Article Text

Abstract
Introduction A national research priority for people living with bile acid diarrhoea (BAD) is effective treatment options to improve their quality of life. This study aims to evaluate the feasibility of conducting a randomised controlled trial (RCT) of a novel healthy dietary pattern (The 8×5 Diet) to inform a future, larger trial.
Methods and analysis We plan to enrol 76 UK adults living with BAD and ongoing diarrhoea using self-selection sampling and digital technologies. Eligible participants will be assigned to groups using permuted block randomisation using 1:1 allocation to receive either 8 weeks of usual care or The 8×5 Diet using one-to-one, dietitian counselling via a video-conferencing platform and developed digital resources. Randomisation, consent, recruitment, retention and acceptability will be evaluated using data from the RCT and post-trial interviews conducted with those in the intervention group. Secondary outcome exploratory assessment will include health-related quality of life, symptom relief, diarrhoea, diet quality, nutrient intakes and diet satisfaction.
Ethics and dissemination Ethical approval was granted by the University of Manchester Research Ethics Committee (2024-19094-33261; V1.7, last updated: 24/02/2025).
Findings will be disseminated through peer-reviewed publication, conference presentation and social media.
Trial registration number NCT06259396.
- Clinical Protocols
- Adult gastroenterology
- NUTRITION & DIETETICS
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
The main strength of the study is the use of explicit feasibility criteria as the primary outcome.
The use of telemedicine to conduct the trial is appropriate for this patient population who have reduced health-related quality of life due to debilitating diarrhoeal symptoms.
Recruitment is limited to self-selected sampling across the UK, likely to be biased to those already highly motivated to change their diet in order to improve symptoms.
A mixed-methods approach will be employed to generate an integrated set of evidence, enhancing the results from a patient perspective to inform the design of a larger trial.
All assessments rely on accurate self-report using questionnaires and bespoke diaries. To reduce response bias related to food intake, all participants will maintain a dietitian-instructed, 7-day weighed food record at both baseline and during the last week of the trial.
Introduction
Primary bile acid diarrhoea (BAD) is a functional bowel disorder characterised by non-bloody diarrhoea.1 Untreated, the severity of the diarrhoea has been found to be worse than in irritable bowel syndrome (IBS), including urgency to defaecate, more watery stool consistency, bowel movements per week, importance to be near a toilet and worry about losing bowel control, significantly impacting on health-related quality of life (HR-QoL).2 BAD affects at least 1% of the population in the UK,3 compared with 4.0% for IBS.4 To differentiate BAD from IBS, the British Society of Gastroenterology recommends endoscopic investigation and objective testing using a radionuclide bile acid homologue, 75selenium homocholic acid taurine (SeHCAT), to determine the turnover of the bile acid pool.5 6 Severe, moderate, mild and borderline BAD are classified as <5%, < 10%, < 15% and<20% retention of SeHCAT, respectively.7
The adverse impact on living with the condition can be very debilitating. In an online survey of 100 adults in 2015, 38% self-reported with BAD and all others had secondary types including cholecystectomy, ileal resection and inflammation, or other gastrointestinal diseases.8 Despite medical treatment, persisting extreme tiredness and reduced physical activities were self-reported in at least 50%. In a Danish retrospective survey on the long-term effect of treatment by colestyramine, colesevelam, colestipol, loperamide and psyllium, persisting bothersome diarrhoea was self-reported in 273 out of 377 (74%) SeHCAT-diagnosed patients with severe to mild BAD, of which 198 (52%) had BAD.9 Severe diarrhoea impacting on everyday life affected 20% of the whole cohort. The National Institute for Health and Care Excellence recommends research to be undertaken to assess the effectiveness of treatment options for BAD and better understand the HR-QoL in people living with BAD.10
In BAD, the digestion and absorption of dietary fats and fat-soluble vitamins remain maximised by the conversion of bile acids to bile salts for efficient transportation across the small intestine’s brush border.11 Bile salts are passively absorbed along the jejunum, and active absorption follows in the terminal ileum for their return to the liver.12 However, the problem is hepatic bile acid overproduction typically seen in primary BAD causing ileal saturation and, consequentially, excess colonic bile salts induce a prosecretory response of water, potassium and sodium.13 This secretory diarrhoea is also exhibited in BAD postcholecystectomy, with the impact of no gallbladder also reducing orocaecal and colonic transit times14 due to a smaller bile acid pool.15
Treatment to manage symptoms is lifelong pharmacotherapy of bile acid sequestrants (BAS) and anti-diarrhoeal medicines.16 A systematic review of published studies to 2013 showed that for approximately 30% of adults living with BAD, they were inadequately effective.17 Side effects include constipation and abdominal symptoms.18 Intolerability to colestyramine and colestipol is the most common reason for discontinuing medical treatment.19 A recent double-blind, placebo-controlled RCT of colesevelam at a target dose of three capsules two times per day for 12 days supports the use of colesevelam.20 Complete remission from diarrhoea was found in 26 out of 37 patients receiving colesevelam and 37 out of 38 patients receiving placebo, indicating the need for adjunctive therapies. The severity of BAD does not correlate with self-reported diarrhoea,21–23 suggestive of influencing factors such as diet.
Many people living with BAD alter their diet to try to control symptoms.8 24 A reduction in fat intake to 40 g/day is widely believed among the public8 and gastroenterologists16 25 to benefit BAD symptoms. However, the evidence base does not support this belief. A systematic review of dietary interventions in all types of BAD identified no published RCTs and eight prospective cohort studies.26 In primary BAD, one study was found but in only two patients.27 After treatment by colestyramine optimised to 2 to 12 g, reduced intakes of lactose and/or fructose plus sorbitol provided unquantified improvement in diarrhoea. In secondary BAD, seven studies were found in which fat intake was reduced and provided very low certainty of a beneficial direction of effect on diarrhoea.28–34 However, the studies included participants with medical complications known to cause fat malabsorption,35 and in ileal dysfunction, dietary fat induces a secretory effect by inhibiting reabsorption of water and electrolytes, worsening diarrhoea and causing steatorrhoea.36 Out of the seven studies, these included distal ileal resections, with reported resection lengths of 10 to 100 cm,32 8 to 40 cm or the length was unknown,34 or not reported30 in three studies, ileal dysfunction due to radiotherapy in two studies,28 31 extensive ileal lesions in one study,33 exocrine pancreatic insufficiency in two studies30 34 and small intestinal bacterial overgrowth in three studies.30 31 34 In two of the studies, faecal fat losses were reported,29 32 evidencing steatorrhoea even at small resection lengths of 25 and 35 cm.32 However, fat intakes were not measured. Five studies involved a total of 181 patients living with the late effects of cancer treatment and targeted the reduction of fat intake as 40 g per day,28 ‘20% of total energy’,30 34 simply as ‘low-fat’31 or ‘reduced-fat’.29 The two other studies involved a total of nine inpatients, and a liquid, elemental diet containing less than 5 g fat/day was given for short-term ‘bowel rest’.32 33 Therefore, to understand the effect of dietary fat on diarrhoea in BAD, studies are needed that do not exhibit ileal dysfunction and other clinical conditions that cause fat malabsorption. Food is a complex matrix of dietary components other than fat, and no studies have comprehensively evaluated nutrient intakes or diet quality. High-quality diet studies are needed that describe interventions in sufficient detail to enable replication.
Furthermore, perceived food intolerance and consequential food avoidance have been found to be high in BAD. In an online cross-sectional survey conducted in 2021 over 4 weeks in 434 UK adults who reported that they had been diagnosed using the SeHCAT test, the prevalence rate of food intolerance was very high (88%).24 Persisting diarrhoea was identified in 80% (333 of 416), despite ongoing use of BAS and loperamide in the vast majority (93%). Prevalence rates on avoiding fatty foods, all types of dairy, and fruit and vegetables were 30%, 20% and 15%, respectively. More studies are also needed,37 and these should initiate understanding of the diet quality and nutrient intakes in BAD.
This parallel group, feasibility RCT aims to evaluate trial feasibility and acceptability of conducting a fully powered RCT for a dietitian-counselled, healthy dietary pattern (The 8×5 Diet) compared with usual care for 8 weeks in adults living with BAD and ongoing diarrhoea in the UK. The aim is in accordance with the methods recommended by the Medical Research Council and National Institute for Health and Care Research for developing and evaluating complex interventions.38 Objectives are to:
Calculate rates on consent, recruitment, randomisation and retention.
Assess the acceptability of the data collection instruments.
Assess the practicalities of running a trial in relation to consent, recruitment, randomisation, retention and the data collection instruments.
Assess the acceptability and safety of the intervention.
Obtain initial estimates of effect size from outcomes to inform the primary outcome for a future definitive RCT.
The trial will be reported following the Standard Protocol Items: Recommendations for Interventional Trials guidelines39 and the Consolidated Standards of Reporting Trials extension to randomised pilot and feasibility trials.40
Methods and analysis
Study setting, sample size and recruitment
The study will be conducted remotely using digital technologies (video-conferencing, websites, social media, email, text messaging using participants’ computers, laptops, smartphones, tablets) between 2 April 2024 and 30 April 2025.
As this is a feasibility study that is not designed to detect a targeted difference in the secondary outcomes, a sample size calculation was not appropriate. For feasibility studies, good practice guidance suggests a sample of at least 30 individuals to estimate a parameter with the necessary level of precision.41 Therefore, a sample size of 30 participants was chosen for each group. A 20% attrition rate for each group over the recruitment and delivery period of 12 months is estimated, and so the total target sample size is 76 participants.
Identification of potential participants will be from advertising of the study in the BAD UK website,42 and related national, patient and public, and research organisations; social media (Facebook: two groups from the membership of BAD UK and social media); and a database held from a previous study in BAD on the resources for this trial where participants gave consent for their details to be used in other studies. Interested potential participants will contact the researchers (YM) via telephone or email and be invited to discuss the study, access the study’s website43 and receive the Participant Information Sheet (online supplemental material S1).
Supplemental material
Eligibility and consent
Eligibility will be assessed by a researcher-completed bespoke screening tool and an eligibility questionnaire completed on screen in Zoom to meet the eligibility criteria presented in table 1 and in online supplemental files 1 and 3. Those who are eligible and willing to participate will be emailed the informed consent form to complete by the research team (YM) and e-sign to enable progression to enrolment. Those who are ineligible or decline participation will have the reason anonymously recorded if voluntarily shared.
Supplemental material
Inclusion and exclusion criteria
Allocation
Participants will be 1:1 randomly allocated to the intervention or control group. Randomisation using random permuted blocks to generate the allocation sequence will be performed using an online randomisation service44 by a researcher from the University of Manchester not involved in the study. Blinding of the allocation to participants and the researchers will not be possible.
The participant timeline is outlined in figure 1. Details on study procedures are in the participant information sheet (in online supplemental file S1).

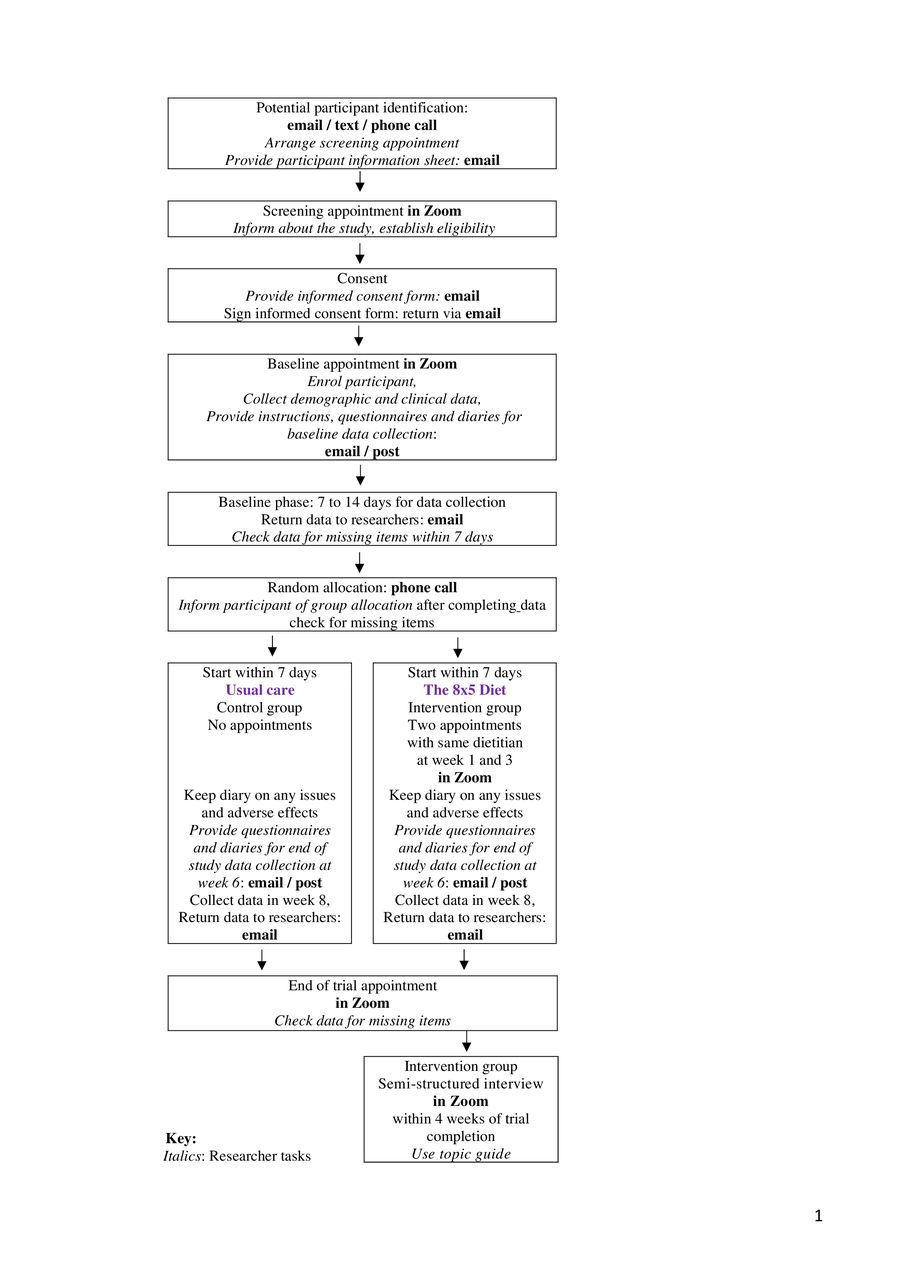{kind=link}
Flow diagram of participants through the study.
Interventions
Participants allocated to the control group will continue their usual dietary pattern. No advice will be provided, other than to continue to take their current medications and attend usual healthcare professional follow-ups.
Participants allocated to the intervention group will be counselled to follow The 8×5 Diet, a healthy dietary pattern designed for adults living with BAD. The intervention is structured on six dietary and four behaviour change components to optimise diet quality and nutrient intakes and was designed to have the potential for use in clinical practice for the management of BAD.
The dietary components include having a fat intake of 40 g/day through five meals and snacks per day and up to 8 g fat per eating session; the addition of specific foods to increase colonic water-holding capacity; ensuring adequate hydration across each day, and encouraging increases in the intakes of fruit, vegetables and whole grains from a broad range. It is framed on the UK’s Eatwell guide, an instrument used to define UK government recommendations on what constitutes a healthy, balanced diet.45
The intervention will be delivered as one-to-one counselling by a specialist gastroenterology dietitian (YM). To follow a ‘real-world’ dietetic counselling approach, the British Dietetic Association’s ‘The ‘Model and process for nutrition and dietetic practice’46 will be used. This process starts with identifying the participant’s nutritional and dietetic needs and works through six consecutive stages of assessing, identifying, planning, implementing, monitoring and reviewing, to evaluating the nutrition and dietetic intervention. A checklist at each appointment will be used to implement these processes.
To optimise adoption of the intervention, behaviour change techniques were selected for counselling on each dietary component when grocery shopping, at home, on the go and dining out, based on the behaviour change technique taxonomy.47 Selected techniques include goal setting (behaviour), instruction on how to perform the behaviour, problem-solving, removing aversive stimulus, prompts, social support, habit formation, self-monitoring, action planning, review of dietary components and feedback.
To standardise delivery and implementation of the intervention, digital resources will be provided. These include a manual, a 34-recipe booklet and four aids for meal planning and monitoring. They were designed to be considerate of food cost, time for grocery shopping and meal preparation, popular meals and treats in the UK, and those who are vegetarian or vegan, with the information offered in an accessible format. Their development was informed by findings from a cross-sectional survey among 343 adults living with BAD24 and the lived experience of adults with BAD and UK dietitians, in accordance with methods recommended by the Medical Research Council.38 Further details on the intervention, following the Template for Intervention Description and Replication checklist,48 are in online supplemental file S2.
Supplemental material
Data collection
The schedule of the study assessments and outcome measures is presented in table 2.
Schedule of the study’s assessments and outcome measures
At the baseline appointment, sociodemographic and past medical history data on biological sex, age, ethnic group, marital status, work status, education, home location, grocery shopping, meal preparation, physical activities, past medical history and nutritional supplements will be collected on screen using a questionnaire with the researcher (YM) (online supplemental file 3).
Clinical status and any changes to medication will be checked at appointments and recorded in the case report form for that appointment.
To maximise completeness of data collection, all completed instruments will be checked by the researchers (YM), recording the number of missing items on instruments before seeking prearranged clarification with participants.
Complete dietary adherence is considered unrealistic49 during events such as celebrations and holidays when increased food intake and deviation from usual dietary patterns are likely. To mitigate this, the timeline will be discussed with each eligible participant to ensure such events do not fall within the data collection periods.
Persisting diarrhoea
Persisting diarrhoea will be assessed at eligibility screening using the Hjortswang criteria50 and the Bristol stool form (BSF) scale,51 via self-report. The Hjortswang criteria are unvalidated for use in BAD but are recommended by European expert consensus for measuring diarrhoea in microscopic colitis in clinical practice.52
Bristol stool form scale
Widely used in UK clinical practice, the validated BSF scale measures patient-reported or clinician-reported stool consistencies pictorially using seven stool form types.51 Diarrhoea is defined as BSF types >5.5 Stool consistencies will be participant-reported in the 7-day food and symptom diary. At the end of each day, participants will total the number of bowel movements and the number of stools that were watery (types 6 and 7).
Height and body weight
Participants will be asked to measure their height in accordance with national standards on measuring height.53 They will be asked to measure their body weight using digital or analogue bathroom weighing scales. Standard operating procedures will be provided. Data will be collected in the food and symptom diary.
Primary outcome
On feasibility and acceptability, we will:
Assess consent: percentage of participants that consent to participate in the trial compared with the percentage that were screened for eligibility
Assess recruitment: percentage of participants randomised compared with the percentage that were screened for eligibility
Assess randomisation: percentage of participants that complete their first appointment compared with the percentage that were randomised, intervention group only
Assess retention: percentage of participants that complete the trial compared with the percentage randomised to each group.
Assess the proportion of missing data from questionnaires identified by the research team on: demographics and clinical (13 items), diet quality (23 items), diet acceptability (10 items) and HR-QoL (36 items).
Explore participants’ views and experiences on participating in the study via interviews using a topic guide that considers the study procedures, data collection instruments and acceptability of the intervention (online supplemental file 3).
Secondary outcomes
Health-related quality of life
There is no HR-QoL measure specific to BAD. HR-QoL will be assessed using the 36-item short-form health questionnaire SF-36v2.54 It measures eight domains to provide physical and psychological composite scores.
Participant-reported BAD symptom relief
BAD symptom relief will be measured using the global symptom question for functional gastrointestinal disorders, ‘did you have adequate relief of your symptoms over the past 7 days?’.55 The Yes/No response will be collected on the last day of the food and symptom diary.
Participant-reported change in diarrhoea
This will be assessed as the difference in the mean number of stool types 6 and 7 per day at baseline compared with trial endpoint in each group.
Participant-reported change in stool frequency
This will be assessed as the difference in the mean number of bowel movements per day at baseline compared with trial endpoint in each group.
Safety
Safety will be defined as type and number of adverse effects in the intervention group compared with those in the control group, identified from a participant-reported bespoke diary on adverse effects during trial duration (online supplemental file 3). An adverse effect is defined as any symptoms or worsening of symptoms which the participant considers to be related to the trial. All adverse events will be reported in accordance with the University of Manchester’s policy on adverse events.
Diet quality and nutrient intakes
Diet quality will be assessed by using the Healthy Diet Index (HDI) which measures adherence to a healthy whole diet.56 The HDI consists of seven weighted domains, 18 items as 23 questions: meal pattern (10 points), fruit and vegetables (20 points), fats (15 points), whole grains (20 points), fish and meat (10 points), dairy (10 points), salty and sugary snacks and beverages including alcohol (15 points), with a score range of 0 to 100. It was validated in Finland for use in clinical practice but not in the English language or in the UK. For applicability to the UK population and for this cohort, minor modifications to the answers for three out of 18 questions were made on cooking oils and fats, spreads and meat.
Nutrient intakes will be assessed from participant-recorded food intake data. Food intake data will be collected prospectively using a bespoke 7-day food diary of weighed food and beverages, structured by when in the day the item or meal was consumed, preparation/cooking method used and quantity consumed (Online supplemental file 3). Standard operating procedures will be provided and include how to photograph meals using their smartphone using the Remote Food Photography method.57 Food intake from submitted images of meals or items will be researcher-assessed for weights. Participants may print the diary template to collect data on paper but must then return the diary electronically by emailing screenshots of each page. To reduce participant burden, we will offer to post the food diaries. Record data on food, fluids including alcohol and psyllium, and excluding vitamin and mineral supplements will be researcher-entered into an online nutrition analysis software system58 by one dietitian (YM) to calculate daily intakes of energy, macronutrients, 23 micronutrients and total fat intakes per eating session (breakfast, mid-morning, lunch, mid-afternoon, evening) at baseline and week 8. Nutrient intakes will be compared with national UK dietary reference values59 and recommendations for nutrient intakes where available.60 61 If wanted, participants will receive their individual nutrient reports after study completion via email.
Acceptability of The 8×5 Diet
Acceptability of the dietary intervention will be measured by using the Diet Satisfaction Score (DSS).62 This instrument is a validated, self-report 10-item questionnaire using a 5-point Likert scale to calculate a mean total DSS from a possible range of 1 (least satisfaction) to 5 (greatest satisfaction). A score above 3.0 indicates acceptability.
Analysis methods
Statistical analyses will be performed using IBM SPSS Statistics 28. Quantitative data will be summarised using descriptive statistics. Primary endpoints and other categorical variables will be presented as frequencies and proportions. Continuous variables will be presented as means with 95% confidence intervals or medians with inter-quartile ranges. Between-group changes in outcomes at baseline and at 8 weeks of the intervention will be tested using statistical approaches as appropriate. To explore changes in the potential main outcomes for a future RCT, multiple regression modelling will be performed with the main outcomes for the purposes of hypothesis generating.
Missing data will be imputed by using the last observation carried forward method. Subgroup analysis is not planned. Data from all randomised participants will be analysed using an intention-to-treat principle, modified to exclude those who were randomised but did not start the intervention. Per protocol analysis will include participants who completed the trial without violation of the protocol.
To analyse the qualitative data, the Framework Method63 will be used, managed in NVivo 12 software (V.12, Lumivero). To ensure rigour of the analysis process, the seven stages involving transcription, data familiarisation, coding, developing a working analytical framework, applying the framework, data charting, and data interpretation64 will be discussed and reviewed by at least two researchers (YM and SB).
To inform on study progression to a powered RCT, the feasibility outcomes will be assessed as an overall binary outcome of whether all components of the trial can work together or not,40 in accordance with the progression criteria identified by Shanyinde et al.65 If appropriate to progress, initial estimates of sample size will be calculated for a fully powered RCT.
Ethics and dissemination
Ethical approval was granted by the University of Manchester Research Ethics Committee 5 (2024-19094-33261) on 25/03/24. Written, informed consent will be obtained from those who are willing to participate by the researchers (YM) using email (in online supplemental file S1). Those who are ineligible or decline participation will have the reason anonymously recorded, if voluntarily shared. Their understanding of their involvement will be checked prior to enrolment. The right of an individual to refrain from participation or to withdraw at any time from the study without giving a reason will be respected and without prejudicing their further healthcare. If they withdraw consent on any further involvement, all further data would not be asked to be completed, and data to this point will be used in analyses. If possible, participants will be asked to complete data. Reasons for withdrawing will be collected if willingly provided. Notification of any changes in a participant’s medical condition or deviation from the protocol will be discussed with the participant and study team (CT, SB, YM) to determine whether violation from the protocol will justify discontinuation. The study will be conducted in accordance with the Declaration of Helsinki guidelines.
Personal information will be pseudonymised, and all collected data accessible to only this study’s researchers will be managed and securely stored in accordance with the University of Manchester’s policies on data protection, the data controller for this study, and in line with UK General Data Protection Regulation. Details of data management procedures are published in DMPonline (https://dmponline.dcc.ac.uk, ID: 139696) via the University of Manchester.
Study findings will be disseminated to study participants, the BAD UK and trial websites, social media (X), by publication in peer-reviewed journals and at national meetings. For sharing purposes, a completely anonymised data set will be archived in the University of Manchester’s repository indefinitely.
Patient and public involvement
From the early developmental stages of this research process, this work has been supported by BAD UK, the UK’s leading charity for information, help and support for people living with BAD. Drawing on the lived experience of patients and the public with BAD, focus group discussions were conducted for developing this research proposal. Their feedback improved the acceptability and readability of the participant resources and influenced trial design. Group discussion involving three members of BAD UK, two of which are co-authors, guided on the final trial design including on eligibility, advertising and recruitment, choice of trial instruments, participant burden and experience, as well as dissemination of the study results.
Discussion
This study is the first feasibility RCT to be conducted in the UK for people living with BAD and ongoing diarrhoea.
Strengths of this study include the use of explicit feasibility criteria as the primary outcome. The mixed methods approach ensures that patient perceptions, their values and context are gained for application to the design of a larger trial. The parallel trial design reflects ‘real world’ clinical practice. However, due to the pragmatic nature of the treatments, the trial will be unblinded to all. These data will provide new knowledge on diet quality and the intakes of a wide range of nutrients.
The comparator chosen is in line with recommendations for RCTs of diet interventions involving gastrointestinal symptoms.66 Incentives for participation will not be provided. Potential participants will not be informed that the purpose of the intervention is to improve diarrhoea, since optimal design includes using neutral language to mask this hypothesis.67
The patient population targeted was identified as urgently needing diet therapy.26 Reduced HR-QoL impacting on everyday living indicates that the use of telemedicine to conduct and deliver the intervention is appropriate so that participants can stay at home near a toilet. In the UK, 96% of the population is online, but a small proportion may be excluded from participating due to digital incompetency, cost of living, and fraud.68 Australia Dietitians recommends the delivery of dietetic consultations as a cost-effective alternative to in-person delivery.69
Recruitment is limited to self-selected sampling across the UK and likely to be biased to those interested in dietary modification and higher levels of motivation to make changes. A national registry for BAD does not exist to enable purposive sampling. At recruitment, this study is susceptible to selection bias. To reduce this, we will not limit the trial to those who are naïve to fat intake reduction. All assessments rely on accurate self-reporting, in particular of food intake, and it will be impossible to know the accuracies of the weighting scales used. To reduce response bias relating to underreporting of food intake, participants will be asked to not alter their behaviours and record everything consumed, including water and alcohol intakes. The precision of estimating nutrient intakes will be maximised by providing comprehensive written and verbal instructions prior to and during the baseline appointment, asking participants to prospectively weigh all food, using a 7 day period, and cross-checking the data with participants within 7 days of completion.
Ethics statements
Patient consent for publication
Acknowledgments
Elizabeth Smith, BAD UK.
References
Footnotes
X @digestnutrition, @Prof_Chris_Todd
Contributors All authors contributed to the design of the study. The manuscript was drafted by YM.All authors read and approved the final manuscript. SB is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.