Article Text

Abstract
Objective Adverse events (AEs) associated with short-term corticosteroid use for respiratory conditions in young children.
Design Systematic review of primary studies.
Data sources Medline, Cochrane CENTRAL, Embase and regulatory agencies were searched September 2014; search was updated in 2017.
Eligibility criteria Children <6 years with acute respiratory condition, given inhaled (high-dose) or systemic corticosteroids up to 14 days.
Data extraction and synthesis One reviewer extracted with another reviewer verifying data. Study selection and methodological quality (McHarm scale) involved duplicate independent reviews. We extracted AEs reported by study authors and used a categorisation model by organ systems. Meta-analyses used Peto ORs (pORs) and DerSimonian Laird inverse variance method utilising Mantel-Haenszel Q statistic, with 95% CI. Subgroup analyses were conducted for respiratory condition and dose.
Results Eighty-five studies (11 505 children) were included; 68 were randomised trials. Methodological quality was poor overall due to lack of assessment and inadequate reporting of AEs. Meta-analysis (six studies; n=1373) found fewer cases of vomiting comparing oral dexamethasone with prednisone (pOR 0.29, 95% CI 0.17 to 0.48; I2=0%). The mean difference in change-from-baseline height after one year between inhaled corticosteroid and placebo was 0.10 cm (two studies, n=268; 95% CI −0.47 to 0.67). Results from five studies with heterogeneous interventions, comparators and measurements were not pooled; one study found a smaller mean change in height z-score with recurrent high-dose inhaled fluticasone over one year. No significant differences were found comparing systemic or inhaled corticosteroid with placebo, or between corticosteroids, for other AEs; CIs around estimates were often wide, due to small samples and few events.
Conclusions Evidence suggests that short-term high-dose inhaled or systemic corticosteroids use is not associated with an increase in AEs across organ systems. Uncertainties remain, particularly for recurrent use and growth outcomes, due to low study quality, poor reporting and imprecision.
- corticosteroids
- asthma
- bronchiolitis
- croup
- paediatrics
- safety
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Examined safety outcomes associated with short-term corticosteroid use across multiple common acute respiratory conditions in young children.
Broad range of adverse events (AEs) captured across organ systems.
Inconsistent definitions, assessments and reporting of AEs.
Extensive variation in corticosteroid formulations and dosages within and between studies.
Did not examine long-term corticosteroid use (>14 days).
Introduction
Corticosteroids are the cornerstone of treatment for many common paediatric respiratory conditions including croup and asthma.1–3 These conditions often result in presentation to urgent and emergency care settings, in otherwise healthy children. Previous studies examining corticosteroid use in chronic asthma have demonstrated the potential for short-term and long-term adverse events (AEs), particularly growth inhibition, bone disease and adrenal suppression.4–6 While corticosteroids have demonstrated effectiveness for the acute treatment of many respiratory indications, clinicians are faced with considerable uncertainty regarding short-term safety, particularly among the youngest children.1
Previous systematic reviews have examined corticosteroids in preschool or school-aged asthma or wheezing4 7 8; however, most focused on efficacy and were restricted to randomised controlled trials (RCTs). These reviews also focused on a specific underlying condition, disease severity, or particular corticosteroid, and mostly for longer-term administration (eg, for recurrent, persistent or chronic asthma). Current guidance on systematic assessment of harms highlights the need to include data from observational studies when considering safety outcomes.9 As well, it has been suggested that it may be useful to have a wider view of the evidence across a number of similar indications.10 Recent knowledge synthesis approaches have studied specific safety outcomes across conditions to increase power, with the assumption that some safety outcomes are not confounded by condition.10 Such a comprehensive approach to knowledge synthesis in this area is critical to inform treatment decisions, reduce practice variation and optimise management of young children who seek care due to acute respiratory illness.
The goal of this study was to synthesise evidence regarding the safety of short course corticosteroid use in young children (<6 years) with acute respiratory conditions.
Methods
This review followed internationally recommended methods and standards for systematic reviews.11–13 An a priori protocol was developed (available from authors).
Patient and public involvement
Patients and/or the public were not involved in the design or conduct of this systematic review.
Literature search
Original database searches were conducted September 2014 in Ovid Medline, the Cochrane Central Register of Controlled Trials (CENTRAL) via Wiley Cochrane Library, and Ovid Embase. Additional sources included regulatory agency databases: Drugs@FDA, Health Canada’s Drug Products Database and the European Medicines Agency’s European Public Assessment Reports. Search strategies combined index terms and keywords for respiratory illnesses, children and drug classes identified in the Global Initiative for Asthma (GINA)14 guidelines. Study design filters were applied to limit results to RCTs and observational studies. Update searches were executed in Medline and CENTRAL in February 2016, and then again in July 2017. Detailed search strategies are in online supplementary file 1.
Supplemental material
Eligibility criteria
We included primary studies involving population (P): children up to six years old; intervention (I): treated with single or recurrent systemic (any dose) or high-dose inhaled (as defined by the GINA guidelines14) corticosteroids for up to 14 days; comparator (C): any comparator; outcome (O): any AE; timing (T): any timing; and, setting (S): any inpatient or outpatient setting providing care to children with an acute respiratory condition. See online supplementary file 2 for detailed eligibility criteria.
Supplemental material
Given the lack of standardised terminology for safety, we gathered information on all potentially drug-related harm outcomes15 from studies including, but not limited to: adverse drug reactions, adverse drug events, medication errors, side effects and potential adverse drug events. For consistency, these outcomes are referred to in the manuscript as AEs. Studies that did not report or mention AEs were excluded. Due to resource constraints and mean age of the studies, no attempt was made to contact study authors if no harms were reported in the text, or when there was potentially missing data; such efforts are unlikely to yield additional data.
Study selection
Two reviewers independently screened the titles and abstracts of all records using a priori selection criteria. Full texts of potentially eligible studies were reviewed by two reviewers independently using a standard form. Disagreements were resolved through consensus or consultation with a third reviewer.
Data extraction
One reviewer extracted data using a structured form, with verification by a second reviewer. Data were extracted on study characteristics (design features), patient characteristics (age, sex, baseline characteristics), respiratory conditions, interventions (type, dose, duration, route of administration, timing, cointerventions, rescue medications), outcomes (types and timing), care setting, funding sources and results.
AEs were extracted as reported by study authors and categorised using a published model based on organ systems (see Results section).16 A panel of clinicians with specialties in paediatrics, emergency medicine, respiratory medicine and clinical pharmacology rated each AE in order of clinical severity independent of knowledge of the study results.
Assessment of methodological quality
Two reviewers independently assessed the methodological quality of studies using the McMaster Quality Assessment Scale for Harms (McHarm)17; disagreements were resolved through discussion.
Data synthesis
A comparative summary of AEs for studies with more than one treatment arm was presented to provide an overall picture of which interventions had a high risk of specific AEs. Risk differences were pooled using the DerSimonian Laird inverse variance random-effects method utilising the Mantel-Haenszel Q statistic. Binary data were also pooled using the Peto ORs (pORs) fixed-effects method.18 Studies that reported at least one event in at least one treatment arm were included in the analysis of pORs and all comparative studies were used for analysis of RD. One AE (growth) was reported as a continuous outcome and data were pooled using a DerSimonian Laird inverse variance random effects method as a mean difference (MD; in cm). The I2 statistic was presented to quantify the magnitude of statistical heterogeneity between studies; while the I2 has the potential to be misinterpreted, it is the standard in the field and we chose to present the statistic for informational purposes.19 Subgroup analyses from study-level data were conducted for respiratory condition and dose (single vs multidose) using Cochran’s Q (α=0.05) to detect statistical heterogeneity. Studies contributing no numerical data for analysis (eg, single arm studies, studies that reported no AEs overall) are summarised in online supplementary file 3. Assessment of small-study bias (for meta-analyses with at least eight studies) was planned using the funnel plot and Egger’s test20; however, this was not conducted due to inadequate number of studies for each outcome. Analyses were conducted using Review Manager V.5.3 (Cochrane Collaboration).21 Graphs were constructed using TIBCO Spotfire S+Workbench V.3.4.22
Supplemental material
Results
Database and grey literature searches yielded 9134 records. Eighty-six papers (85 studies)23–108 involving 11 505 participants were included (figure 1). Characteristics of the included studies are in online supplementary file 3. There was large variation in corticosteroid type, dose, duration and route of administration, both for systemic and inhaled corticosteroids. Methodological quality of studies was poor overall due to inadequate reporting of how AEs were defined and collected (table 1; online supplementary file 4).
Supplemental material

PRISMA study flow selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary of methodological quality assessments
Adverse events
Results below are presented according to the categories in table 2. Figures 2, 3 and 4 display forest plots of AEs comparing systemic corticosteroid to placebo, inhaled corticosteroid to placebo, and systemic dexamethasone to another systemic corticosteroid, respectively. Results of meta-analyses and subgroup analyses are in online supplementary file 5, with effect estimates and 95% CIs. Forest plots from meta-analyses are in online supplementary file 6. There was large variation in the number of studies and number of patients with available data for meta-analysis across comparisons and outcomes. Further, for four safety outcomes there were no events in both study arms (double-zero) across studies. In most cases, the subgroup analyses by dose and condition did not differ substantially from the overall results. Studies reporting no AEs overall are summarised in online supplementary file 7.
Supplemental material
Supplemental material
Supplemental material

Forest plot of adverse events—systemic versus placebo.

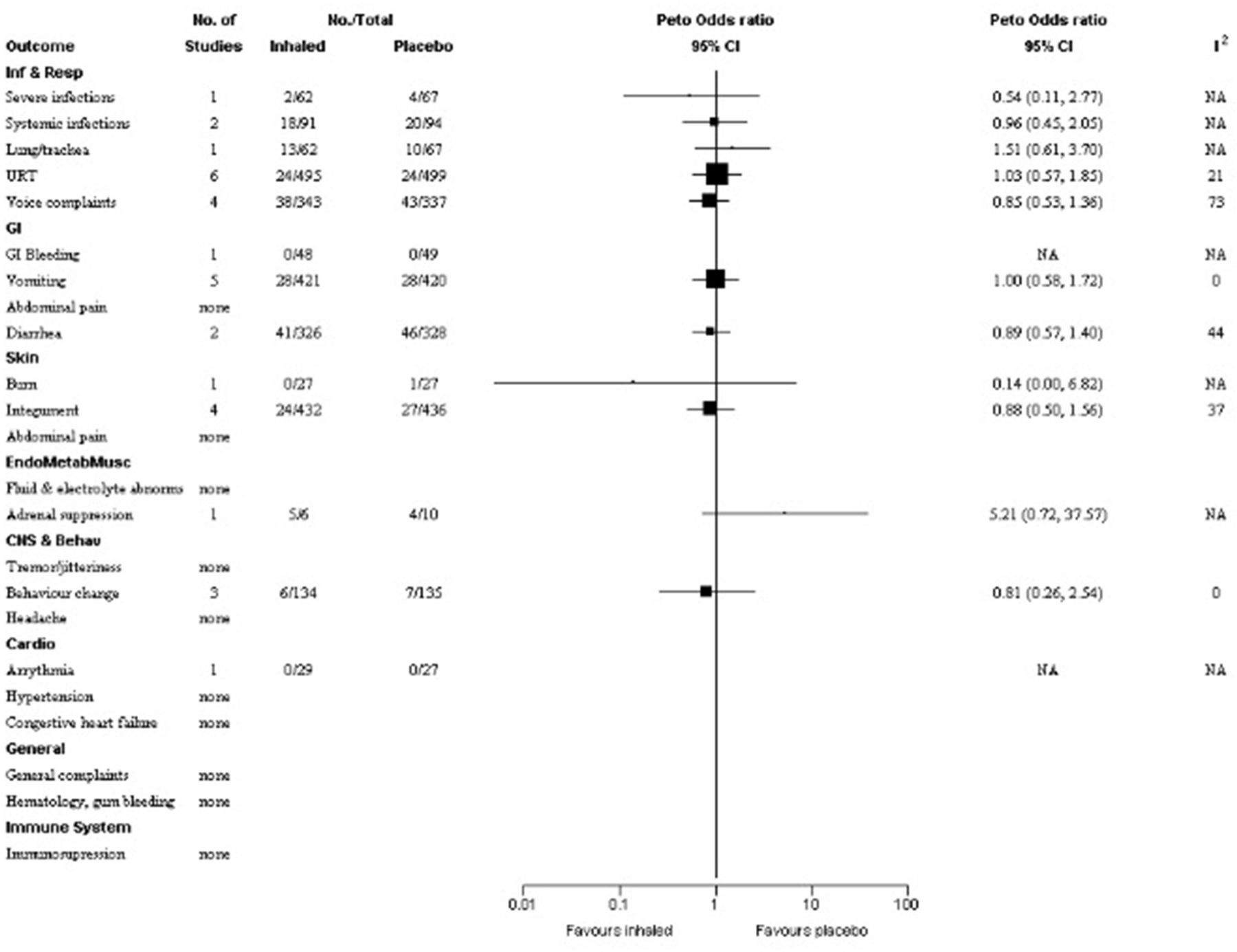
Forest plot of adverse events—inhaled versus placebo.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of adverse events—dexamethasone versus other.
Number of studies and participants reporting adverse events*
Infections and respiratory system
The number of studies contributing to each meta-analysis ranged from one to seven (range 58–2178 children). There were no statistically significant differences between: (1) systemic corticosteroid compared with placebo for severe infections,30 74 96 99 systemic infections,30 40 43 83 infections of the lung/trachea30 40 54 74 96 98 105 and the upper respiratory tract,30 43 54 65 67 74 and voice complaints43 (estimated pORs between 0.15 and 1.26) and (2) inhaled corticosteroid compared with placebo for severe infections,45 systemic infections,43 45 lung/trachea,45 infections of the upper respiratory tract37 44 45 65–67 or voice complaints37 43 100 101 (estimated pORs between 0.54 and 1.51). No study comparing dexamethasone with another corticosteroid reported infections or respiratory AEs.
Gastrointestinal tract
The number of studies contributing to each meta-analysis ranged from one to seven (range 97–3176 children). There were no statistically significant differences between: (1) systemic corticosteroid and placebo for gastrointestinal (GI) bleeding,30 32 40 65 83 87 105 vomiting,30 38 40 42 70 81 83 abdominal pain30 or diarrhoea42 77 105 and (2) inhaled corticosteroid and placebo for GI bleeding,65 vomiting37 45 69 85 101 or diarrhoea.37 45 Estimated pORs for both comparisons ranged from 0.89 to 1.10.
Meta-analysis of six studies (1373 children)25 27 41 49 52 80 found fewer cases of vomiting in patients who received dexamethasone compared with another corticosteroid, although the number of events was small (12/663 vs 51/710 cases; pOR 0.29, 95% CI 0.17 to 0.48; I2=0%). These studies focused on asthma (n=3),27 41 80 croup (n=2)49 52 or both (n=1)25; all compared oral dexamethasone with oral prednisone. No statistically significant difference was found for abdominal pain between dexamethasone and another corticosteroid.25 27 52
CNS and behaviour effects
The number of studies for each meta-analysis ranged from one to five (range 70–1159 children). The estimated pORs for the systemic corticosteroid and placebo were 1.44 for tremor/jitteriness,38 55 70 77 83 1.95 for behaviour change30 42 67 77 and 0.11 for headache,38 with no statistically significant differences. There were also no differences between inhaled corticosteroid and placebo for behaviour change67 85 101; and dexamethasone and another corticosteroid for behaviour change,52 57 headache27 52 or tremor/jitteriness,52 the latter with an estimated pOR of 6.63 from a small study (n=87) with only one reported event.
Dermatologic conditions
The number of studies per meta-analysis ranged from one to four (range 32–1079 children). There were no statistically significant differences between: (1) systemic corticosteroid and placebo for rash and hives,30 42 67 albeit with an estimated pOR of 7.59 (4/536 vs 0/543; 95% CI 1.07 to 54.01) and (2) inhaled corticosteroid and placebo for rash,37 45 85 hives67 and burning sensation68 (estimated pORs 0.88 and 0.14, respectively). No events of phlebitis were reported comparing dexamethasone to another corticosteroid. 57
Endocrine/metabolic and musculoskeletal systems
There were no statistically significant differences for electrolyte abnormalities between systemic corticosteroid and placebo (estimated pOR 3.08)30 47 83 102 and dexamethasone to another corticosteroid (estimated pOR 0.18).102
Pooled data for linear growth between inhaled corticosteroid and placebo included two studies (n=263) using recurrent doses for acute wheeze with follow-up at one year.28 45 The estimated change-from-baseline height was small (MD 0.10 cm; 95% CI −0.47 to 0.67; I2=9%). Five studies reported measurements of growth (height and weight) ranging from one to three years of follow-up, which could not be pooled due to heterogeneous interventions, comparators or outcome measurements.29 31 45 58 71 Three studies included data on inhaled corticosteroid versus placebo. One RCT on asthma58 (n=20) comparing budesonide and placebo found no signs of growth retardation by height measurements at 12 months or after up to six treatments. An RCT of episodic wheeze29 (n=294) found height at three years of age was unaffected in children receiving budesonide or placebo. One RCT of inhaled fluticasone propionate at very high doses (1500 μg per day during upper respiratory infections) versus placebo in recurrent wheeze45 reported additional outcome data on height that was not pooled in the meta-analysis mentioned above. There was a smaller mean change in height z score in the corticosteroid group over one year (MD −0.24; 95% CI −0.40 to −0.08; adjusted results).45 Furthermore, mean weight was significantly lower at one-year follow-up in the fluticasone group (n=62) versus placebo (n=67); two children given fluticasone and one given placebo met criteria for ‘failure to thrive’.45 Finally, two small trials did not report group differences for other comparisons: total and mean height growth (at 8–19 months) for intravenous dexamethasone versus inhaled budesonide in asthma (n=18)71; weight and height gains at 2 years for theophylline and metaproterenol with or without systemic prednisone on prevention of wheeze during upper respiratory infections in asthma (n=32).31
Five studies reported on adrenal function/suppression, with few children contributing data for this outcome.45 57 58 71 89 The RCT of high-dose inhaled fluticasone propionate versus placebo (99 children with data)45 found no significant differences between groups in basal cortisol (baseline and 12 months). Another RCT in asthma reported no differences in serum cortisol and urinary cortisol/creatinine after 10 days of inhaled budesonide or placebo (16 children with data). A subgroup who received oral betamethasone (n=9) showed significant changes from baseline after three days, but no differences at 12–14 days.58 Two studies included comparisons between different corticosteroids. One RCT89 in acute asthma compared intravenous prednisolone (n=20) with nebulised budesonide (n=30) and found significant levels of suppressed serum cortisol in the prednisolone group, although not considered pathologic by the study authors. Although another RCT57 comparing intramuscular dexamethasone with oral prednisone for asthma (n=32) found lower median urinary cortisol/creatinine in the former group at day 14, there was no statistically significant difference. An RCT71 comparing intravenous dexamethasone (n=9) with inhaled budesonide (n=9) found no significant differences between groups from baseline for blood pressure and blood glucose measurements.
Five studies reported on bone health biomarkers, three of which compared inhaled corticosteroids and placebo; no pooled analyses were performed.29 45 58 61 92 One RCT29 compared inhaled budesonide (n=294) with placebo in episodic wheeze and found no effect on bone mineral density over three years. The RCT comparing high-dose inhaled fluticasone propionate with placebo (n=59 children with data) in viral wheeze45 reported no statistically significant differences between groups in lumbar bone mineral density, bone mineral content or bone age at 12 months. A small RCT58 comparing inhaled budesonide with placebo (n=20) in asthma found transient decreased levels of bone and collagen markers post-treatment and in a subset of children who received oral betamethasone, with no difference between groups. A study of patients with acute respiratory illness92 compared hydrocortisone (n=28), methylprednisone (n=21) and controls (n=51) and found decreased levels of osteocalcin and alkaline phosphatase in younger children 2 days post-treatment; these effects were reversed 12 days after treatment. A non-randomised controlled trial of 36 asthma patients61 compared intravenous methylprednisolone of three different durations and found that all had decreasing levels of serum osteocalcin that correlated with increasing duration of treatment.
Cardiovascular system
No significant differences were found between systemic corticosteroid and placebo in three bronchiolitis studies reporting hypertension (estimated pOR 1).32 40 83 Single studies with up to 110 children did not report events for arrhythmia43 and congestive heart failure47 (systemic or inhaled corticosteroid vs placebo); and arrhythmia27 or hypertension57 (dexamethasone with another corticosteroid).
General AEs/other symptoms
Meta-analyses included a total of two studies (range 197–869 children). There were no statistically significant differences between: (1) systemic corticosteroid and placebo for pallor70 83 and (2) dexamethasone and another corticosteroid for dizziness52 or excessive urination.27 No study comparing inhaled corticosteroid with placebo reported general AEs.
Immune system and oncology
One study (95 participants)39 compared systemic corticosteroid and placebo and found no occurrences of immunosuppression. No other study reported immune system-related AEs.
Discussion
This systematic review of studies in which short-course corticosteroids were administered to children under six years of age for acute respiratory conditions, included 85 studies involving more than11 000 patients. These studies used a variety of delivery routes, doses, formulations and duration of corticosteroids. Overall, the evidence suggests that short-term corticosteroid use is not associated with a significant increase in AEs across organ systems. However, given the low quality of included studies, the heterogeneous and poor reporting of AEs, and the lack of precision of results, considerable uncertainties remain regarding the safety of high-dose inhaled or systemic corticosteroids for these indications in this age range.
A common concern when using corticosteroids in young children is effect on growth. Results from a single, small trial (n=129) of recurrent high-dose inhaled fluticasone propionate in wheezing preschoolers were heterogeneous across outcome measures, but suggested a small significant risk of growth suppression.45 Observational data have also suggested that multiple corticosteroid bursts can increase the risk of growth suppression, fractures, bone mineral accretion and osteopenia in children with underlying respiratory disease.5 6 109 Conversely, a pooled analysis using change-from-baseline linear growth did not find significant differences, although the other included study used a substantially lower equivalent dose of inhaled corticosteroid.110 Further, results from individual studies reporting transient differences in bone and adrenal biomarkers are of unclear clinical relevance, particularly for previously healthy children and single use. This calls for caution and monitoring of linear growth, particularly when use of high-dose inhaled or systemic corticosteroid is recurrent.
We found no other statistically significant differences between systemic or inhaled corticosteroid and placebo, or between dexamethasone and other systemic corticosteroid, including subgroup analyses by respiratory condition or dose, for AEs across organ systems. Due to small sample sizes and low number of events, these results should be interpreted with caution. While we found increased pORs when comparing systemic corticosteroids for behavioural outcomes such as tremor/jitteriness and behaviour change, there were wide CIs around estimates. No study examined neurodevelopmental outcomes after corticosteroid administration; ideally, studies should assess children for potentially related long-term AEs using validated instruments in this domain. Results from case series and case reports added anecdotal evidence of rare cases of hypersensitivity, infection or behavioural AEs, which have been described.111 112 While the estimated increased pOR for rash and hives was close to statistical significance, no other differences were found in systemic or severe infections as well as immunosuppression.
This review did not ascertain a clear safety advantage between systemic or inhaled corticosteroids compared with placebo. When comparing between different systemic corticosteroids, evidence favoured oral dexamethasone over oral prednisone for vomiting (pOR 0.029; 95% CI 0.17 to 0.48; I2=0%). Differences in palatability and tolerability between corticosteroids are well known to parents, healthcare providers and researchers, and can influence adherence to medication in children.113 Further, different specific formulations of corticosteroid (eg, prednisolone tablets vs prednisolone syrup) have been shown to influence taste and vomiting.25 However, cost and access to better tolerated formulations may be problematic. Subgroup analyses also found no significant differences between groups by respiratory condition or dose (single vs multiple) for these outcomes. Due to extensive variation in dosing within and across studies, we were unable to analyse data or draw further conclusions with respect to dosage or differences between specific molecules. It should be noted that among the eight RCTs35 43 46 51 65 67 71 89 directly comparing systemic and inhaled routes of corticosteroid administration, none contributed meaningful data for meta-analysis. The decision to initiate corticosteroid and the selection of drug, dose and mode of administration must consider these uncertainties on harms, as well as existing evidence on comparative potency and clinical effectiveness. The risk–benefit rationale is less established for repeated acute use in younger children, such as in recurrent wheezing.114
Strengths and limitations
We conducted a comprehensive systematic review of the literature following rigorous methods, including grey literature, to minimise potential for publication and selection bias. We examined safety outcomes across multiple acute respiratory conditions using ‘baskets’ of outcomes in each organ system to increase our ability to detect rare events and the precision of our estimates.16 This approach is reflective of clinical practice where corticosteroids are used across many respiratory diseases, even if the evidence base is not entirely robust for children. A recent systematic review also assessed the toxicity of short-course oral corticosteroids in children across clinical conditions.115 However, there was scarce overlap in respiratory conditions across included studies, and authors mostly provided estimates of the incidence of AEs within treatment groups rather than comparative treatment effects. Studies in adults have also adopted similar approaches to estimate incidence rates of AEs. For example, findings from a recent retrospective cohort in adults showed a significant increase in rates of sepsis, venous thromboembolism and fracture.116
This review was limited by the quality of the primary literature, particularly regarding the definition, assessment and reporting of AEs. This underscores the challenges researchers encounter when attempting to synthesise safety data due to sparse and poor reporting,117 and highlights the urgent need to enhance detection and reporting of AEs. For example, it is worthwhile noting that 26 studies reported ‘no AEs’ or ‘no significant AE’ which could not be included in pooled estimates; this may be a reflection of these studies being under-powered to detect statistically significant findings (especially for rare AEs) and/or AEs that may or may not be considered of special interest and/or clinically important. Such blanket statements are problematic for interpretation, highlighting the need for study authors to clearly report AEs of interest pre-study and post-study conduct. Common nomenclature (eg, www.meddra.org) and standardised approaches to collection of AE data should be implemented to help draw comparisons across studies. Further, safety reporting was not a primary focus of the studies, AEs were rarely defined a priori, and methods for ascertaining AEs were usually absent. While the McHarm scale is recommended to be used in conjunction with other quality assessment tools to evaluate the broader elements of study quality, we used it exclusively to assess methodological quality since the primary focus of this review was on AEs. The AEs reported typically reflect what is detected by a healthcare provider; it is difficult to discern what is reported by patients as well as what patients consider important. The duration of surveillance of most studies was insufficient to detect many of the long-term AEs potentially associated with corticosteroid use. Although the present study suggests that single doses of systemic or inhaled corticosteroids may result in few AEs, recurrent courses may lead to long-term risks, as cumulative dosing has been shown to be a determinant of safety.109 Finally, there was variation within and across studies with respect to maintenance corticosteroids, and concomitant and rescue medications. Due to the variation in corticosteroids and extensive range of AEs reported (including when a single study contributes to an outcome or in cases of zero events, where meta-analysis was not feasible or meaningful) among varied study designs of overall poor quality, we did not attempt to rate the quality of the body of the evidence using the Grading of Recommendations Assessment, Development and Evaluation118 approach.
Conclusion
This is the most comprehensive systematic review to date examining the safety of corticosteroids for managing acute respiratory conditions among young children, an age group of great clinical concern. While the existing evidence suggests that short-term high-dose inhaled or systemic corticosteroids is not associated with an increase in AEs across organ systems, uncertainties remain due to low quality of studies, poor reporting and lack of precision of results. Importantly, these results can help guide future research in the collection and reporting of AEs, particularly concerning measures of growth and behavioural outcomes; this in turn is needed to help inform shared decision-making between clinicians and parents/caregivers of young children.
Acknowledgments
We gratefully acknowledge the following individuals for their contributions: Megan Nuspl, Sanjaya Dhakal and Pritam Chordiya for assisting with screening, initial data extraction and verification, and article retrieval; Marc Parsons for assisting with data extraction and verification, and quality assessment; and, Jack Yeung, Marta Oleszczuk and Igor Pravdivyi for assistance with translations. MN, SD, PC and MP received remuneration for their work from a Canadian Institutes of Health Research (CIHR) grant (funding reference number KRS134306). JY, MO and IP did not receive remuneration for the translation work.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
Footnotes
Contributors RMF, AW, BV, SA, ACP, ASS, BHR, DWJ, DA, TPK and LH critically reviewed and contributed to drafts of the report. RF conducted the literature searches. AW conducted screening, quality assessments and data extraction. AW and BV conducted data synthesis/analysis. RMF, AW, BV, SA, ACP, ASS, BHR, DWJ, DA, TPK and LH contributed to interpretation of results. All of the authors approved the final version of this report.
Funding This study was funded by a Knowledge Synthesis Grant from CIHR (funding reference number KRS134306). The funder had no role in the design of the study, the collection, analysis or interpretation of data, the writing of the report or the decision to submit the paper for publication.
Competing interests All authors declare funding from CIHR for the submitted work. LH was funded in part by a New Investigator Salary Award from the CIHR. ACP is supported by a Tier II University of Ottawa Research Chair Award. BHR was supported by a Tier I Canada Research Chair in Evidence-based Emergency Medicine from CIHR. The remaining authors have no financial relationships relevant to this manuscript to disclose. DWJ, TPK and ACP are also authors on some of the included studies.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement LH had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Data for this systematic review (using published data) are available from the corresponding author upon reasonable request.
Patient consent for publication Not required.