Article Text

Abstract
Introduction Prone positioning with head rotation can influence cerebral haemodynamics, potentially affecting cerebral perfusion and oxygenation. Elderly patients with impaired brain perfusion and oxygenation are at an increased risk of developing postoperative delirium (POD). Despite this, few studies have explored whether head orientation during prone positioning contributes to POD in older adults, an aspect often overlooked by clinicians. This study aimed to evaluate the impact of head orientation during prone positioning on the incidence of POD in elderly patients undergoing thoracolumbar spine surgery.
Methods and analysis This study is a single-centre, randomised, single-blind trial, with the assessors blinded to the intraoperative head position. Eligible participants are patients aged ≥65 years undergoing elective thoracolumbar spine surgery. A total of 500 patients will be randomly assigned to either the prone position with the head centred, or the prone position with the head deviated. The primary outcome is the incidence of POD, measured using the 3 min Diagnostic Interview for Confusion Assessment Method (3D-CAM) until postoperative day 5. Secondary outcomes include the severity of POD assessed by the Memorial Delirium Assessment Scale (MDAS), postoperative cognitive impairment evaluated using the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA), intraoperative regional cerebral oxygen saturation (rSO2), changes in vertebrobasilar artery and middle cerebral artery haemodynamics, and plasma levels of calcium channel-binding protein S100 subunit beta (S100B) and neuron-specific enolase (NSE).
Ethics and dissemination Ethical approval was obtained from Yancheng No. 1 People’s Hospital Ethics Examination Committee (2023-K-120–01). The findings will be disseminated through presentations at annual conferences and publications in scientific journals.
Trial registration number ChiCTR2300078839.
- Delirium & cognitive disorders
- Posture
- Thoracic surgery
- Clinical Trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study design is a randomised controlled trial to investigate the potential effects of head rotation on postoperative delirium with a relatively large sample size.
The study does not account for graded angles of head rotation.
It does not differentiate between left and right head deviations.
The single-centre design may limit the generalisability of the findings.
Introduction
Postoperative delirium (POD) is an acute, fluctuating neuropsychiatric syndrome characterised by disturbances in attention, awareness and cognition, typically manifesting within 5 days postsurgery. It is the most common postoperative complication in older adults.1 Recent meta-analyses report that the incidence of POD in elderly patients undergoing spinal surgery ranges from 3.8 to 40.4%, often associated with adverse clinical outcomes.2
Emerging evidence suggests that cerebral hypoperfusion, influenced by cerebral haemodynamics, plays a crucial role in the pathogenesis of POD. Significant reductions in regional cerebral blood flow have been observed in patients with delirium, affecting both cortical and subcortical regions, with improvements noted on resolution of delirium.3 Inadequate cerebral perfusion pressure has also been linked to a higher risk of POD following lung transplantation.4 Additionally, intraoperative decreases in regional cerebral oxygen saturation (rSO2) have been associated with POD during thoracotomy and endovascular procedures.5 6 Furthermore, reduced mean flow velocity (MFV) in the middle cerebral artery has been correlated with cognitive impairment and delirium in non-surgical populations.7 8 These findings highlight the importance of monitoring perioperative factors that contribute to cerebral hypoperfusion.
In thoracolumbar spine surgeries, head positioning—whether neutral or with lateral deviation—is typically based on clinical considerations. However, studies suggest that head rotation may affect cerebral haemodynamics. For instance, contralateral cervical rotation in supine-conscious volunteers has been shown to reduce vertebral artery flow in the extracranial segment.9 10 Similarly, intracranial vertebral artery blood flow velocities are significantly reduced with contralateral head rotation in prone, young volunteers.11 Under general anaesthesia in the prone position, head rotation of approximately 80° to the right has been observed to reduce MFV by ~10% in healthy young volunteers.12 Despite these observations, the potential impact of head orientation in the prone position on POD, through its effect on cerebral haemodynamics and oxygenation, remains unclear. Based on existing literature, we hypothesise that maintaining a neutral cervical spine position will result in a lower incidence of POD compared with a deviated position.
Epidemiological studies on POD have seldom considered the influence of head orientation during spinal surgery, and no research has specifically examined the effects of head orientation in the prone position on POD in older adults. Thus, the primary aim of this study is to assess the impact of head direction during prone positioning on the incidence of POD in elderly patients undergoing thoracolumbar spine surgery. Our secondary aim is to investigate the effects of head direction on cerebral haemodynamics and oxygenation during prone positioning.
Methods and analysis
Study design
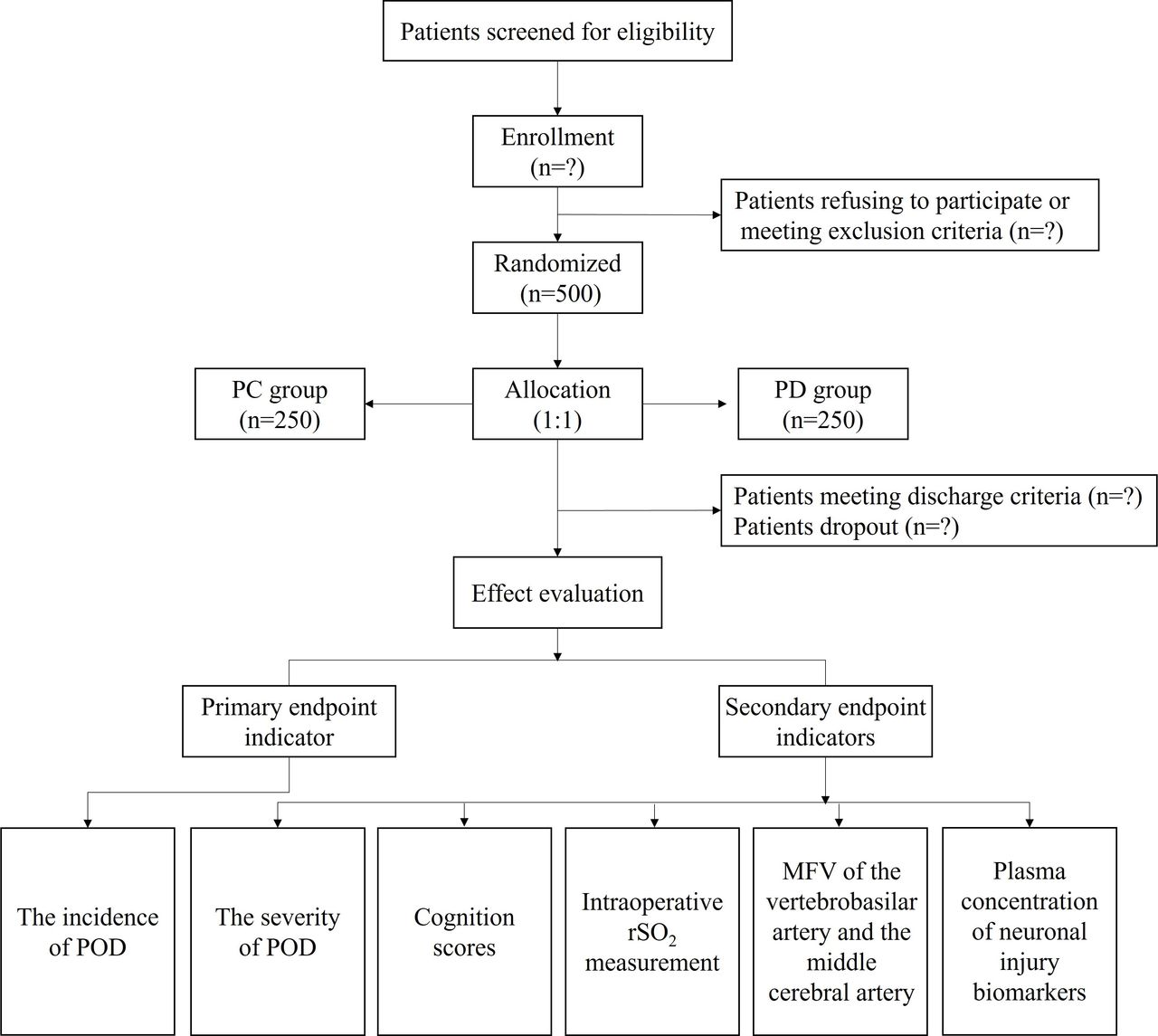
This single-centre, single-blind, randomised controlled trial aims to assess whether maintaining a neutral cervical spine position reduces the incidence of POD compared with a deviated position in older adults undergoing thoracolumbar spine surgeries. The trial design and follow-up process are detailed in figure 1 and table 1. The study will be conducted at the First People’s Hospital of Yancheng, Yancheng, China. Assessors will undergo standardised training, and the protocol will adhere to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines (see online supplemental additional file 1).
Supplemental material

{kind=link}
Study flow chart. MFV: mean flow velocity; PC: prone with the head centred; PD: prone with the head deviated; POD: postoperative delirium; rSO2: regional cerebral oxygen saturation.
Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) schedule for enrollment, interventions and assessments
Randomisation and blinding
This trial design is single-blinded, with the attending anaesthetist collecting intraoperative data and not blinded to group assignments. Patients will be randomised into either the neutral cervical spine position (PC) group or the deviated position (PD) group using a computer-generated randomisation table. Group assignments will be concealed in opaque envelopes, which will be opened intraoperatively. The allocation ratio is 1:1, and assessors responsible for preoperative and postoperative evaluations will be blinded to the intraoperative head orientation.
Patients and recruitment
A total of 500 patients meeting the inclusion criteria will be enrolled from 20 December 2023 to 31 December 2025. Participants will receive written information about the study (see online supplemental additional file 2), and written informed consent will be obtained the day prior to surgery.
Supplemental material
Eligibility
Inclusion criteria
Age ≥65 years.
American Society of Anesthesiologists (ASA) physical status classes II–III.
Mini-Mental State Examination (MMSE) score >23 points, assessed 1 day preoperatively.
Expected duration of surgery >2 hours.
Exclusion criteria
Cervical spine trauma.
Restricted head positioning.
Cervicogenic dizziness and vertigo.
Central nervous system disorders with clinical manifestations.
Communication impairments.
Psychiatric disorders.
Discharge criteria
Duration of surgery <2 hours.
Severe adverse events (AEs), such as anaphylaxis or intraoperative blood loss >800 mL.
Protocol deviations requiring intervention.
Interventions
Vital signs, including electrocardiography (ECG), oxygen saturation and invasive arterial blood pressure, will be recorded prior to anaesthesia induction. Anaesthesia will be induced with dexamethasone (10 mg), remimazolam tosylate (0.05–0.1 mg/kg), 1% propofol (1–1.5 mg/kg), fentanyl (0.1–0.15 µg/kg) and cis-atracurium (0.2 mg/kg). During the transition from supine to prone positioning, the head will be positioned according to the assigned group. Anaesthesia maintenance will involve 1–1.5% sevoflurane inhalation and continuous intravenous remifentanil infusion (0.1 µg/kg/min) until the completion of the surgery. Fentanyl and cis-atracurium will be administered as needed. Postoperatively, patients will be transferred to the postanaesthesia care unit (PACU) for extubation and observation until fully awake. Tropisetron hydrochloride (10 mg) and flurbiprofen axetil (50 mg) will be administered intravenously 15 min before surgery. Postoperative analgesia for 48 hours will include butorphanol tartrate injection (8–10 mg) and tropisetron hydrochloride (10 mg) via an analgesic pump.
Principles of intraoperative anaesthesia management include:
Bispectral index (BIS) value: 45–60
End-tidal carbon dioxide (PETCO2): 40–55 mm Hg
Body temperature: 36–37.5℃
Haemodynamic stability assisted by vasoactive drugs (mean arterial pressure (MAP) changes within 10% over 5 min)
Pulse pressure variation (PPV) <10%
Acid–base and electrolyte homeostasis.
Outcome measures
Primary outcome measure
The primary outcome is the incidence of POD within 5 days postsurgery, assessed using the 3 min Diagnostic Interview for Confusion Assessment Method (3D-CAM), conducted two times per day (08:00–10:00 and 18:00–20:00).13
Secondary outcome measures
Secondary outcomes include the severity of delirium, perioperative cognitive changes, cerebral oxygen saturation, cerebral haemodynamics and markers of neuronal injury. The severity of POD will be assessed using the Memorial Delirium Assessment Scale (MDAS) together with the evaluation of 3D-CAM.14 Cognitive function will be evaluated perioperatively using the MMSE and Montreal Cognitive Assessment (MoCA) 1 day preoperatively and daily for 5 days postoperatively.15 Baseline rSO2 will be calculated by averaging the values within 2 min before anaesthesia induction (T0). Intraoperative rSO2 values will be continuously recorded using a cerebral oximeter at the following time points: T1 (60 min after turning over), T2 (90 min after turning over), T3 (2 hours after turning over), T4 (5 min before surgery ends) and T5 (before leaving the PACU). Haemodynamic parameters of the vertebrobasilar and middle cerebral arteries will be quantified using transcranial Doppler ultrasound at T1–T5. Serum concentrations of S100 calcium-binding protein B (S100B) and neuron-specific enolase (NSE) will be determined using ELISA kits, with blood samples collected at T0 and 1 day postoperatively.
Data collection
Preoperative assessments
Preoperative assessments will be conducted by trained assessors 1 day before surgery and will include:
General data: age, sex, education level, body mass index (BMI), ASA classification and baseline blood pressure.
Medical history: major cardiovascular and cerebrovascular diseases (hypertension, diabetes, coronary heart disease and stroke).
Key laboratory results: complete blood count, coagulation profile, atherogenic index of plasma (AIP), and serum concentrations of S100B and NSE.
Cognitive function: assessed using MMSE and MoCA.
Pain assessment: evaluated using the Visual Analogue Scale (VAS).
Sleep quality: assessed using the Pittsburgh Sleep Quality Index (PSQI).
Anaesthesia, surgery and postoperative care
Detailed records of all perioperative interventions, including the duration in the prone position, use of vasoactive medications and anticholinergics, and vital signs, will be maintained for post hoc analysis. Special attention will be given to the intraoperative rSO2 values and haemodynamic parameters of the vertebrobasilar and middle cerebral arteries, recorded at specified time points. Blood gas analysis will be performed hourly.
Postoperative assessments
Incidence and severity of delirium: assessed using 3D-CAM (incidence) and MDAS (severity).
Serum concentrations of S100B and NSE: measured on postoperative day 1.
Blood pressure: monitored two times per day.
Cognitive function: evaluated using MMSE and MoCA.
Pain levels: assessed using VAS.
Sleep quality: evaluated using PSQI.
Complications and mortality: recorded as part of the study follow-up.
Sample size
Sample size calculations were performed using PASS (V.15.0.5). Preliminary experiments involving 32 patients (8 in the PC group and 24 in the PD group) indicated that 1 in the PC group and 6 in the PD group were diagnosed with POD. To achieve a power of 90% with a two-sided significance level of 0.05, the required sample size was calculated to be 200 patients per group. To account for an anticipated 20% loss to follow-up, a total of 500 patients were required. A mid-term analysis will be conducted once 50% of the target sample size is reached, with adjustments made based on the observed incidence of POD.
Data analysis
Statistical analyses will be conducted using SPSS V.20.0. Data will be presented as mean±SD for normally distributed data and median (IQR) for non-normally distributed data. Comparisons will be made using independent-sample t-tests for normally distributed data and Mann-Whitney U tests for non-normally distributed data. Categorical data will be expressed as numbers or percentages and analysed using Fisher’s exact test or χ2 test. Univariate repeated measures analysis of variance (ANOVA) will be used for intragroup comparisons, with post hoc tests and Bonferroni correction applied to control for Type I errors. A Mantel-Haenszel test, stratified by potential influencing factors such as age (youngest-old (65–74 years), middle-old (75–84 years) and oldest-old (>85 years)), AIP, gender (male and female) and head deviation (left or right), will be used to compare the risk of POD between groups. Statistical significance will be set at p<0.05.
Data monitoring
The Data Monitoring Committee (DMC) will consist of an independent researcher responsible for data collection and classification, as well as a statistician. The DMC will focus solely on data monitoring without involvement in other aspects of the study. The DMC will ensure data completeness and accuracy, and assess the overall progress of the trial. On completion, the original data, final dataset and outcomes will be submitted to the Scientific Research Management Committee.
Safety evaluation
All AEs associated with head rotation will be closely monitored. AEs include hypotension, significant cardiac arrhythmias, pneumothorax, significant disability or incapacity, cerebrovascular accidents and death. Researchers will conduct daily patient visits until discharge and meticulously record any AEs. If an AE occurs, the trial will be suspended immediately for investigation, and appropriate actions will be taken based on the findings.
Discussion
POD is a common and serious complication in elderly patients, significantly affecting postoperative recovery. In-hospital mortality was considerably higher among individuals with delirium (7.2%) compared with those without (0.9%). Additionally, postoperative 30-day mortality was also notably greater in patients with delirium (5.7%) than in those without (1.8%).16 Thus, understanding and preventing POD is crucial for improving patient outcomes and recovery.
Reduced cerebral perfusion has been linked to POD,4 17 18 with key markers for assessing cerebral perfusion, including MFV measured by transcranial Doppler and rSO₂.19 Previous studies have reported that MFV and intracranial vertebral artery blood flow velocities decrease during head rotation in the prone position among young volunteers.11 12However, a prospective controlled study found no significant difference in rSO₂ between neutral head positions and rotations to the right or left.20 This study did not focus on elderly patients, and the short duration of head positioning (<30 min) may limit its applicability. Furthermore, rSO₂ measurements were obtained by adjusting pressure sensors during head positioning, which may have affected results. Our study addresses these limitations by using a Mayfield headrest in the prone position, which mitigates pressure build-up on the forehead during cervical rotation. Despite a reported 10% decrease in MFV and compromised jugular venous return during rotation,20 the impact on cerebral perfusion pressure and autoregulation remains unclear. Further research is needed to clarify whether head rotation affects cerebral perfusion and oxygenation, and subsequently influences the incidence of POD.
Atherosclerosis, prevalent among older adults, is often assessed using the AIP, with higher values indicating more severe atherosclerosis and a greater impact on blood flow.21 Notably, both carotid and vertebral arteriosclerosis are manifestations of large-artery atherosclerosis. Research suggests that the left vertebral artery (LVA) is more susceptible to atherosclerosis than the right vertebral artery (RVA) due to higher blood flow velocity and pressure.22 A prior study reported that in healthy adults, approximately 50% have a dominant LVA, 25% have a dominant RVA and the remaining 25% have vertebral arteries of similar sizes.23 Likewise, in a study of 1414 stroke-free participants with a mean age of ≥45 years, plaques were found in both carotid arteries in 85% of cases, with a higher prevalence in the left carotid artery (67%) compared with the right (33%).24 These findings highlight the notable asymmetry between the left and right vessels. Our preliminary experiments did not show a significant effect of head lateralisation on POD. Future analyses will stratify data based on AIP and head deviation to explore these factors further. Additionally, sex differences in vertebral artery blood flow during head rotation have been reported,11 with mild reductions in males but not females during ipsilateral rotation.11 These sex differences will also be considered in our stratified analyses.
This study has two main limitations. First, all participants are recruited from a single centre, which may limit the generalisability of the findings. Second, the study does not include graded angles for head direction, which would have complicated the experimental design.
Despite these limitations, we anticipate that this trial will provide valuable insights into whether maintaining a neutral cervical spine position reduces the incidence of POD compared with a deviated position.
Trial status
To date, 32 participants have been enrolled in the study; however, participant recruitment is still ongoing at the time of submission. This trial is scheduled to be conducted from 20 December 2023 to 31 December 2025.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Footnotes
JZ, YC and YC are joint first authors.
JZ, YC and YC contributed equally.
Contributors BQ took responsibility for the integrity of the work as a whole and served as the primary investigator. JZ, YC, YC, KN, FL and BQ were involved in the study’s design. JZ, KN, FL and BQ drafted the manuscript. YC, FL and HM contributed to the calculation of the sample size and provided statistical consultation. QC, FW, XC and ZX developed the case report forms and conducted a preliminary trial. JZ, YC, HM, QC, FW, ZX, KN, FL and BQ were responsible for conducting the clinical trials. All authors contributed to revising the manuscript for important intellectual content. BQ acted as guarantor.
Funding This work was supported by Yancheng Fundamental Research Program (YCBK202208) and The First Affiliated Hospital of Jiangsu Vocational College of Medicine Basic Research Program (QN2022001).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.