Article Text

Abstract
Objectives To investigate clinical characteristics, symptom profile, testing practices, treatment patterns and quality of life (QoL) among patients with pulmonary arterial hypertension (PAH) in Latin America.
Design Data from the Adelphi Real World PAH Disease Specific Programme, a cross-sectional survey with retrospective data collection.
Setting University/teaching hospital, regional centres, private practices and government institutions in Argentina, Brazil, Colombia and Mexico.
Participants 246 physicians provided data for 958 patients, of which 533 patients also self-reported data.
Results Mean (SD) patient age was 53.7 (17) years, 70% of patients were female and 79% were WHO functional class (WHO FC) I–II. Overall, 76% had undergone a right heart catheterisation, ranging from 92% in Argentina to 64% in Brazil (p<0.0001). Only 28% underwent a simplified risk assessment strategy in the past 12 months, ranging from 46% in Argentina to 16% in Brazil. Fatigue and dyspnoea on exertion were reported most commonly by physicians (37% and 53%) and patients (68% and 67%). Patient–physician agreement on symptom reporting was minimal-to-weak (kappa, 0.21–0.42). PAH-specific combination therapy varied across countries (21% Mexico, 30% Brazil, 70% Colombia and 79% Argentina, p<0.0001)). Overall, 73% of patients received a phosphodiesterase type 5 inhibitor; 52% an endothelin receptor antagonist, 15% a prostacyclin pathway agent and 11% a soluble guanylate cyclase stimulator. The mean (SD) EQ-5D (generic instrument to define quality of life)utility ranged from 0.66 (0.20) to 0.70 (0.20) across countries and the mean (SD) EQ-5D Visual Analogue Scale (VAS) was 67.0 (18.10). Lower VAS and utility scores were reported among patients with higher WHO FC (p<0.05).
Conclusions Patients reported a high burden of PAH in terms of symptoms and QoL, particularly within higher WHO FC. Low usage of risk assessment strategies and PAH-specific combination therapy was seen in Brazil and Mexico. Further research could identify barriers to prescribing optimal treatment.
- Pulmonary Disease
- Hypertension
- Patients
- Physicians
Data availability statement
Data are available upon reasonable request. All data, that is, methodology, materials, data and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to MS at mark.small@adelphigroup.com. MS is an employee of Adelphi Real World.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is a real-world study, providing insights into real treatment practices occurring in clinics in Latin America, without external influence or intervention.
The study was conducted in Latin America (Argentina, Mexico, Colombia and Brazil), providing valuable information about pulmonary arterial hypertension (PAH) practices in a poorly studied region.
The Adelphi Real World PAH Disease Specific Programme methodology used in this study is not based on a true random sample of physicians or patients; rather, the patient population is a pseudorandom sample of the consulting PAH population, influenced by physicians’ and patients’ willingness to participate.
The study was conducted during the COVID-19 pandemic from December 2020 to September 2021, with varying restrictions in place at different times during the data collection period. This may have resulted in a bias towards patients least likely to contract COVID-19 or those most able to attend their study clinic.
There is some disparity among countries in the proportion of physicians who were affiliated with PAH specialist centres, ranging from 18% in Brazil to 71% in Argentina. Although this is a reflection of the real-world nature of this study, it may potentially limit the validity of certain direct country-to-country comparisons.
Introduction
Pulmonary arterial hypertension (PAH) is a rare, progressive and incurable disease1 characterised by elevated pulmonary vascular resistance resulting in right ventricular failure.2 PAH is classified into different subtypes according to the underlying disease pathogenesis, including idiopathic PAH (IPAH), heritable PAH (HPAH) and PAH associated with other conditions (APAH) such as connective tissue disease.3 4
International guidelines both at the time of the survey and currently mandate the use of right heart catheterisation (RHC) to confirm a diagnosis of PAH.3–5 Further recommendations include determining the initial treatment for newly diagnosed patients by stratifying patients into three strata (low-risk, intermediate-risk or high-risk) based on expected 1-year mortality.3–5 At least a basic risk assessment strategy, consisting of the WHO functional classification (FC), a right ventricular function evaluation through brain natriuretic peptide (BNP/Pro-BNP) and a 6-minute walk distance test, among others, was strongly recommended to assess prognosis6 and determine treatment strategy. Due to its impact on delaying disease progression, upfront combination therapy became the standard of care for the vast majority of patients.7 8
Patients who are adequately diagnosed via RHC, stratified by risk status and who receive appropriate, guideline-driven therapy experience a significant improvement in life expectancy, in contrast to those with untreated IPAH, for whom the mean survival is 2–3 years.9 This highlights the critical importance of identifying patients early and offering guideline-recommended treatment as a priority. Therefore, it is important to explore the characteristics of patients affected by PAH to understand why they may not be receiving optimal therapy.
Although PAH burden is well studied in Europe and the USA,10–12 low- and middle-income regions such as Latin America have been largely overlooked in disease reviews,13 despite stark reported differences in patient profiles compared with other regions.13–17
There is a need to evaluate PAH epidemiology and real-world clinical practices in Latin American countries to understand the demographic profile of patients with PAH, disease characteristics, treatment patterns and identify any discordance between current guideline recommendations and real-world clinical practice.
This study aimed to investigate clinical characteristics, symptom profile, patient/physician symptom alignment, testing practices, treatment patterns and quality of life (QoL) among patients with PAH. This study also looked to identify any differences in patient management between geographical setting, disease severity as measured by WHO FC, patients consulting with physicians affiliated with an accredited PAH centre compared with physicians based in non-affiliated settings and those with or without a recorded RHC.
Methods
Data were drawn from the Adelphi Real World PAH Disease Specific Programme (DSP), a real-world, cross-sectional survey with retrospective data collection of physicians and their consulting patients with PAH, conducted in four Latin American countries from November 2020 to March (Argentina), August (Mexico) and September (Brazil and Colombia) 2021. The methodology has been previously described,18 19 validated20 and demonstrated to be representative and consistent over time.21 The study design is illustrated in online supplemental figure 1.
Supplemental material
Survey population
Physicians (pulmonologists or cardiologists) were eligible if they were personally responsible for the management of patients with PAH and saw a minimum of two patients with PAH per month in Argentina, Brazil, Colombia or Mexico. Patients were eligible for inclusion if they were ≥18 years of age with a physician-confirmed diagnosis of WHO group 1 PAH and were not enrolled in a clinical trial at the survey date.
Data collection
Physicians completed online patient record forms (PRFs) for the next five consecutively consulting patients who visited the physician in person for routine care. PRFs captured patient demographics, disease characteristics and treatment history for patients with PAH. Physicians completed the PRFs through consultation of existing patient clinical records, as well as using their judgement and diagnostic skill, which is consistent with the decisions made in routine clinical practice. No follow-up information was collected.
Patients for whom physicians completed a PRF were then invited to voluntarily complete a pen and paper patient self-completion form (PSC) independently of their physician, to capture their own perspective on the impact and specificities of their condition. PSCs contained validated instruments to assess patient-reported health-related quality of life (HRQoL). PRF and PSC data were matched anonymously using physician/patient survey numbers to allow comparison between physician and patient-reported data.
Measures and variables
Physician demographics and physician-reported patient demographics were recorded. Physicians reported on patient clinical characteristics using the WHO FC assessment: FC I = no limitations in daily physical activities, no symptoms of dyspnoea with routine exertion; FC II = mild symptoms with exertion, no symptoms at rest; FC III = moderate dyspnoea with routine activities and activities of daily living, no symptoms at rest; and FC IV = inability to perform even minimal activities, dyspnoea present at rest. PRFs also captured PAH disease classification (APAH, IPAH or HPAH) and symptom data (number, type, severity in the 4 weeks prior to survey date and age at symptom onset). Data regarding diagnostic tests and any tests conducted over the year prior to the survey data were collected. Where patients were recorded as having undergone WHO FC, BNP and 6-minute walk distance test (6MWT) in the year prior to the survey date, this was defined as the patient having undergone a simplified risk assessment strategy. Treatment information was also captured.
Patients reported their PAH symptom experience for the 4 weeks prior to the survey date and their HRQoL at the survey date using the five-level version of the EQ-5D and the EuroQol Visual Analogue Scale (EQ VAS). EQ-5D index scores were calculated according to country-specific tariffs, in which scores begin at 1 (indicating a full health state) and are negatively scored to 0 (indicating a health state equivalent to dead). Via the EQ VAS, patients provided a score of their current health on a scale from 0 (‘The worst health you can imagine’) to 100 (‘The best health you can imagine’).22
Physicians and patients were provided with 15 matched symptom options in list form, with accessible terminology used within the PSC. The presence and severity of symptoms were reported via tick box, including a ‘Don’t know’ option and open-text responses for symptoms not listed.
Statistical analysis
Results were delineated by country, WHO FC, RHC status and whether or not the physician was affiliated with a PAH specialist centre (use of combination therapy only). Descriptive analysis was used to summarise variables and compare characteristics of groups. Due to the variability and availability of data extracted from patient clinical records, missing data were not imputed. Therefore, the base number of patients for analysis could vary from variable to variable and was reported separately for each analysis.
Univariate/bivariate analysis was also used and involved the comparison of outcomes between two or more patient groups. The type of test used depended on the type/distribution of the outcome variable. For comparisons between two patient groups, t-tests were used for numeric variables, Fisher’s exact tests were used for binary categorical variables and Mann-Whitney U (non-parametric) tests were used for numeric variables where the t-test assumptions were violated. For comparisons between three or more patient groups, analysis of variance (ANOVA) was used for numeric variables, Kruskal-Wallis (non-parametric) tests were used for numeric variables where the ANOVA assumptions are violated and χ2 tests were used for categorical variables with more than two groups.
Level of concordance between physician- and patient-reported symptoms was assessed using a weighted kappa statistic and interpreted as defined by Cohen’s kappa, such that 0.0–0.20=no agreement; 0.21–0.39=minimal; 0.40–0.59=weak; 0.60–0.79=moderate; 0.80–0.90=strong and >0.90=almost perfect agreement.23
Patient and public involvement
Patients were not involved in the design, or conduct, or reporting, or dissemination plans of our research.24
Results
In total, 246 physicians across four Latin American countries (Argentina, n=47; Brazil, n=74; Colombia, n=56; Mexico, n=69) completed forms for 958 patients with PAH. A total of 533 patients completed the voluntary PSC. Physician and patient sample numbers are summarised in online supplemental table 1.
Study population
Overall, 55% of physicians were pulmonologists and 45% were cardiologists (online supplemental table 2). In total, 41% of participating physicians were affiliated with a PAH specialist centre, ranging from 18% in Brazil, 41% in Mexico, 43% in Colombia, to 71% in Argentina (online supplemental table 3). The mean (SD) age of enrolled patients was 53.7 (17) years, ranging from 51.0 (17) in Colombia to 58.2 (17) in Brazil. Patients within WHO FC I–II were younger (53.117 years) than those within WHO FC III–IV (56.118 years; p=0.0314). Patients with a recorded RHC were younger than those without (51.117 vs 62.017 years, respectively; p<0.0001, online supplemental table 2). Most patients (70%) were female, ranging from 62% in Brazil to 77% in Argentina (p=0.0031). The mean (SD) time since PAH diagnosis was 2.9 (2.4) years. At the survey date, the majority of patients (79%) were classified as WHO FC I–II, with 21% classified as FC III–IV, compared with 33% of patients classified as WHO FC I-II and 64% classified as WHO FC III-IV prior to first initiation of treatment.
Overall, 14% of patients were in full-time employment, ranging from 7% in Colombia to 18% in Mexico (p=0.0013). Patients with WHO FC I–II were four times more likely to be working full time compared with WHO FC III–IV (16% vs 4%; p<0.0001). A similar proportion of patients with a recorded RHC were working full time (12%) to those with no recorded RHC (19%; p=0.0157).
APAH was the most common class of PAH (60% overall compared with 37% IPAH and 3% HPAH), and the proportion of patients with APAH varied from 49% in Colombia to 70% in Mexico (p<0.0001). The most frequent form of APAH was connective tissue disease (54%), followed by congenital heart disease (32%). Patients without a recorded RHC were more frequently diagnosed with APAH (70%) compared with those with a recorded RHC (57%; p=0.0007).
Diagnostic and clinical testing
The proportion of patients reported to have undergone RHC varied across countries (Argentina, 92%; Brazil, 64%; Colombia, 87%; Mexico, 69%; p<0.0001). Among patients consulting a physician based within a pulmonary hypertension expert centre, 92% had received an RHC compared with 65% of patients consulting physicians based in non-specialised settings (p<0.0001). This differed between markets (Argentina, 99% in a specialist centre vs 68% in a non-specialist centre, p<0.0001; Brazil, 80% in a specialist centre vs 62% in a non-specialist centre, p=0.0185; Colombia, 98% in a specialist centre vs 78% in a non-specialist centre, p<0.0001; Mexico, 81% in a specialist centre vs 60% in a non-specialist centre, p=0.0005).
An echocardiogram was the most frequently performed physician-reported test overall and in each country (online supplemental table 4).
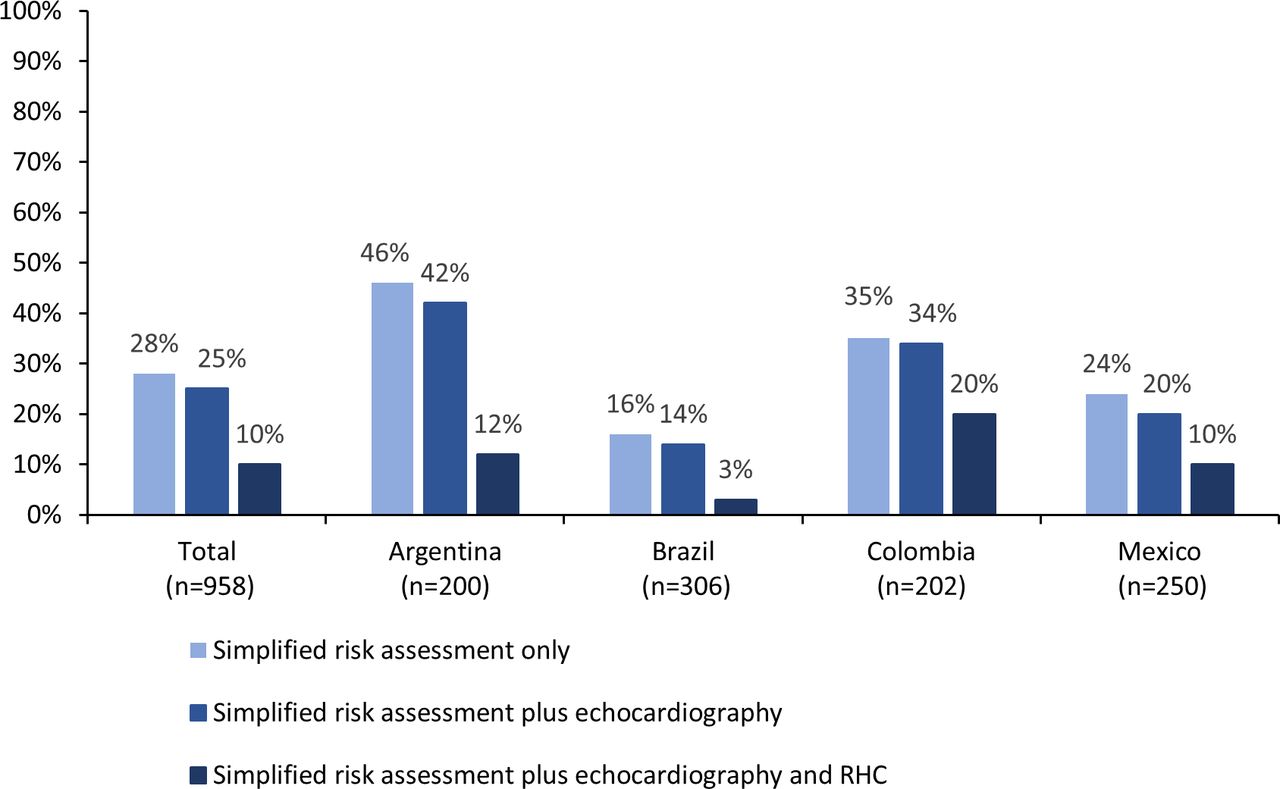
In the 12 months prior to the survey date, only 28% of all patients were indicated to have undergone a simplified risk assessment strategy (WHO FC, BNP, 6MWT). There was considerable variation in the proportion of patients undergoing the risk assessment strategy across countries (figure 1). A small proportion of patients in each country (25%) had undergone a simplified risk assessment strategy plus an echocardiogram, and even fewer (10%) had the addition of an RHC. Base sizes are reported in figure 1.

Percentage of patients who underwent the simplified risk assessment, including echocardiography and RHC by country (% of patients). RHC, right heart catheterisation. Base size: simplified risk assessment only (total, n=217; Argentina, n=91; Brazil, n=49; Colombia, n=71; Mexico, n=60); simplified risk assessment plus echocardiography (total, n=243; Argentina, n=83; Brazil, n=43; Colombia, n=68; Mexico, n=49); simplified risk assessment plus echocardiography and RHC (total, n=98; Argentina, n=24; Brazil, n=9; Colombia, n=40; Mexico, n=25).
Most commonly reported symptoms and symptom alignment
The mean (SD) patient-reported age at first PAH symptoms was 46.4 (19) years, with shortness of breath being the first symptom noticed by 78% of patients, followed by fatigue (65%) and chest pain/pressure (34%).
The mean (SD) number of physician-reported patient symptoms experienced in the 4 weeks prior to the survey date increased with WHO FC from a mean (SD) of 3 (2) symptoms in FC I–II to 6 (4) symptoms in FC III–IV. The proportion of patients experiencing at least one physician-defined severe symptom also increased with WHO FC, from 8% in FC I–II to 54% in FC III–IV (p<0.0001). A similar mean (SD) number of symptoms was reported for patients with versus without a recorded RHC (3.9 (3.3) and 3.5 (3.3), respectively; p=0.1231).
Fatigue/tiredness and dyspnoea on exertion were the most common symptoms reported in the 4 weeks prior to the survey date by both physicians (37% fatigue and 53% dyspnoea on exertion) and patients (68% fatigue and 67% dyspnoea on exertion, online supplemental table 5; online supplemental figure 2). Symptoms were more frequently reported by the patient than their physician, with minimal-to-weak alignment between physician and patient reports of the presence and severity of symptoms (kappa statistic score, 0.21–0.42 across symptoms, online supplemental table 5). All symptoms were reported with a greater frequency by patients within WHO FC III–IV compared with FC I–II (p<0.0001, online supplemental table 5)
Current treatment prescription
Overall, 80% (n=766) of patients were receiving treatment for their PAH at data collection. By treatment class, 73% of patients were receiving a phosphodiesterase type-5 inhibitor (PDE5i), 52% received an endothelin receptor antagonist (ERA), 15% received a prostacyclin pathway agent and 11% received a soluble guanylate cyclase stimulator (SGCS). Differences were noted among countries with respect to classes of treatment prescribed. In Argentina, 88% of patients were receiving a PDE5i compared with 68% in Brazil, 56% in Colombia and 81% in Mexico (p<0.0001). ERAs were prescribed to 81% of patients in Argentina, 36% in Brazil, 72% in Colombia and 25% in Mexico. SGCSs were prescribed to 3%, 0%, 36% and 7% of patients in Argentina, Brazil, Colombia and Mexico, respectively.
Little difference in the currently prescribed regimen between WHO FC was seen. However, patients who had undergone RHC for diagnosis of their PAH were more likely to receive treatment with an ERA (61% vs 19%; p<0.0001) or a prostacyclin pathway agent (18% vs 3%; p<0.0001).
Combination therapies
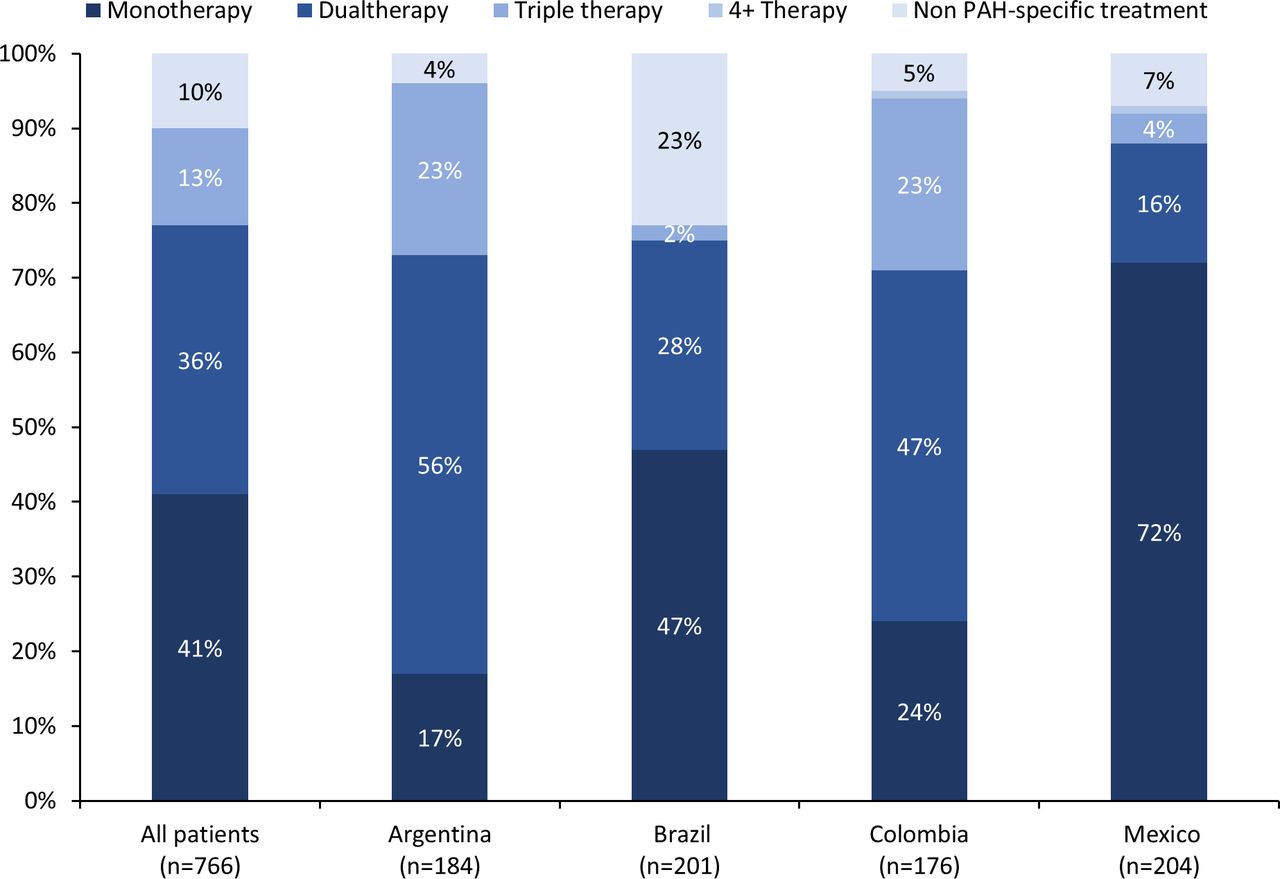
Combination therapy using PAH-specific treatments (any of the two following treatment classes: ERAs, PDE5i, SGCS or prostacyclin pathway agents) was prescribed to 49% of patients (figure 2), with 67.2% of patients consulting with a physician affiliated with an accredited PAH centre receiving combination therapy compared with 31.7% of patients consulting physicians based in non-affiliated centres (p<0.0001). Overall, the proportion of patients treated with combination therapy varied across countries (21% Mexico, 30% Brazil, 70% Colombia and 79% Argentina; p<0.0001); however, the variation is lower if only patients followed at affiliated centres are considered (33% Mexico, 57% Brazil, 78% Colombia and 85% Argentina; p<0.0001) (online supplemental figure 3).

PAH-specific treatment type prescribed by country (% of patients). PAH, pulmonary arterial hypertension. PAH-specific treatment includes any treatment from the following classes: endothelin receptor antagonists, prostacyclin pathway agents, soluble guanylate cyclase stimulators and phosphodiesterase type 5 inhibitors. Non-PAH-specific treatment includes treatment with calcium channel blockers, supportive therapies (diuretics, oxygen, anticoagulants) and other therapies (was an open-ended response code).
Usage of combination therapy was similar across WHO FC (48% in FC I–II and 51% in FC III–IV; p=0.5839). Patients with a recorded RHC were more frequently prescribed PAH-specific combination therapy than those without a recorded RHC (57% vs 6%; p<0.0001). The proportion of patients prescribed combination therapy differed by the time since PAH diagnosis (23% <1 year (n=116), 52% ≥1 year and <3 years (n=301) and 60% 3 years and above).
The most frequently prescribed dual therapy treatment was a PDE5 inhibitor alongside an ERA (83%). Patients receiving triple therapy were most commonly prescribed a PDE5 inhibitor and ERA in combination with a prostacyclin pathway agent (71%).
Patient-reported HRQoL
Mean (SD) EQ-5D index scores were similar across countries, ranging from 0.66 (0.20) in Mexico to 0.70 (0.20) in Argentina, Brazil and Colombia (figure 3).

{kind=link}
{kind=link}
{kind=link}
EQ-5D-5L index score by country and delineated by WHO FC. EQ-5D index scores were calculated according to country-specific tariffs, scores begin at 1 (indicating a full health state) and are negatively scored to 0 (indicating a health state equivalent to dead) (EuroQol Group, 2001). Base size: Argentina (WHO FC I–II, n=106; WHO FC III–IV, n=33); Brazil (WHO FC I–II, n=50; WHO FC III–IV, n=14); Colombia (WHO FC I–II, n=85; WHO FC III–IV, n=19) and Mexico (WHO FC I–II, n=128; WHO FC III–IV, n=43). FC, functional class.
Mean (SD) health state score as measured by EQ-5D VAS was 67.0 (18.1). Scores were similar across countries, ranging from 64.5 (20.1) in Argentina to 69.1 (17.4) in Mexico (p=0.1512).
Lower mean (SD) scores were observed among patients with a higher WHO-FC; 69.8 (16.2) versus 57.1 (19.7) for WHO FC I–II and WHO FC III–IV, respectively (p<0.0001). Lower mean (SD) EQ-5D VAS and index scores were reported by patients with a higher WHO FC in each country (p<0.05).
Discussion
The results of this real-world study provide a clear overview of the demographic and clinical characteristics, symptom profile, testing, treatment and HRQoL of patients with PAH in Latin America. It is important to consider the differences in healthcare systems and treatment availability both within Latin American countries and between Latin America and the rest of the world (online supplemental table 6).
In our study, mean patient age was comparable to other Latin American studies which have reported mean patient age ranging from 41 to 51 years,13 in contrast to European and US patients with PAH, typically older in the last reported registries.25 26 It is difficult to attribute this finding to different regional disease awareness or solely to different healthcare access and healthcare systems.13 We found a higher proportion of female patients, similar to other studies conducted in Latin America13 14 27–30 and the rest of the world.31 Furthermore, the most common type of PAH reported in our study was APAH, similar to previous studies in Brazil27 29 and Mexico.29
Patients in our survey were most frequently classified as WHO FC I–II, representing mild to moderate functional limitation of disease, with 21% having more severe FC III–IV disease. Other studies in Latin America have reported a similar or higher prevalence of FC III–IV disease, in up to 70% of patients in one study.13 30 32 33 This may be due to differences in the time of FC assessment as previous studies have reported changes in FC over the course of the disease, with 27% of patients within the REVEAL registry classified as FC III at enrolment reported to have improved FC at 4-month follow-up.34
A high symptomatic burden was reported by patients, with symptoms of fatigue and dyspnoea most frequently experienced. The number of symptoms experienced and the proportion of patients reporting at least one severe symptom increased with higher WHO FC, indicating a greater symptomatic burden with worsening disease severity. Kappa analysis revealed a minimal-to-weak alignment between physician and patient reports of the presence and severity of symptoms. This finding emphasises the importance of regular assessment using patient-reported outcome tools in clinical practice to enhance patient–physician communication of symptoms. This disconnect should be investigated further to help understand the full impact of symptoms on patients with PAH to optimise treatment and management of their disease.
Despite currently being recognised as the gold standard for diagnosis of PAH,3–5 a low proportion of patients were reported to have undergone RHC. This varied across countries and management setting. This may be due to lack of knowledge or training, cost or the invasive nature of the procedure.35 This study was undertaken during the coronavirus pandemic which reportedly delayed and reduced the number of RHC procedures performed.36 As diagnosis via RHC is important to a establish prognosis and avoid misdiagnosis,35 it is crucial to encourage its utilisation as standard practice. It is interesting to notice the significantly higher proportion of patients undergoing RHC at reference centre; this finding highlights the need for specialised centres for optimising PAH diagnosis and management as suggested in current guidelines.3 4
In terms of HRQoL, a mean EQ-5D VAS score of 67.0 was observed, and utility scores ranged from 0.6 to 0.7 across countries. Patient-reported HRQoL was poorer for those within higher WHO FC groups, a pattern seen across countries. These scores were notably below age-matched population norms reported in Colombia (VAS: 81.5, index: 0.9)37 and the USA (VAS: 75.9, index: 0.8),38 and were comparable with index scores of patients with other chronic conditions such as heart failure (0.7) and chronic obstructive pulmonary disease (0.6–0.7).39 This demonstrates the high patient HRQoL burden of PAH and highlights the need for regular HRQoL assessment through the course of the disease.
Our survey found that less than one-third of patients underwent a simplified risk assessment in the year prior to the survey date. There are few existing studies investigating real-world usage of risk assessment tools, including one US study which also found that a low proportion of physicians (59%) used risk assessment tools in their management of PAH.40 Guidelines strongly recommend regular risk assessment to measure disease progression and determine the most appropriate treatment approach.3–5 This finding represents an opportunity for education regarding the benefits of a regular formalised risk assessment strategy to ensure patients are receiving the optimal treatment for their condition and identify any barriers to testing.
The proportion of patients receiving combination therapy was low and varied significantly across countries. A similarly low uptake of combination therapy was reported in the Mexican pulmonary hypertension registry (RENEHAP) with 24% prescribed dual and 2% prescribed triple-combination therapy.29 In Brazil, only 28% of patients included in the RESPHIRAR study were reported to receive combination therapy.41 The stark country differences in combination therapy prescribing may reflect country healthcare systems, with barriers such as limited drug availability, low government reimbursement, geographical challenges and local recommendations for monotherapy reported for Mexico and Brazil.17 In addition, the relatively low proportion of physicians who were affiliated with a PAH specialist centre in Brazil in particular (18%) and also in Mexico (41%) may help explain the low use of combination therapy in these countries. The benefits of treatment in a PAH specialist centre compared with local centres have previously been described and include the greater relevant experience of healthcare professionals, the greater chance of an association with patient groups and more likely input from a multidisciplinary team.42 This also highlights the importance of specialist referral and greater patient access to PAH-accredited centres for the optimal treatment of PAH. A potential justification for the differences in combination treatment may be related to the follow-up time (or evolution) since diagnosis. We found that patients with a longer recorded time since PAH diagnosis were more frequently prescribed combination therapy. Further research is needed to identify any barriers to prescribing PAH treatment and the clinical impact of these treatment patterns.
Limitations
This study has a number of limitations that reflect its real-world methodology.43 The DSP is not based on a true random sample of physicians or patients. Physicians provided data for a consecutive series of patients to avoid selection bias. Data were collected at the time of each patient’s most recent consultation and physicians had access to patient clinical records for retrospective extraction of historical data, which was expected to reduce the likelihood of recall bias. While minimal inclusion criteria governed the selection of the participating physicians, participation was influenced by willingness to complete the survey. The population of included physicians based in PAH-accredited centres compared with general care settings differed among countries surveyed, ranging from 18% in Brazil to 71% in Argentina. Although this is a reflection of the real-world nature of this study, it may potentially limit the extent of direct country-to-country comparisons.
One important limitation of this study is that data were collected during the COVID-19 pandemic, which may have had implications on many aspects of the study, including patient management and sampling, as well as patient QoL and well-being.
Finally, this DSP survey consisted of patients with a physician-confirmed diagnosis of PAH, meaning that diagnosis via RHC was not required for inclusion in the survey.
Conclusions
Our study demonstrated a different PAH scenario in Latin America with high variability of diagnosis and treatment strategies across the different countries. Furthermore, the differences between patients and physicians’ perception of disease severity, the low use of appropriate diagnostic approach and the low proportion of patients receiving combination therapy evidenced an urgent need for establishing continuous medical education programmes in the region as a way to improve PAH care in the region. Further research is needed to identify other barriers to prescribing PAH-targeted therapies and the clinical impact of these treatment patterns.
Data availability statement
Data are available upon reasonable request. All data, that is, methodology, materials, data and data analysis, that support the findings of this survey are the intellectual property of Adelphi Real World. All requests for access should be addressed directly to MS at mark.small@adelphigroup.com. MS is an employee of Adelphi Real World.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but data collection was undertaken in compliance with EphMRA guidelines24 and as such does not require ethics committee approval. The survey was submitted to the Western Institutional Review Board (WIRB), a central institutional review board, where ethical exemption determination was granted on 6 November 2020 (WIRB work order #1-1359466-1). Participants gave informed consent to participate in the study before taking part. Using a check box, patients provided informed consent for use of their anonymised and aggregated data for research and publication in scientific journals. Data were collected so that patients and physicians could not be identified directly; all data were aggregated and de-identified before receipt.' to end of article.
Acknowledgments
Medical writing support under the guidance of the authors was provided by RSD Medical Communications on behalf of Adelphi Real World in accordance with Good Publication Practice (GPP) guidelines.43
References
Footnotes
X @mauricioorozco
Contributors All analyses were performed by Adelphi Real World. All authors were involved in the (1) conception or design, or analysis and interpretation of data; (2) drafting and revising the article; (3) providing intellectual content of critical importance to the work described and (4) final approval of the version to be published, and therefore meet the criteria for authorship in accordance with the International Committee of Medical Journal Editors guidelines.44 In addition, all named authors take responsibility for the integrity of the work as a whole and have given their approval for this version to be published. A steering committee of Latin American-based physicians provided support in the development of the study. MS is the guarantor.
Funding Janssen Pharmaceuticals did not influence the original survey through either contribution to the design of questionnaires or data collection. The analysis described here used data from the Adelphi Real World PAH DSP. The DSP is a wholly owned Adelphi Real World product. Janssen Pharmaceuticals is one of multiple subscribers to the DSP. Publication of survey results was not contingent on the subscriber's approval or censorship of the manuscript. Janssen Pharmaceuticals participated in the interpretation of the data, review and approval of this manuscript.
Competing interests TPi is an employee of Janssen and is a Janssen shareholder. MS and JH are employees of Adelphi Real World. MO-L, RS, IMB, JLHO, AL, GM, AR, AV and TPu received consulting fees from Janssen.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.