSPERO on 22 February 2017.
Study eligibility criteria
Participants
We included studies of adults (18 years of age and older) with meniscal tears of the knee. We excluded studies of individuals with other injuries to the knee (eg, ACL ligament injury and fracture), previous surgery to the knee (eg, ligament reconstruction and arthroscopy) or anatomical variants (eg, discoid meniscus).
Three population groups with knee pain and a meniscal tear were considered: (A) all patients (any type of meniscal tear with or without radiographic osteoarthritis); (B) patients with any type of meniscal tear in a non-osteoarthritic knee; and (C) patients without osteoarthritis and with an unstable meniscal tear as defined by symptoms (meniscal or ‘mechanical’ symptoms – author definition) and the pattern of the meniscal tear on MRI imaging (author definition). These groups were defined based on consensus statements summarising the important stratification factors relevant to patients with meniscal tears, where group C represents the ‘ideal candidate’ for APM.23 Severity of osteoarthritis is recognised as a key selection factor and, in accordance with published consensus, osteoarthritis was defined radiographically as Kellgren-Lawrence grade 2 or greater changes on a plain x-ray radiograph of the knee (or equivalent).16 23 33 Although mechanical symptoms and unstable meniscal tears have been defined and investigated by several groups, there remains some variability in published definitions.4 5 23 34–36 Therefore, for the purposes of this review, study author definitions of these terms were accepted for inclusion in group C. Table 1 summarises the characteristics of the three population groups considered.
Characteristics of population groups evaluated
Intervention
We included studies of APM as the primary intervention. We excluded studies of open or ‘total’ meniscectomy.
Comparators
We included studies with the following comparators, which were analysed separately: (1) non-surgical (eg, physiotherapy and exercise therapy); (2) pharmacological (eg, non-steroidal anti-inflammatory drugs [NSAIDS], intra-articular steroid injection); (3) surgical (eg, arthroscopic lavage, diagnostic arthroscopy, sham surgery and placebo surgery); and (4) no intervention (eg, waiting list and active monitoring). We excluded studies with other surgical intervention comparators (eg, open meniscectomy, meniscal repair, allograft or implant transplantation and chondroplasty). Placebo surgery was defined as diagnostic arthroscopy with omission of partial meniscectomy as the ‘critical element’.24 Sham surgery was defined as a procedure requiring an anaesthetic and surgical skin incision but without any knee arthroscopy procedure (diagnostic, washout and other) being performed.
Outcomes
The primary outcomes assessed were knee function and knee pain, as measured using a validated patient-reported outcome measure (PROM) (eg, Lysholm knee scale and Knee injury and Osteoarthritis Outcome Score [KOOS] pain scale, respectively).37 Secondary outcomes assessed, where reported, were knee-specific quality of life (eg, KOOS quality of life and Western Ontario Meniscal Evaluation Tool) and generic health-related quality of life (eg, EuroQol five dimensions questionnaire [EQ-5D]), presence of knee ‘mechanical symptoms’ (eg, subdomain Lysholm or Meniscal Symptom Index) and activity level (eg, Tegner); number of individuals requiring repeat surgery (eg, further arthroscopy and knee replacement); and number of individuals developing complications (eg, venous thromboembolism, infection and mortality). Outcomes were assessed at 6–12 months (midterm) follow-up. If both 6-month and 12-month data were reported, the 12-month data were included in the meta-analysis. In addition, analysis of early (under 6 months) and long-term (over 12 months) outcome was performed where data were available.
Information sources and search strategy
A search of MEDLINE, Embase, CENTRAL, Scopus and Web of Science was performed (24 March 2017 and updated 12 April 2018; 18 October 2018), unlimited by language or publication date. The search was designed and performed by an independent librarian; full details are available in online supplementary appendix 1. Clinical trial registries (clinicaltrials.gov and ISRCTN) were searched to identify ongoing and recently completed studies. Randomised controlled trials (RCTs) (including quasirandomised) were eligible for inclusion. Cohort studies with a comparator group were also identified but not included in the meta-analysis. When no trial was identified (group C), the cohort evidence was reviewed in this context.
Supplemental material
Study selection and data extraction
The title and abstract of the search results was screened by two authors (SGFA and APM/LEB). The full-text articles were retrieved for all studies meeting the inclusion criteria. Where there was disagreement on inclusion of a study based on the title and abstract, the full-text article was retrieved, and inclusion was decided by consensus.
Data were extracted using a previously piloted data extraction form. Data items extracted included study design, study centres and location, length of follow-up, funding source and conflicts of interest, inclusion and exclusion criteria, number of randomised participants, number lost to follow-up, number analysed, baseline demographics including age and gender, details of the intervention and comparator delivered. Final value outcome data were extracted for the primary and secondary outcomes.
Risk of bias
Studies meeting the inclusion criteria were formally evaluated for risk of bias using the Cochrane ‘risk-of-bias tool’, assessing for selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias (including baseline imbalance and cross-over).38 Two authors (SGFA and SH) assessed each of the included studies and each potential source of bias was graded as high, low or unclear risk of bias; any disagreements were resolved by consensus.38
Data synthesis
Meta-analyses were undertaken where studies were considered sufficiently clinically and methodologically similar and reported for the relevant population group. Where studies met criteria for inclusion, but published data were inadequate for meta-analysis, study authors were contacted to request appropriate summary or raw data for inclusion. In addition, unpublished subgroup data were requested from the authors of included studies. Data were analysed separately to compare the effects of APM versus each of the main comparator interventions: (1) non-surgical (eg, physiotherapy and exercise therapy); (2) pharmacological (eg, NSAIDS and intra-articular steroid injection); (3) surgical (eg, arthroscopic lavage, diagnostic arthroscopy, sham surgery and placebo surgery); and (4) no intervention (eg, waiting list and active monitoring).
The standardised mean difference (SMD) with 95% CIs was used to pool the results of individual trials for continuous outcomes measured using different scales. When interpreting the magnitude of effects using SMD, we used the index thresholds recommended by Cohen.39 The MD and 95% CIs were used for pooling continuous outcomes measured using the same scale. When considered appropriate, we used a random effects model to pool for results of comparable groups of trials in a meta-analysis. Scales were transformed if required to ensure that a higher score indicated a better outcome. If the SD or mean was not reported in the original article, where possible, it was calculated from the reported data, obtained directly from the study authors, or estimated using established methods.31 40
Summary of findings tables
A summary of findings table was constructed for the two comparisons with more than one trial: APM versus non-surgical intervention (physiotherapy), and versus surgical intervention (placebo surgery and sham surgery). The outcomes included were: knee function, knee pain, knee-specific quality of life and generic quality of life. Grading of Recommendations Assessment, Development and Evaluation (GRADE) considerations (risk of bias, consistency of effect, imprecision, indirectness and publication bias) were assessed and used to summarise the quality of the study evidence that contributed data to each outcome.41
Change between the protocol and published review
Following data extraction, as the majority of studies reported patient-reported pain separately from function, rather than reporting complete composite scores (eg, KOOS-5), we modified our analysis plan to more comprehensively report pain, function and quality of life outcomes separately. Similarly, the majority of studies reported either 6-month or 12-month outcome data (not both) and defined long-term follow- up as greater than 12 months. Therefore, to provide a more complete picture of early, medium and long-term outcomes, we modified the time point at which outcomes were reported to: under 6 months, 6–12 months and over 12 months, respectively. One included study did not perform MRI in all patients prior to randomisation (Gauffin et al 2014).42
Results
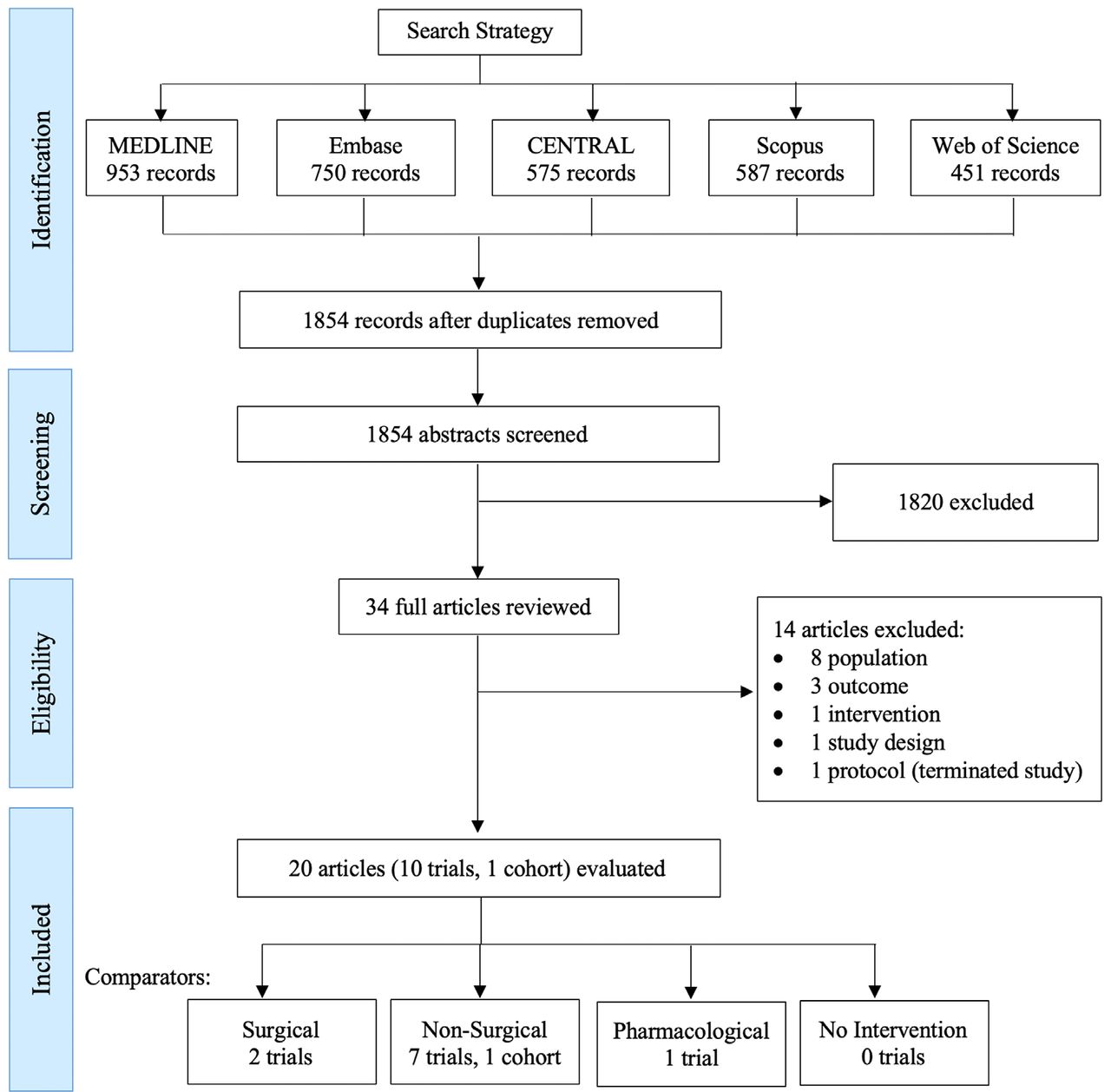
The search strategy identified 1854 unique articles for screening. After screening, 34 full-text articles were retrieved, of which 20 articles (reporting 11 studies) were eligible for evaluation. Ten studies were RCTs (published in 19 articles) and one was a cohort study (1 article). The study selection process is summarised in the PRISMA flow diagram (figure 1). Excluded studies are listed in online supplementary appendix 2. Unpublished data were requested from the authors of all included studies for inclusion in group B or group C, with data subsequently provided for group B by the authors of four studies (Gauffin et al, Kise et al, Roos et al and van de Graaf et al).42–45 The search of clinical trial registries identified three ongoing studies (see online supplementary appendix 3).46–50
Supplemental material
Supplemental material

PRISMA flow diagram full search strategy may be found in online supplementary appendix 1.
Seven RCTs (Herrlin et al, Katz et al, Osteras et al, Yim et al, Gauffin et al, Kise et al and van de Graaf et al)42 43 45 51–54 compared the effects of APM versus non-surgical interventions. One RCT (Vermesan et al 55) compared the effects of APM versus pharmacological interventions. Two RCTs (Sihvonen et al and Roos et al 35 44) compared the effects of APM versus surgical interventions.43 44 No studies were identified comparing the effects of APM versus no intervention. The characteristics of the included studies are summarised in table 2. Full details of the inclusion, exclusion criteria, delivery of the intervention and comparator interventions, location and funding are included in online supplementary appendix 4.
Supplemental material
Study characteristics and risk of bias assessment
APM versus non-surgical interventions
Study characteristics
Eight studies (seven RCTs and one cohort study) were identified, including a total of 1186 participants randomised with a mean age ranging from 47 years to 58 years.42 43 45 51–54 All RCTs included a physiotherapy comparator (intervention delivered for between 6 weeks and 3 months) with follow-up ranging from 3 months to 60 months (table 2). All seven RCTs were eligible for analysis in group A; data from four RCTs (after receipt of unpublished data) excluding patients with osteoarthritis were eligible for analysis in group B.
Risk of bias
All seven RCTs were rated at high risk of performance and detection bias due to a lack of blinding. The method of random sequence generation was unclear in four RCTs, and allocation concealment was unclear in four (table 2). One RCT was rated at high risk of attrition bias due to greater than 10% loss to follow-up. Five were rated at high risk of bias due to cross-over rates exceeding 10% of non-surgical participants (other bias) (table 2).
Knee pain
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis)
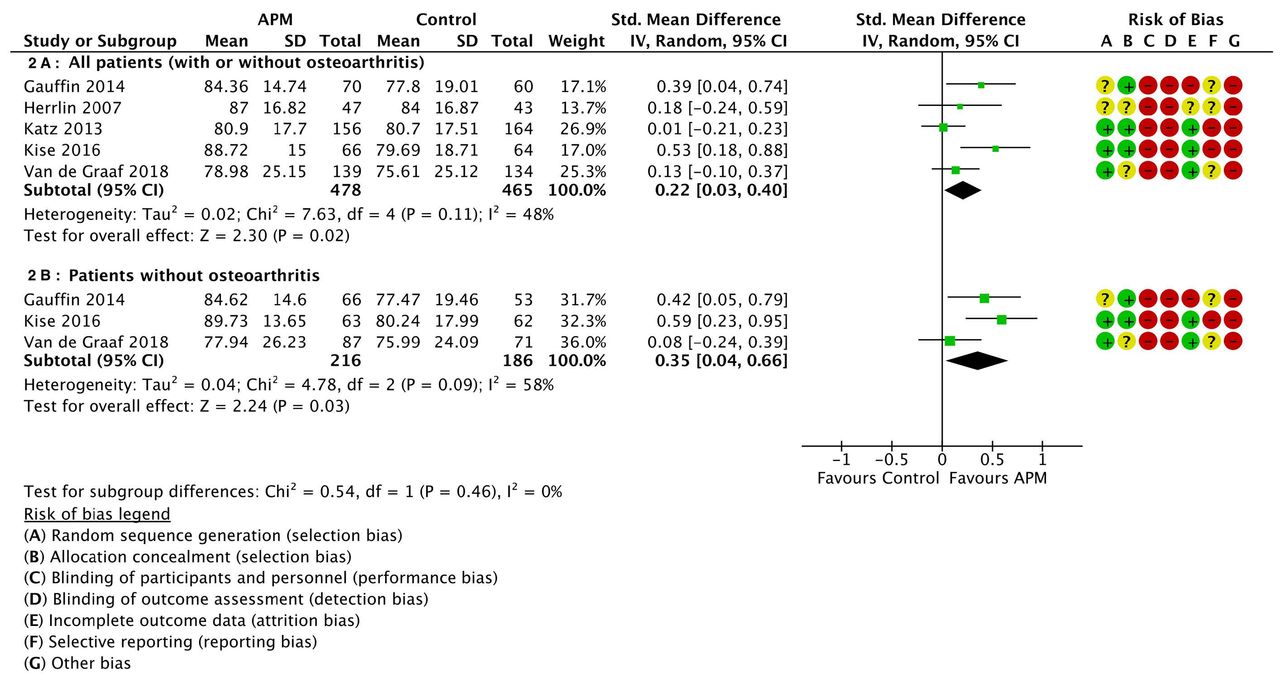
There was a small improvement in knee pain following APM compared with physiotherapy at 6–12 months (SMD 0.22 [95% CI 0.03 to 0.40]; five trials, 943 patients; I2 48%; GRADE: low) (figure 2A). This is the equivalent of a MD of 4.10 KOOS (95% CI 0.74 to 7.46), measured using the KOOS pain scale, where the Minimal Clinically Important Difference (MCID) is estimated to be around 8–10.56 57 There was no difference at under 6 months (SMD 0.18 [95% CI −0.00 to 0.37]; two trials, 434 patients; I2 0%; GRADE: very low) but a small improvement at over 12 months (SMD 0.22 [95% CI 0.04 to 0.40]; three trials, 484 patients; I2 0%; GRADE: very low) (table 3; online supplementary appendix 5).
Supplemental material

Pain following arthroscopic partial meniscectomy (APM) versus non-surgical intervention (6–12 months).
Summary of findings: APM versus non-surgical comparators
(B) Patients with any type of meniscal tear in a non-osteoarthritic knee
There was a small to moderate improvement in knee pain following APM compared with physiotherapy at 6–12 months (SMD 0.35 [95% CI 0.04 to 0.66]; three trials, 402 patients; I2 58%; GRADE: very low) (figure 2B). This is the equivalent of a MD of 6.91 [95% CI 2.87 to 10.94], measured using the KOOS pain scale, where the MCID is estimated to be around 8–10.56 57 There was also no difference at under 6 months (SMD 0.16 [95% CI −0.25 to 0.57]; two trials, 306 patients; I2 68%; GRADE: very low) or over 12 months (SMD 0.21 [95% CI 0.00 to 0.42]; three trials, 368 patients; I2 0%; GRADE: very low) (table 3; online supplementary appendix 5).
(C) Patients with an unstable meniscal tear in a non-osteoarthritic knee
One cohort study was identified in patients undergoing physiotherapy, with patients still complaining or unsatisfied on completion of treatment being offered APM.58 This cohort reported failure of physical therapy in all 50 included patients after a period of 8 weeks due to no significant change in visual analogue pain scores (VAS). All 50 patients subsequently opted to undergo APM, and a significant improvement in patient-reported pain was reported at average 12.5-month follow-up.
Knee function
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis)
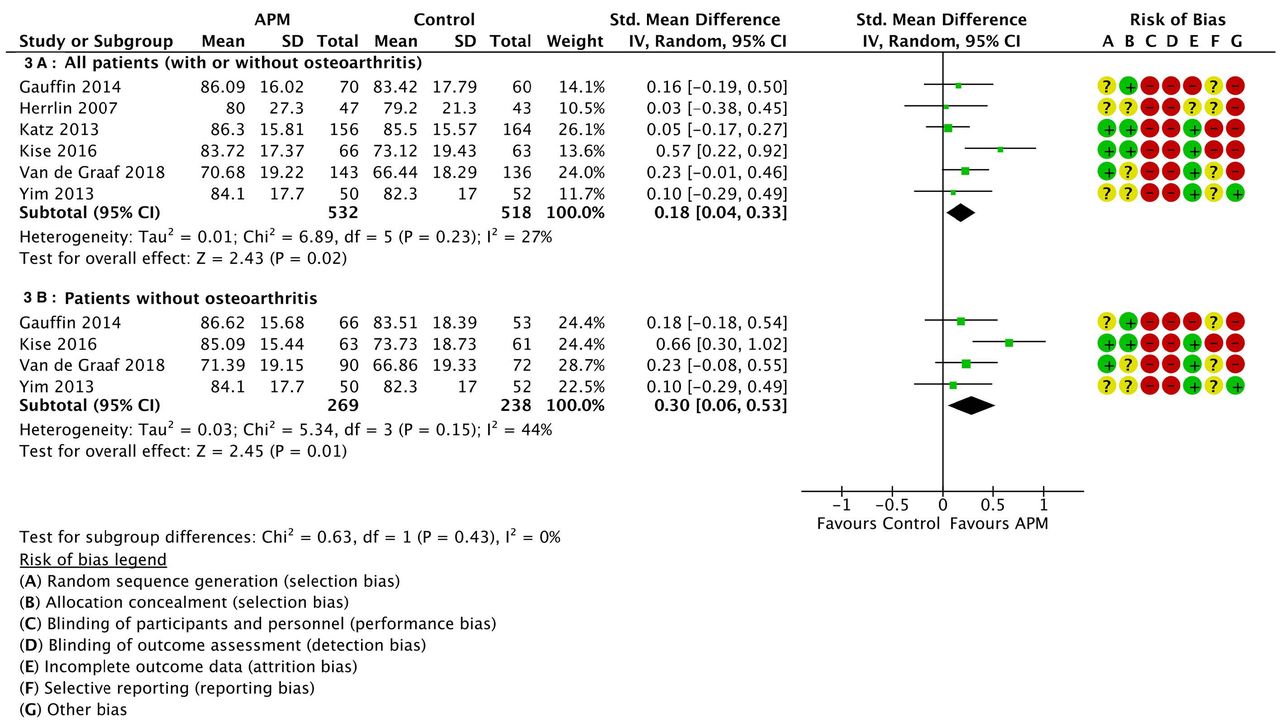
There was a small improvement in knee function following APM versus non-surgical treatment at 6–12 months (SMD 0.18 (95% CI 0.04 to 0.33); six trials, 1050 patients; I227%; GRADE: Low) (figure 3A), equivalent to a MD 3.36 (95% CI 0.55 to 6.16), measured using the Lysholm scale, where the MCID is estimated to be around 8–10 as measurement properties are similar to KOOS.56 57 59 There was no difference at under 6 months (SMD 0.08 (95% CI −0.08 to 0.25); four trials, 561 patients; I2 0%; GRADE: Low) but a small improvement at over 12 months (SMD 0.18 (95% CI 0.04 to 0.33); five trials, 730 patients; I2 0%; GRADE: Low) (table 3; online supplementary appendix 5).

Function following arthroscopic partial meniscectomy versus non-surgical intervention (6–12 months).
(B) Patients with any type of meniscal tear in a non-osteoarthritic knee
There was a small to moderate improvement in knee function following APM versus non-surgical treatment at 6–12 months (SMD 0.30 (95% CI 0.06 to 0.53); four trials, 507 patients; I244%; GRADE: Very low) (figure 3B), equivalent to a MD of 5.31 (95% CI 1.12 to 9.51), measured using the Lysholm scale, where the MCID is estimated to be around 8–10 as measurement properties are similar to KOOS.56 57 59 There was also no difference at under 6 months (SMD 0.11 (95% CI −0.13 to 0.35); three trials, 411 patients; I2 33%; GRADE: Low) but a small improvement at over 12 months (SMD 0.19 (95% CI 0.01 to 0.36); four trials, 501 patients; I2 0%; GRADE: Low) (table 3; online supplementary appendix 5).
(C) Patients with an unstable meniscal tear in a non-osteoarthritic knee
One cohort study was identified with patients undergoing a physiotherapy programme, with patients still complaining or unsatisfied after completion of this treatment being offered APM.58 In this study, the authors defined an unstable meniscal tear using previously published MRI-based radiological criteria and also corresponding positive McMurray test on clinical examination.4 58 This cohort reported failure of physical therapy in all 50 included patients after a period of 8 weeks due to no significant change in function (Lysholm knee scale). All 50 patients subsequently opted to undergo APM, and a significant improvement in patient-reported function was reported at average 12.5-month follow-up.
Knee specific and generic quality of life
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis)
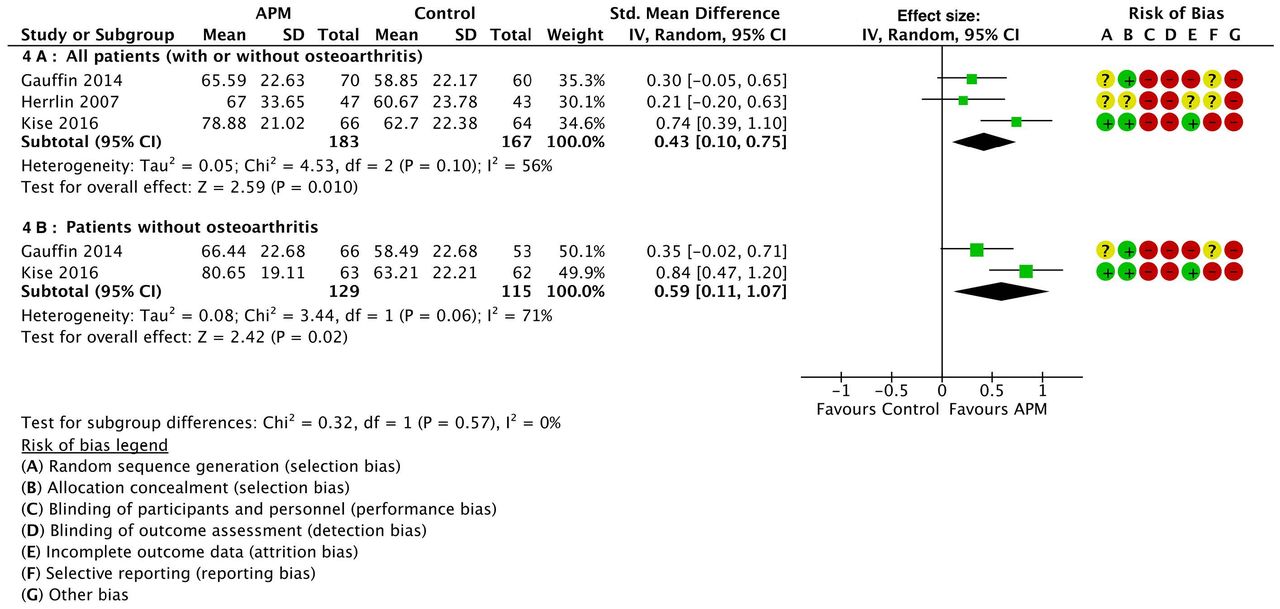
There was improvement in knee-specific quality of life following APM compared with non-surgical treatment at 6–12 months (SMD 0.43 [95% CI 0.10 to 0.75]; three trials, 350 patients; I2 56%; GRADE: low) (figure 4A). This is the equivalent of a MD of 10.36 [95% CI 3.58 to 17.14], measured using the KOOS quality of life scale, where the MCID is estimated to be around 8–10.56 57 There was also improvement at under 6 months (SMD 0.45 [95% CI 0.10 to 0.80]; one trial, 129 patients; GRADE: low) and a small to moderate improvement over 12 months (SMD 0.30 [95% CI 0.05 to 0.56]; two trials, 245 patients; I2 0%; GRADE: very low) (table 3; online supplementary appendix 5). There was no difference in generic quality of life following APM versus non-surgical treatment at 6–12 months (SMD 0.01 [95% CI −0.34 to 0.35]; MD 0.00 EQ-5D [95% CI −0.06 to 0.06]; one trial, 130 patients; GRADE: low), but a small to moderate improvement was reported at over 12 months (SMD 0.47 [95% CI 0.10 to 0.85]; MD 0.10 EQ-5D [95% CI 0.02 to 0.18]; one trial, 113 patients; GRADE: very low) (table 3). For EQ-5D, an MCID of 0.15 is proposed.60

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knee-specific health-related quality of life following arthroscopic partial meniscectomy (APM) versus non-surgical intervention (6–12 months).
(B) Patients with any type of meniscal tear in a non-osteoarthritic knee
There was a moderate to large improvement in knee-specific quality of life following APM compared with non-surgical treatment at 6–12 months (SMD 0.59 [95% CI 0.11 to 1.07]; two trials, 244 patients; I2 71%; GRADE: low) (figure 4B). This is the equivalent of a MD of 12.89 [95% CI 3.60 to 22.18], measured using the KOOS quality of life scale, where the MCID is estimated to be around 8–10.56 57 There was also a moderate to large improvement at under 6 months (SMD 0.52 [95% CI 0.16 to 0.87]; one trial, 124 patients; GRADE: low) and over 12 months (SMD 0.39 [95% CI 0.13 to 0.65]; two trials, 231 patients; I2 0%; GRADE: low) (table 3; online supplementary appendix 5). There was a no improvement in generic quality of life at 6–12 months (SMD 0.06 [95% CI −0.30 to 0.42]; MD 0.01 EQ-5D [95% CI −0.05 to 0.08]; one trial; 119 patients; GRADE: low), but a moderate to large difference was reported at over 12 months (SMD 0.63 [95% CI 0.23 to 1.02]; MD 0.13 EQ-5D [95% CI 0.05 to 0.21]; one trial, 105 patients; GRADE: very low) (table 3). For EQ-5D, an MCID of 0.15 is proposed.60
APM versus pharmacological comparators
Study characteristics
One RCT comparing APM with intra-articular steroid injection was identified, including 114 randomised patients with a mean age of 58 years (table 2; online supplementary appendix 4).55 Patients were followed up at 1 month and 12 months, and only the Oxford Knee Score (pain and function) and repeat operation data were reported. This RCT included patients with osteoarthritis was therefore only eligible for analysis in group A.
Risk of bias
A summary of the risk of bias assessment is shown in table 2. This study was rated at high risk of performance and detection bias due to a lack of blinding. The method of random sequence generation and allocation concealment was unclear. The rate of loss to follow-up was 14.0% (n=16/114), and therefore the trial was rated at high risk of attrition bias. The trial was also rated at high risk of bias due to a cross-over rate exceeding 10% of non-surgical participants (20.8%; other bias).
Knee pain and function
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis)
There was no improvement following APM versus intra-articular steroid injection at 6–12 months (SMD 0.38 [95% CI −0.02 to 0.78]; one trial; 98 patients; GRADE: low). This corresponds to an MD of 1.40 (95% CI −0.07 to 2.87), using the Oxford Knee Score from 0 (severe symptoms) to 48 (no symptoms), where a MCID of 5 points is proposed for patients with osteoarthritis.61 There was a moderate to large improvement at under 6 months (SMD 0.82 [95% CI 0.41 to 1.23]; MD 2.90 Oxford Knee Score [95% CI 1.50 to 4.30]; one trial; 98 patients; GRADE: low).
(B) Patients with any type of meniscal tear in a non-osteoarthritic knee and (C) Patients with an unstable meniscal tear in a non-osteoarthritic knee
No trials were identified.
Other outcomes
See online supplementary appendix 6.
APM versus surgical interventions
Study characteristics
Two RCTs (Sihvonen et al and Roos et al) were identified, including a total of 190 participants’ randomised with a mean age of 52 years and 46 years, respectively.43 44 One RCT (Sihvonen et al)62 compared the effect of APM versus placebo surgery (diagnostic arthroscopy). The other RCT Roos et al compared the effect of APM versus sham surgery (skin incisions only) (table 2).44 Available study data for both RCTs excluded patients with osteoarthritis and were eligible for analysis in group A and group B.
Risk of bias
A summary of the risk of bias assessment for the included studies is shown in table 2. One study Roos et al 44 was rated at high risk of bias due to a high proportion (36%) of patients randomised to the comparator intervention ‘crossing-over’ to undergo APM before final follow-up (other bias).
Knee pain
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis) and (B) patients with any type of meniscal tear in a non-osteoarthritic knee
There was no improvement in knee pain in those patients who received APM compared with those who received placebo surgery at 6–12 months (SMD 0.08 [95% CI −0.24 to 0.41]; one trial, 146 patients; GRADE: low). This is the equivalent of a MD of 2.00 [95% CI −5.69 to 9.69] measured using the KOOS pain scale from 0 (worse) to 100 (better) where a minimum clinically important difference (MCID) is estimated to be around 8–10.56 57 There was also no improvement in knee pain in comparison with sham surgery at under 6 months (SMD 0.26 [95% CI −0.41 to 0.93]; one trial; 35 patients; GRADE: low). At over 12 months, there was a moderate to large improvement in patients receiving APM in comparison with sham surgery (SMD 0.72 [95% CI 0.02 to 1.42]; one trial, 34 patients; GRADE: low) equivalent to a MD of 17.50 (95% CI 1.16 to 33.84) measured using the KOOS pain scale. There was no improvement in comparison to placebo surgery (SMD 0.00 [95% CI −0.33 to 0.33]; MD 0.00 KOOS pain [95% CI −8.35 to 8.35]; one trial; 144 patients; GRADE: low) or combining the placebo and sham surgery trials (SMD 0.29 [95% CI −0.40 to 0.99]; two trials, 178 patients; I2 70%; GRADE: very low) (table 4; online supplementary appendix 5).
Summary of findings: APM versus surgical comparators
(C) Patients with an unstable meniscal tear in a non-osteoarthritic knee
No trials were identified.
Knee function
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis) and (B) patients with any type of meniscal tear in a non-osteoarthritic knee
There was no improvement in knee function following APM compared with placebo surgery at 6–12 months (SMD −0.08 [95% CI −0.41 to 0.24]; one trial, 146 patients; GRADE: high); equivalent of a MD of −1.55 (95% CI −7.95 to 4.66) measured using the Lysholm scale from 0 (worse) to 100 (better), where the MCID is estimated to be around 8–10 as measurement properties are similar to KOOS.56 57 59 There was also no improvement versus sham surgery at under 6 months (SMD 0.07 [95% CI −0.60 to 0.73]; one trial; 35 patients; GRADE: low). At over 12 months, there was no improvement in participants receiving APM in comparison with sham surgery (SMD 0.63 (95% CI −0.06 to 1.32]; MD 12.2 Lysholm [95% CI −1.16 to 25.6]; one trial, 34 patients; GRADE: low) or placebo surgery (SMD −0.18 [95% CI −0.51 to 0.14]; MD −3.49 Lysholm [95% CI −9.89 to 2.72]; one trial; 144 patients; GRADE: low). Combining placebo and sham surgery trials, there was no difference at over 12 months (SMD 0.16 [95% CI to −0.62 to 0.95]; two trials, 178 patients; I2 77%; GRADE: very low) (table 4; online supplementary appendix 5).
Knee-specific and generic quality of life
(A) All patients (any type of meniscal tear with or without radiographic osteoarthritis) and (B) patients with any type of meniscal tear in a non-osteoarthritic knee
There was no improvement in knee-specific quality of life following APM compared with placebo surgery at 6–12 months (SMD 0.05 [95% CI −0.27 to 0.38]; one trial, 146 patients; GRADE: high). This is the equivalent of a MD of 1.10 (95% CI −5.64 to 7.84) measured using the KOOS quality of life scale from 0 (worse) to 100 (better), where the MCID is estimated to be around 8–10.56 57 There was also no difference at under 6 months in comparison with sham surgery (SMD 0.25 [95% CI −0.42 to 0.91]; one trial; 35 patients; GRADE: low). At over 12 months, there was no improvement in participants receiving APM in comparison with sham surgery (SMD 0.65 [95% CI −0.04 to 1.35]; MD 16.50 KOOS quality of life [95% CI −0.27 to 33.27]; one trial, 34 patients; GRADE: low) or placebo surgery (SMD −0.01 [95% CI −0.34 to 0.32]; MD −0.20 KOOS quality of life [95% CI −6.27 to 5.87]; one trial; 144 patients; GRADE: low). Combining placebo and sham surgery trials, there was no difference at over 12 months (SMD 0.25 [95% CI −0.39 to 0.88]; two trials, 178 patients; I2 65%; GRADE: very low) (table 4; online supplementary appendix 5). There was no improvement in generic health-related quality of life following APM versus placebo surgery at 6–12 months (SMD 0.23 [95% CI −0.09 to 0.56]; one trial, 146 patients; GRADE: high), equivalent to a MD of 0.02 [95% CI −0.01 to 0.05], measured using EQ-5D, where the MCID is estimated to be around 0.15.60 There was no improvement versus sham surgery at under 6 months (SMD 0.37 [95% CI −0.30 to 1.04]; one trial; 35 patients; GRADE: low) or over 12 months (SMD 0.69 [95% CI −0.01 to 1.38]; one trial; 34 patients; GRADE: low).
Other outcomes
See online supplementary appendix 6.
APM versus no intervention
No trials were identified for inclusion in this group.
Discussion
This systematic review examined the effectiveness of APM with a methodology that stratified trials by comparator intervention and patients by the important clinical and radiological findings as defined by international consensus groups, for the first time.23 63 Findings were limited by small sample size, small number of trials and cross-over of participants to APM from comparator interventions. At 6–12 months, in trials with a non-surgical comparator, there was a small benefit in favour of APM for pain, knee-specific quality of life and function in studies including patients with osteoarthritis. Excluding patients with osteoarthritis, there was a small to moderate benefit in pain, knee-specific quality of life and function. The clinical importance of these differences is, however, uncertain. In one trial of APM versus a pharmacological comparator (intra-articular steroid injection), no difference in pain and function was detected. In trials of APM versus surgical comparators (placebo or sham surgery), no MD was detected. In the one trial with a placebo surgery comparator, the MD did not exceed a threshold for clinical importance. In the one trial with a sham surgery comparator, no MD was detected, CIs were wide, but the MD in favour of APM exceeded the threshold for clinical importance in pain, function and knee-specific quality of life at 24 months. No trial has compared APM with no intervention.
Prior reviews of knee arthroscopy included trials of interventions such as knee lavage or debridement for advanced osteoarthritis alongside trials of APM for meniscal tears.16 27–29 For example, the aim of the recent review by Thorlund et al 16 was to determine the ‘benefits and harms of arthroscopic knee surgery for middle aged or older patients with knee pain and degenerative knee disease’. Our systematic review is more specific, including only trials of APM performed for meniscal tears. Our analysis confirms, however, that outcomes after APM surgery are inferior in patients with osteoarthritis and that APM should not be considered a first-line treatment option, especially in those with non-specific ‘knee pain’.
In comparison with non-surgical interventions, the greatest improvement in pain and quality of life was seen in patients with knee pain and a meniscal tear but without osteoarthritis. In this group, APM was associated with improvement in pain and knee-specific quality of life in comparison with non-surgical treatment, at a level that, as discussed later, may exceed the MCID. Effect estimates were limited, however, by small study numbers, large numbers of patients ‘crossing-over’ to undergo APM after being randomised to comparator interventions, a lack of blinding in those studies without a surgical comparator and wide CIs. It should be noted, however, that the physiotherapy delivered by the included trials was intensive, generally including a progressive combination of muscle strength, endurance, flexibility and balance exercises with gym sessions 2–3 times per week for 3–12 weeks. The associated outcomes may not be generalisable to clinical practice and the cost-effectiveness of the intervention requires evaluation in comparison with, for example, a less costly unsupervised home exercise programme. Further studies are needed to determine the effectiveness of APM when applied to patients who fail to respond to non-surgical treatment.
No trial has been performed, or been registered, with inclusion criteria limited to patients meeting the clinical and radiological criteria required for APM to be recommended in current practice, that is, an unstable pattern of tear with symptoms that are considered to be likely to be ‘meniscal’ in origin rather than non-specific knee pain.23 63 Previous trials have not used or recorded these specific criteria in individual patients, and therefore no meaningful subgroup data were available for analysis.
It remains unknown whether APM performed in a population with more focused indications (unstable meniscal tear and without osteoarthritis) may be beneficial to pain and quality of life, especially in patients who fail to respond to non-surgical treatment.64 65 Our review only identified one cohort study, which provides low-quality evidence that APM may provide some benefit in pain relief in this population.58 The authors of the four most recent trials provided supplementary subgroup data for inclusion in our review (Gauffin et al, Kise et al, Roos et al and van de Graaf et al),42–45 which did show some improvement in mean outcomes when patients with osteoarthritis were excluded.
Up to 30% of patients randomised to non-surgical treatment ‘crossed over’ to undergo APM before final follow-up, which is a serious limitation of the current trial evidence.42 43 45 53–55 66 This issue was not limited to studies with a non-surgical comparator and also observed in up to 36% of comparator patients in studies with a surgical comparator and 21% with a pharmacological comparator.44 55 These patients were not blinded, and the outcome of these individuals had they not undergone APM is unknown, but the high cross-over rate confounds the non-surgical intention-to-treat analysis, particularly at longer term follow-up.67 For many years now, there have been calls for all patients with meniscal tears to be treated non-surgically in the first instance, with APM being reserved for those patients failing to improve with this treatment strategy.18 23 26 64 65 None of the included trials restricted inclusion to patients who had failed a specific non-surgical treatment programme, and future RCTs should aim to evaluate the effects of APM for this patient population.
Two RCTs have been performed of APM versus a surgical comparator (placebo or sham surgery) and interpretation of these studies requires careful consideration.44 62 In the larger, placebo-controlled study (Sihvonen et al),62 no difference was reported between the APM and placebo surgery (arthroscopic lavage) groups, while considerable improvement was noted from baseline to follow-up in both groups. As the trial lacked a non-surgical control arm, and patients had not undergone a period of structured physiotherapy before randomisation, it is not clear what underlies this improvement.65 In contrast, the other study of Roos et al 44 had a true sham surgery comparator, with patients receiving an anaesthetic but skin incisions only. Thirty-six per cent of patients in the sham group crossed over to undergo APM, yet the MD between groups in the intention-to-treat analysis was still suggestive of a better outcome in the APM group at over 12 months.44 CIs were wide in this small study, but the authors concluded that ‘a clinically relevant difference could not be excluded’.44 These conflicting results lead to uncertainty regarding the efficacy of APM and the ‘critical surgical element’ in the recruited patients.24 Meniscal tears may be asymptomatic and pain, and mechanical symptoms may be caused by other knee pathology.3 68 69 Therefore, it is essential that clinical and radiological features correspond before arthroscopy is recommended over alternative non-surgical treatments.23 In the majority of RCTs, patients were eligible for inclusion if they had knee pain localised to a joint line and any pattern of meniscal tear. In the one study (Sihvonen et al)70 where knee arthroscopy was performed in all patients, 27% had full thickness cartilage loss and 47% had partial thickness cartilage degeneration, despite minimal radiographic evidence of osteoarthritis prior to surgery. For these individuals, partial resection of the meniscus is unlikely to be the critical surgical element to induce a treatment effect in comparison to a placebo effect or any other effect, for example, from the joint lavage performed in both the intervention and control groups of this particular study.24
No trials have been performed with inclusion criteria limited to the current consensus led indications for APM: with appropriate meniscal symptoms corresponding with an unstable meniscal lesion visible on MRI as the treatment target.23 Although authors have attempted to report outcomes in underpowered subsamples of patients with either unstable meniscal tears or with mechanical symptoms, no attempt has, so far, been made to relate the symptoms with the pathology.71 As a result, the efficacy of APM in this group is unknown, despite a single cohort data supporting the usefulness of the treatment after failure of physiotherapy.58 No other systematic review has attempted to address this question and clearly more evidence is required to define the efficacy of APM in these patients.
Strengths and limitations
This review is the first to specifically focus on the effectiveness of APM in patients with meniscal tears, stratified according to the important clinical and radiological patient selection criteria.23 The analysis was bolstered by the provision of unpublished data by the authors of four trials. Only RCTs were included in the pooled analysis due to the risk of selection bias in cohort studies. The review search strategy was, however, highly sensitive and designed to also identify cohort studies and ongoing studies to provide context and narrative when no completed trial evidence was available. The current evidence does have a number of limitations including small numbers of trials and study numbers, risk of bias and high rates of cross-over of participants to APM from comparator interventions in both unblinded and blinded studies.
To ease interpretation, all outcomes were converted to familiar PROM instruments in the summary of findings tables. When considering the magnitude of the effect from APM reported, it must be noted that the MCID and patient acceptable symptom state (PASS) in PROM scores for patients with meniscal tears is unknown.37 59 Although generally not designed for use in patients with meniscal tears, attempts have been made to validate a number of PROMs for use in this population. The validation evidence is, however, poor quality and incomplete, with the lack of a known MCID a major limitation.37 Nevertheless, to ease interpretation of our study, an MCID threshold of 8–10 was used to attribute potential clinical relevance for outcomes measured on the 0–100 KOOS scale, as proposed by the developers of the tool.56 57 As Lysholm is measured on the same scale and has otherwise comparable measurement properties in similar patient groups, the same tentative threshold was applied to interpreting functional differences measured on the Lysholm scale.59 For generic quality of life, one estimate of an MCID of 0.15 on the EQ-5D has been suggested for patients with osteoarthritis.60 Even for osteoarthritis of the knee, however, MCID estimates vary widely from 4 to 20 for KOOS pain and 3–9 for KOOS function in daily living (KOOS-ADL)60 The thresholds for interpretation are therefore intended as a tentative guide only, as the true MCID and PASS for the population of patients with meniscal tears remains unknown.37 59 For reference, we have also included a summary of the magnitude of effect based on the SMD guide thresholds suggested by Cohen.39
Another important limitation to the interpretation of the current evidence is that the treatment preferences of patients with meniscal tears are currently unknown. In general, any benefit from APM in comparison with non-surgical treatment was seen in the early (under 6 months) and midterm (6–12 months) following intervention but not detected in the longer term (over 12 months). The relative patient preference for a potentially more rapid improvement in pain and quality of life following APM, in comparison with avoiding surgery but a slower rate of improvement with non-surgical treatment, has not been evaluated. Furthermore, only one trial has evaluated outcomes at greater than 2 years following APM in comparison with physiotherapy, and therefore the longer term outcomes of APM, including rates of progressive osteoarthritis, in comparison with alternative treatments remains relatively uncertain. The high rate of cross-over of non-surgically treated patients to APM may also influence treatment decisions.
Meaning of study
This review highlights the importance of stratifying the trial evidence to specific populations of patients with meniscal tears, by the key clinical and radiological findings. Performing APM in all patients with knee pain and a meniscal tear, without initial non-surgical treatment, is not appropriate, especially in patients with concurrent osteoarthritis where outcomes are inferior. However, in trials reporting the ‘cross-over’ of patients randomised to non-surgical treatment, up to 30% of patients subsequently chose to undergo APM due to a reported lack of improvement in their symptoms. Further research is required. but the findings broadly suggest that APM should be reserved for patients with persisting symptoms, correlating with a meniscal tear, after completion of intensive, appropriately structured non-surgical treatment (physiotherapy).
Unanswered questions and future research
Perhaps the most important conclusion of this review is that the current trial evidence should be interpreted with care due to limitations from non-specific selection of patients (without stratification) and the overall small numbers of included patients. The available evidence suggests that surgical treatment should not be the first-line intervention for patients with meniscal tears. Outcomes are improved in patients without osteoarthritis, but crucially, no trial has been limited to individuals failing to respond to non-surgical treatment, and patients meeting the strictest clinical and radiological indications for APM are not represented by the current evidence. There is an urgent need for a high-quality RCT in this population.
What is already known
Arthroscopic partial meniscectomy (APM) is one of the most commonly performed surgical procedures worldwide, and rates have risen, particularly in older age groups susceptible to degenerative knee disease.
Previous systematic reviews have demonstrated that undifferentiated knee arthroscopy (lavage, debridement and/or APM) performed for pain associated with degenerative knee disease is ineffective. The effectiveness of APM, specifically in patients stratified according to the important clinical and radiological patient selection factors, is unknown.
What are the new findings
This systematic review indicates that surgical treatment should not be the first-line treatment intervention for patients with a meniscal tear.
APM provides a small improvement in all people and small to moderate improvement in those without osteoarthritis, from reduction in pain and improvement in function and quality of life, compared with physiotherapy, but the clinical importance of these improvements is uncertain.
Patients meeting the latest, strict, clinical and radiological selection criteria for APM are not represented by the current evidence, and no study has been limited to patients who have failed non-surgical treatment. There is an urgent need for trial evidence in this group to inform clinical guidelines and practice.
Acknowledgments
The authors would like to thank Eli Harriss, Bodleian Health Care Libraries, University of Oxford, for work designing and running the search strategy for this review. The authors would also like to thank Nina Jullum Kise (Martina Hansens Hospital), Håkan Gauffin (Linkoping University), Ewa Roos (University of Southern Denmark) and Victor van de Graaf (OLVG Amsterdam), along with their coauthors, for kindly agreeing to provide unpublished study data.
References
Footnotes
Contributors SGFA: concept, methodology, study selection, analysis, writing and editing paper and guarantor. SH: concept, methodology, analysis, writing and editing paper. APM and LEB: study selection and editing paper. DJB: concept, writing and editing paper. AJP: concept, methodology, writing and editing paper.
Funding This report is independent research supported by the National Institute for Health Research (NIHR Doctoral Research Fellowship, SGFA, DRF-2017-10-030) and Oxford NIHR Biomedical Research Centre.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Dataset available from the corresponding author.
Patient consent for publication Not required.