Article Text

Abstract
Objective To determine whether a structured programme of parent anticipatory guidance ‘Toddlers Without Tears,’ delivered in universal primary care, can prevent preschool child behaviour problems.
Design Cluster randomised controlled trial.
Setting/participants 40 primary care nursing centres (clusters) in metropolitan Melbourne, Australia. 733 English-speaking mothers of 6- to 7-month-old infants consecutively recruited from well-child appointments; 589 (80%) retained at age 3 years.
Intervention Parenting programme from age 8 to 15 months, with two group sessions co-led by well-child providers and a parenting expert. The programme addressed normal behaviour development and offered strategies to increase desired and reduce unwanted behaviour. While 93% of intervention parents received at least some of the programme, only 49% completed all components.
Control Usual primary care.
Main outcome measures Maternal report of child externalising behaviour (Child Behaviour Checklist), parenting (Parent Behaviour Checklist) and maternal mental health (Depression Anxiety Stress Scales) when children were aged 3 years.
Results Behaviour scores in the intervention and control groups were similar (mean (SD)) 11.4 (7.1) versus 12.4 (7.6); adjusted mean difference −0.8, 95% CI −2.2 to 0.6, p=0.26). On the parenting subscale scores, intervention parents reported fewer unreasonable expectations of child development (37.3 (10.9) vs 39.9 (10.2), adjusted mean difference −3.1, 95% CI −4.9 to −1.4, p=0.001). The mean scores for harsh/abusive and nurturing parenting, and maternal mental health, were similar between the two groups.
Conclusions A brief universal parenting programme in primary care is insufficient to prevent development of preschool externalising problems. A new population trial targeting more intensive prevention to distressed parents with toddler behaviour problems is now under way, aiming to prevent externalising and internalising problems before school entry.
Trial registration number ISRCTN77531789
Statistics from Altmetric.com
Introduction
Mental health problems affect around one in five youth in Australia and internationally,1 with major personal, societal and economic ramifications.2 3 Children's mental health problems are primarily externalising (eg, oppositional defiance, aggression) and internalising (eg, anxiety, depression) problems.1 Up to 50% of preschool behaviour problems persist through childhood if left untreated, then into adolescence and adulthood.4 Approaches to improving children's mental health in the population would ideally involve effective prevention in addition to clinical treatment of severe problems.5 6 Behavioural parenting programmes have the strongest evidence of efficacy to date for treating children's established behaviour problems.2 7,–,10 Although effective, parenting programmes to treat children's established behaviour problems are cost- and time-intensive, and require an available workforce trained in evidence-based treatments. They are currently inaccessible to most families in Australia.1
What is already known about this topic
Mental health problems affect up to 20% of children and have cumulative personal, societal and economic ramifications.
A brief, universally offered parenting programme led to modest improvements in parenting risks but did not impact on toddler behaviour.
What this study adds
Rather than sleeper effects on preschool behaviour, the impacts of a brief universal parenting programme on parenting faded with time.
A further trial needs to test if a universal programme adds public health benefit when coupled with an effective targeted family support programme (by improving reach and uptake).
However, the potential of universal prevention in early childhood to improve mental health remains largely unexplored.2 5 7 We previously published short-term outcomes at toddler age11 of the first cluster randomised trial of a truly universal early parenting programme, Toddlers Without Tears, designed to be offered to all parents in the community and aiming to prevent externalising behaviours using anticipatory guidance before any developmental onset. Programme content was informed by a review of the intervention literature (social learning and attachment theoretical perspectives) and developed in partnership with parenting experts and well child providers to be delivered at age 8–15 months in the Australian primary care setting.12 The programme achieved high recruitment, fidelity and retention, and some modest short-term outcomes at each of 3 and 9 months postintervention.11 At age 18 months (3 months postintervention) child behaviour, parenting and maternal mental health scores were similar in the intervention and control groups. By age 24 months (9 months postintervention) parenting effects emerged, with intervention parents significantly less likely to report harsh/abusive parenting (adjusted mean difference −1.83, 95% CI −3.12 to −0.55, p=006) and unreasonable expectations of child development (−2.18, CI −3.74 to −0.62, p=005).11
We now report trial outcomes at preschool age (3 years), that is, 21 months postintervention. Longer-term follow-up is required to determine whether the above short-term benefits are extinguished, maintained or augmented over time. Preventive interventions might have ‘sleeper effects’13,–,16 whereby initial improvements are seen, but more sizeable improvements lie dormant, to be seen at a later developmental period. Sleeper effects are frequently discussed in prevention science literature. Gray and McCormick15 cite as examples reduced criminal/antisocial behaviour emerging long term in the Nurse Home Visiting Programme, High Scope/Perry Preschool Study and Chicago Child Parent Centre Programme. In the present study, from a developmental perspective young children's behaviour becomes more regulated overall from the toddler to preschool period.17 Families in the intervention group have time to practise and therefore could consolidate new parenting skills from the anticipatory guidance programme over time. Therefore, preventive effects could become more apparent with the longer follow-up. Alternatively, because of the brevity of this preventive intervention, one might expect impacts only to be evident in the short term. Of these possibilities (emerging vs fading effects) we hypothesised that the short-term benefits of brief universal prevention would be reduced by longer-term follow-up.
Methods
Setting and participants
Detailed description of the trial's methods have been previously published.11 The cluster randomised trial was conducted in six socio-economically diverse18 local government areas (LGAs) in Victoria, Australia.11 Free universal health visits are scheduled from birth to 42 months of age, and over 90% of parents attend visits during the first 6 months of life.19 Maternal and child health (MCH) nurses consecutively invited mothers of 6- to 7-month-old infants attending across August–September in 2004 to take part in the Toddlers Without Tears trial. The only exclusion criterion was mothers with insufficient English to complete questionnaires.
Cluster randomisation
The trial was conducted in accordance with the CONSORT statement for cluster randomised trials.20 MCH centres (clusters) were randomised to minimise contamination that might result if parents attending the same centre were randomised to different groups. Randomisation was conducted after recruitment of families, by an independent statistician using a computer-generated allocation sequence. Randomisation was performed within pairs created by matching centres according to the closeness of their socio-economic level18 within each LGA. Allocation was concealed from researchers and participants until recruitment was complete.
Universal anticipatory guidance
The structured parenting programme consisted of three sessions targeting key modifiable parenting risk factors for children's externalising behaviour problems, that is, harsh/abusive discipline, low nurturing and inappropriate expectations of child development. At the routine individual health visit at 8 months, mothers received four handouts (discussed in 15 min) on what to expect in terms of normal child behaviour over the ensuing 12 months (ie, high mobility and tantrums). At 12 months, parents were invited to attend a 2 h group session at the local MCH centre discussing ways to develop a warm and sensitive relationship with their toddler and encourage desirable behaviour. The need to plan ahead for ‘difficult’ situations where toddlers are likely to misbehave was introduced, along with alternatives to common parent ‘irrational beliefs’ that can lead to harsh parenting. At 15 months, parents were invited to another 2 h group session discussing ways to manage unwanted child behaviour. Rather than smacking and yelling, parents were encouraged to distinguish ‘low-priority’ problem behaviours (eg, tantrums) for which strategies such as planned ignoring, distraction and logical choices were discussed, and ‘high priority’ misbehaviours (eg, aggression) for which ‘quiet time’ was discussed.
Procedures were employed to maximise fidelity of prevention programme delivery. These included (1) standardised training for all intervention MCH nurses, (2) codelivery of the intervention by a nurse and an experienced child psychologist, (3) a scripted intervention manual for leaders to follow and (4) standardised handouts for parents. MCH nurses completed a checklist at the end of each parenting group recording which intervention components were delivered that demonstrated fidelity. The programme was offered locally in the community at MCH centres routinely attended for infant health advice. On-site child care was offered, along with a variety of alternative days and times for groups (including after hours). Ninety-three per cent of mothers in the intervention group attended the first individual visit, 67% attended the group session at child age 12 months, and 56% attended the group session at child age 15 months;11 thus 49% of intervention mothers completed all three intervention sessions.
Usual care
Families in the control arm of the trial received usual healthcare from their MCH nurse, which may include some advice on early behaviour but does not incorporate a structured prevention programme to promote young children's behavioural development.
Measures
Baseline and outcome data were measured by validated questionnaires completed by the primary care giver.5 11 The baseline questionnaires at age 7 months measured sociodemographic details, infant difficult temperament, maternal mental health and family stress and, at 12 months, parenting style and partner relationship. The short-term outcome questionnaires at 18 and 24 months are detailed later as per long-term outcomes. The outcome questionnaires repeated the 12 month measures of parenting style and parent mental health, and added measures of child externalising and internalising behaviour. High sample retention was achieved at 18 months (92%) and 24 months (89%).
Consistent with prior short-term outcomes, the primary measure at age 3 years was externalising behaviour problems, assessed by the 99-item validated Child Behaviour Checklist (CBCL 1½–5).21 This checklist also quantifies internalising behaviour problems, and yields raw scores (used to compare groups as the primary outcome) and T-scores with a clinical cut-point derived from the combined norming sample of children aged 1 through 5 years (used to describe the sample relative to international norms). The secondary outcome measure was the Parent Behaviour Checklist (PBC),10 a 32-item measure of parenting practices known to contribute to externalising behaviour problems (harsh/abusive discipline, nurturing, expectations of normal development) for parents of children aged 1–5 years. The PBC yields T-scores (mean 50, SD 10) derived from norms with 6 month age-bands (no clinical cut points). Maternal mental health was measured by the Depression Anxiety Stress Scales (DASS),22 a 21-item measure that, as well as mean scores for each subscale, provides cut points to indicate risk of depression (score >9), anxiety (score >7) and stress (score >14).
Analysis
Outcome variable means were compared between the intervention and control trial arms at follow-up. To detect a reduction of 0.3 SD units in the mean score for the primary outcome with 80% power at the two-sided significance level of 0.05, 175 children were required for each of the intervention and control groups. The sample size was inflated by a design effect of 1.18–210 infants per trial arm to allow for correlation between responses within the same MCH centre cluster,23 assuming an average cluster size of seven eligible mothers attending each centre and intracluster correlation coefficient of 0.03. Assuming a 30% drop out rate at follow-up, a final sample size of 300 infants per trial arm was required and achieved for adequate power at long-term follow-up.
The trial arms were analysed as randomised, applying the intention to treat principle. We compared the trial arms using unadjusted analyses and analyses that were adjusted for potential prognostic factors (listed in table 2). Analyses were implemented at the level of the individual using random effects (multilevel) linear regression models24 fitted using maximum-likelihood estimation to allow for the correlation (or clustering) between the responses of subjects from the same MCH unit. Effect sizes were calculated by dividing the mean difference between the trial arms by the pooled SD. Analyses of all skewed outcomes were validated using the bootstrap method.25 Analyses were carried out using Stata 9.2.26
Long-term outcome comparisons at child age 3 years
Project approval (26007A, 1/10/06) was obtained from the Ethics in Human Research Committee of the Royal Children's Hospital, Melbourne, Australia.
Results
Sample retention
Of the original 733 families recruited in infancy, 589 (80%) completed the 3-year-old follow-up (on average 29 months postrandomisation and 21 months postcompletion of intervention) (see figure 1). Table 1 describes characteristics of the original sample and those completing follow-up for each trial arm. At 3 years of age, 259 (79%) and 330 (82%) of intervention and control families, respectively, returned the questionnaires. Families who completed the follow-up questionnaires were similar to the baseline sample with respect to child gender and temperament, maternal education and mental health, and household income and disadvantage scores.

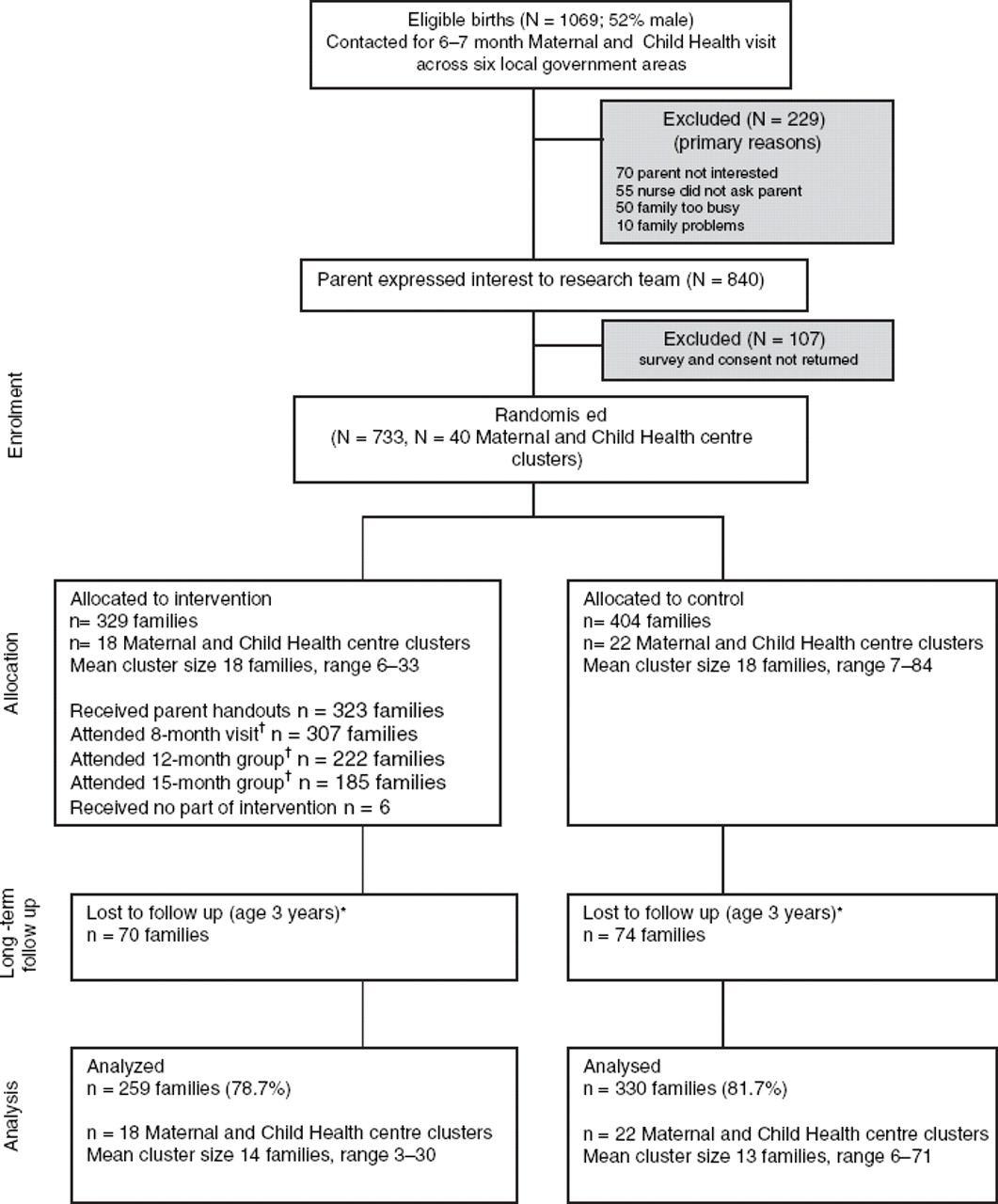{kind=link}
CONSORT flow chart of participants.
*All lost to follow-up due to failure to return questionnaires. †Take-up of the intervention was voluntary.
Sample characteristics
Outcomes at long-term follow-up
Child behaviour
United States population norms for children's externalising and internalising problems (1–5 years combined) have a T-score mean (SD) of 50 (10), with 17% of children scoring above the borderline-clinical cut point (60). The Australian 3-year-old sample had a slightly lower level of externalising problems, with a mean (SD) of 49 (10) and 12% of children scoring above the borderline-clinical cut point. The Australian sample's 3-year-old level of internalising problems was also slightly lower than United States norms, with a mean (SD) of 47 (10) and 12% scoring above the clinical cut point. At child age 3, the mean (raw) externalising behaviour score was similar between trial arms (mean (SD): 11.4 (7.1) vs 12.4 (7.6); adjusted mean difference −0.8; 95% CI −2.2 to 0.6; p=0.26). The mean child internalising scores were also similar between the universal prevention and control groups at age 3 years (table 2).
Parenting practices
Mean scores for harsh/abusive discipline and nurturing parenting were similar in universal prevention and control groups (table 2). Intervention mothers, however, continued to report lower levels of unreasonable developmental expectations with their preschool children than did control mothers (adjusted mean difference of −3.1 (95% CI −4.9 to −1.4; p=0.001), effect size of −0.29 (95% CI −0.47 to −0.13)).
Maternal mental health
The mean maternal stress, anxiety and depression scores did not differ between the two groups by child age 3 years (table 2). Two posthoc tests of interaction provided no evidence of differential effects of intervention on externalising or internalising behaviour problems by preintervention risk based on (1) a maternal mental health problem (clinical-level depression, anxiety or stress) or (2) infant difficult temperament.
Discussion
Rather than emerging positive sleeper effects on preschool child behaviour, the impact of a brief universal parenting programme on harsh discipline parenting practices faded over time from toddler to preschool age. Other than fewer unrealistic expectations of their preschool children's behaviour, intervention parents did not differ from controls on parenting, parent mental health or child behaviour outcomes. Although not statistically significant, all of the small observed differences did favour the prevention group. Nevertheless, given the brevity of the intervention, longer-term outcomes are likely to show further fading of effects over time. We are collecting school entry data for this sample in 2010 to confirm this prediction.
Methodological issues for prevention trials
This cluster randomised trial had several strengths including high population uptake (69%) based on eligible birth records, wide socio-economic representation, well-validated and age-appropriate outcome measures, and high retention (80%). This strongly supports the validity of the trial's findings.
The trial had three limitations. First, we included single source (maternal report) rather than multisource assessment. Primary care giver report is widely recognised to be the most useful source for very young children's behaviour,25 but mothers could not be blinded to their group membership. A lack of blinding, however, should increase the difference between intervention and control groups, leading to false positive rather than null results. A second limitation was that the highest-risk families in the population and non-English-speaking parents were likely under-represented in this universal prevention trial. Nevertheless, many families with known and measured risks for behaviour problems were recruited, with 39% of the sample at baseline reporting the risk factors of maternal depression, anxiety, substance misuse, partner conflict, social isolation and/or financial problems.5
Third, while almost all families (93%) received some components, only half (49%) received the entire programme. This ‘dose’ of uptake is high for an unsolicited universal prevention programme that required parent time and travel. We maximised attendance by programme brevity, delivery nearby in routine health services, out-of-hours sessions and free on-site child care, and parents who missed group sessions were still mailed the written parenting handouts. Eighty-nine per cent of all intervention mothers reported they would recommend this programme to their friends. In any universal programme, it is likely that many parents will not feel the need to attend all sessions, particularly if they are busy and not experiencing behaviour difficulty. The intention-to-treat analyses in our trial therefore determined whether universal prevention effects occurred at a population-level, based on ‘real world’ uptake.
Conclusions and future direction
These long-term outcomes do not support widespread promotion of a brief universal parenting programme during the toddler years as a stand-alone approach for preventing preschool mental health problems. While it remains possible that a higher ‘dose’ of the programme (ie, more sessions over a longer period) might be effective, this would be more costly and probably too burdensome for parents, based on our falling attendance by the third session.
There is now good evidence that a targeted programme addressing the issues most strongly related to early externalising and internalising symptoms (maternal stress and negative parenting practices)27 can effectively reduce preschool behaviour problems.28 However, this means that only those parents identified with overt stress or parenting issues receive the programme, when many others may also be covertly in need. Therefore, it remains possible that a universal early parenting programme coupled with an effective targeted family support programme for toddlers still at risk at age 2–3 years could substantially add to the population benefit of the targeted programme alone, by increasing community reach and uptake of the targeted intervention when needed. It is our view that a trial of this approach is now warranted, with a focus on costs and on coverage, uptake and costs as discriminators for the public health benefit.
Acknowledgments
The authors acknowledge the input of A Price and E Morton-Allen as research assistants during data collection from 7 to 36 months. The authors would like to thank the MCH nurses and families of the Victorian Cities of Glen Eira, Greater Geelong, Kingston, Maribyrnong, Nillumbik and Stonnington who took part in this research.
References
Footnotes
-
Funding This project was funded by the Telstra Community Development Fund. JB is funded by an Australian Rotary Health Research Fund postdoctoral fellowship; HH's and OU's postdoctoral positions are funded by Australian National Health & Medical Research Council (NHMRC) Population Health Capacity Building Grant 436914; MW was part-funded by NHMRC Career Development Awards 284556 and 546405.
-
Competing interests None.
-
Ethics and approval Project approval (26007A, 1/10/06) was obtained from the Ethics in Human Research Committee of the Royal Children's Hospital, Melbourne, Australia.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent Obtained.