Article Text

Abstract
Background The persistent trigeminal artery (PTA) is an adult carotid-basilar anastomosis with debated pathologic aspects, such as its association with brain aneurysms. True trigeminal artery aneurysms are rare vascular anomalies, reported in a few case reports.
Objective To report our experience with a ruptured trigeminal artery aneurysm and to provide a systematic review of the literature in order to analyse potential links between the anatomic configuration of the PTA and PTA aneurysm (PTAA) type, and implications of each PTAA type for the diagnostic and therapeutic approach.
Methods We reviewed the medical literature on trigeminal artery aneurysms according to the PRISMA guidelines. Population characteristics, aneurysms features, and PTA type and side were assessed.
Results 40 previously published cases of PTAAs were included in the analysis. The mean age of subjects was 55 years, with a strong female predominance (77%). Four PTAAs were accidentally discovered, while 16 caused compressive symptoms and 20 were ruptured. Successful endovascular treatment was performed in 62% of cases.
Conclusions PTAAs are rare vascular anomalies, underdiagnosed in the presence of a trigemino-cavernous fistula. Parent vessel occlusion seems to be the best therapeutic option for ruptured or symptomatic unruptured PTAAs in Saltzman type II and III PTAs. Patency of the parent vessel is the main target in Saltzman type I PTA.
- aneurysm
- artery
- congenital
- fistula
- blood pressure
Statistics from Altmetric.com
Introduction
The persistent trigeminal artery (PTA) derives from the primitive trigeminal artery. It develops in the embryo with the trigeminal ganglion, and it connects precursors of cavernous internal carotid arteries (ICAs) and basilar artery (BA), at the 3–4 mm embryonic stage.1 2 At the 7–12 mm stage, it regresses completely as a small cavernous branch of the ICA, called the lateral artery of the clivus, or in some rare cases its incomplete regression results in the intracavernous origin of a cerebellar artery or the basilar origin of the middle meningeal artery. Why PTA persists into the adult stage is not completely clear.3
Several studies have analysed PTA prevalence, anatomical characteristics, and its association with cerebral aneurysms and vascular malformations, since the first autoptic and angiographic description was made. However, only few cases of proper primitive trigeminal artery aneurysms (PTAAs) have been reported (online supplementary table 1), with consequent lack of consistent data available. The aim of this paper is to provide a review about PTAAs in order to analyze potential links between the anatomic configuration of the PTA and PTAA type and implications of each PTAA type for the diagnostic and therapeutic approach.
Supplemental material
Materials and methods
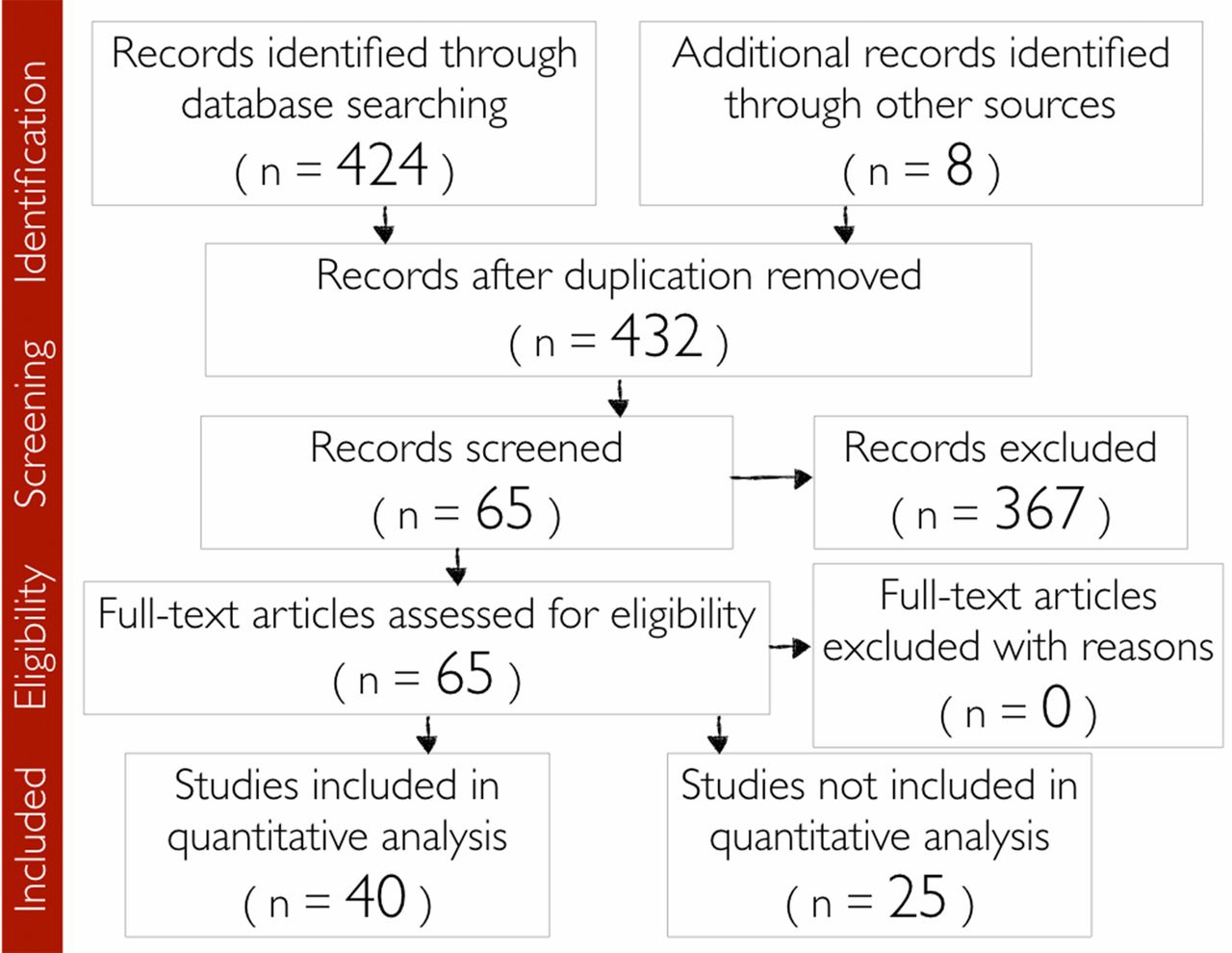
We reviewed the medical literature about PTAAs up to March 2019, searching on PubMed and combining search terms for ruptured and unruptured PTAAs. All studies reporting an aneurysm of the trigeminal artery were included in online supplementary table 1 and used for the quantitative analysis (table 1). Moreover, 32 trigemino-cavernous (T-C) fistulas with an unidentified aneurysm were found and reviewed in order to study their pathophysiology and the possible presence of an undiagnosed aneurysm (online supplementary table 2). Evaluation was performed according to the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISMA) statement, including methods of publication search, eligibility, data collection, extraction, analysis, and preparation of the systematic review report (figure 1)
Supplemental material

PRISMA flow chart.
Trigeminal artery aneurysms. Results of the systematic review.
Cavernous PTA and Salas classification
The PTA originates from the cavernous portion of the ICA and its course is usually tortuous.4 Within the cavernous sinus it is located superior to the oculomotor, trochlear, and abducens nerves and medial to the ophthalmic branch of the trigeminal nerve and ganglion.
Salas et al described two types of PTA based on their relationships to the abducens nerve: lateral or petrous, and medial or sphenoid (figure 2). The petrous type arises from the posterolateral aspect of the cavernous ICA and runs under the VI cranial nerve. It pierces the dura mater just medial to the sensory root of the trigeminal nerve. The sphenoid type arises from the posteromedial aspect of the cavernous ICA, than pierces the dura over the dorsum sellae and courses medial to the abducens nerve.5

Salas classification: petrous and sphenoid persistent trigeminal artery. Drawing of our case: a lateral petrous persistent trigeminal artery with a cavernous aneurysm.
Cisternal PTA and Saltzman classification
Generally, the cisternal segment of the PTA is more regular than the cavernous one. It inserts into the BA between the anterior-inferior cerebellar artery and the superior cerebellar artery (SCA).
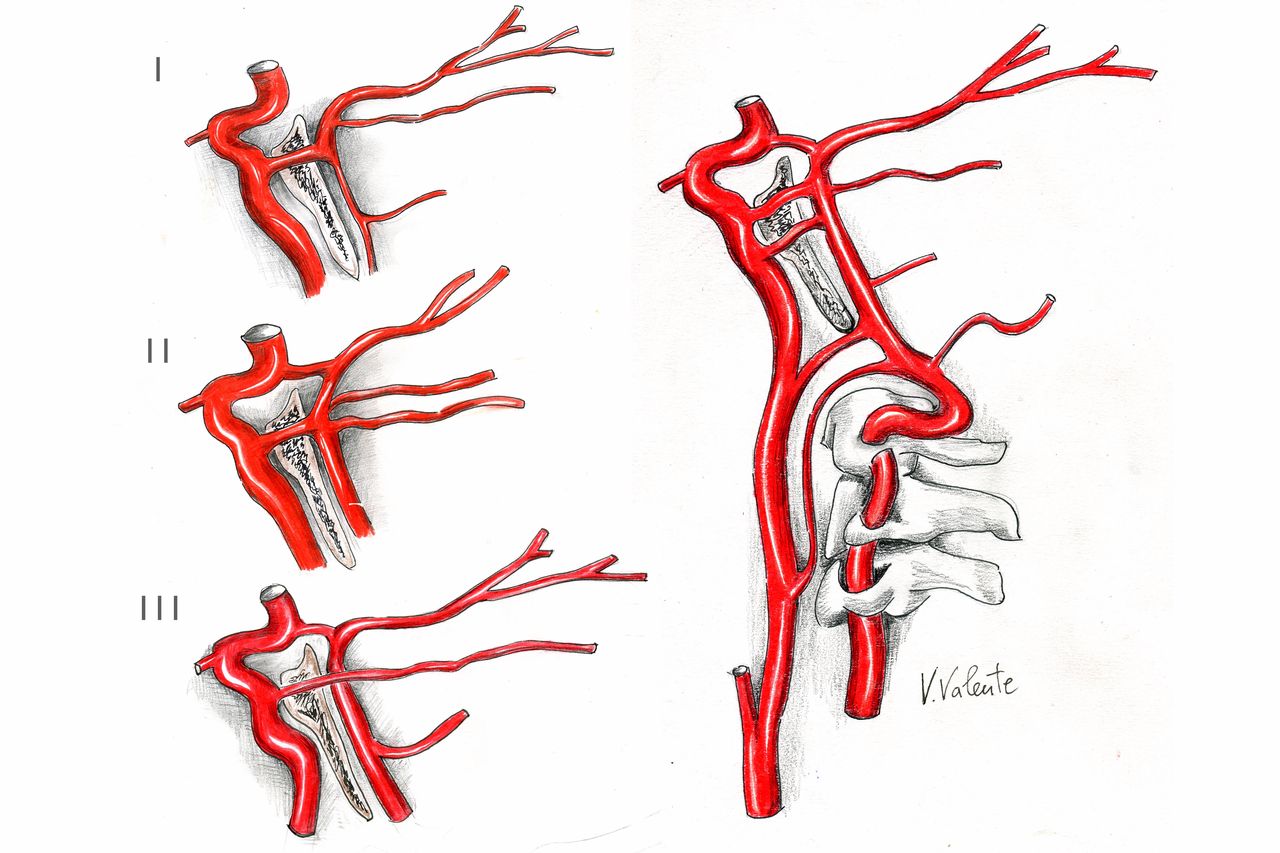
There is a haemodynamic balance between the PTA and the vertebrobasilar system to supply the posterior fossa. According to Saltzman et al,6 PTA can be classified based on the configuration of the posterior circulation and the contribution of the proximal vertebrobasilar system. This angiographic classification initially divided PTA in two main types. In Saltzman type I, the PTA is the main supply to the distal BA, posterior cerebral artery, and SCA territories, generally because the BA proximal to the insertion of the PTA is hypoplastic and the posterior communicating artery is absent. In Saltzman type II, the PTA mainly supplies the SCA territory, because the posterior cerebral arteries receive their blood supply predominantly from patent posterior communicating arteries. Some Saltzman variants have been identified as Saltzman type III7–9; they are an uncommon junction of the PTA with one of the cerebellar arteries originating from the BA (figure 3).

Drawing of the persistent primitive carotid-basilar anastomoses (proatlantal, hypoglossal, otic, and trigeminal arteries). Saltzman classification: type I with hypoplastic mid-basilar artery proximal to insertion of the persistent trigeminal artery (PTA) and aplasic or hypoplasic posterior communicating arteries; type II with well formed midbrain and the posterior communicating arteries present; type III which is a cerebellar artery arising from the PTA.
Case presentation
A 61-year-old woman presented with a 2-year history of progressive, right-side, audible bruit, exophthalmos, conjunctival congestion, and diplopia. She had no history of trauma and no family history of connective tissue disorder or berry aneurysm. MR angiography showed the T-C fistula involving the right cavernous sinus and the ipsilateral PTA. The patient was admitted for the endovascular treatment.
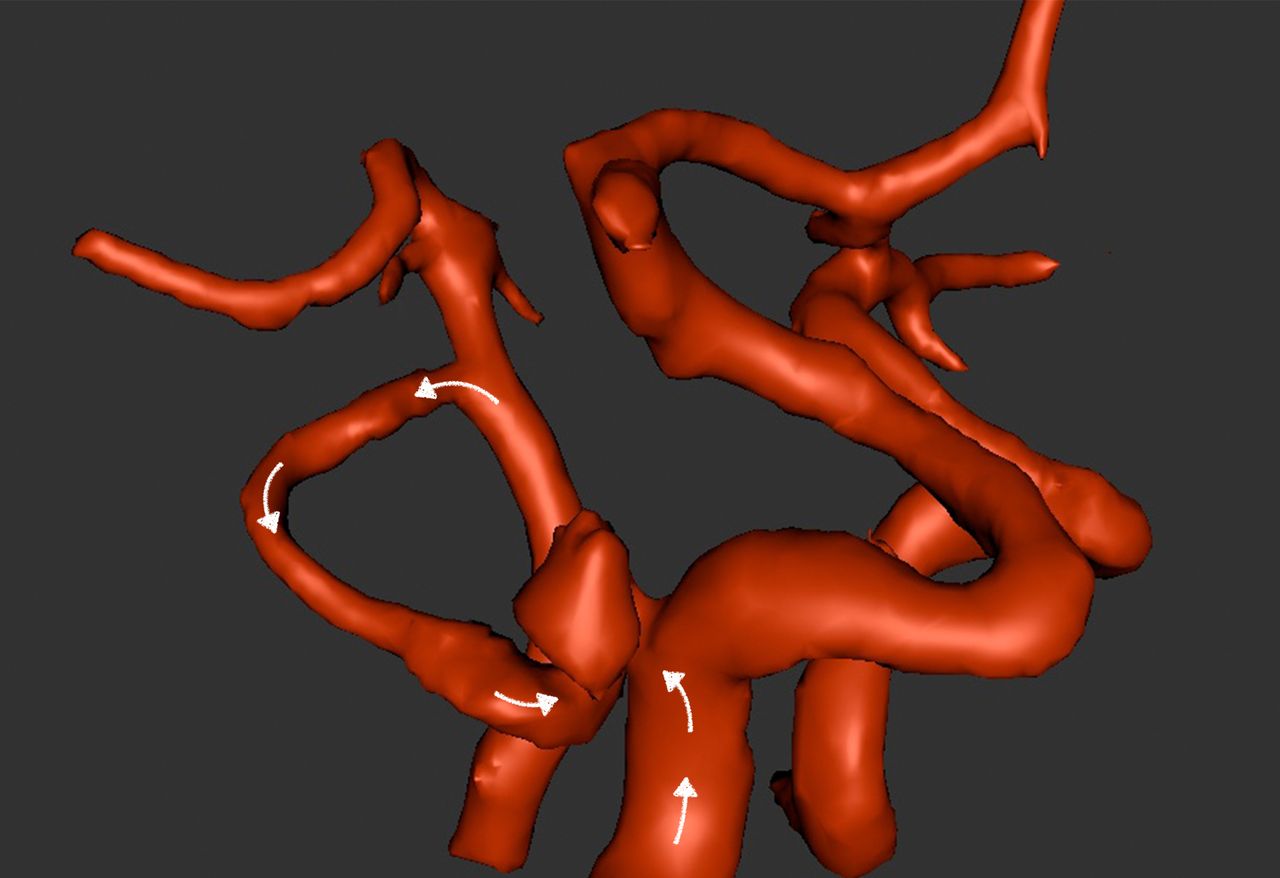
The procedure was performed under general anesthesia with bilateral transfemoral access. A Vertebral Optitorque 4F (Terumo, Tokyo, Japan) was used for the complete pretreatment evaluation. Pretreatment digital subtraction angiography (DSA) and a 3D-DSA with injection in the right ICA and right vertebral artery confirmed the T-C fistula caused by the rupture of a small cavernous saccular PTAA (figure 3; figure 4). Both the cavernous sinuses were engorged; the venous drainage involved both the dorsal ophthalmic veins and the right inferior petrous sinus (figure 5A–C).

3D reconstruction of the MR angiogram, which shows the ruptured small trigeminal artery aneurysm of the cavernous sinus. Arrows indicate the direction of the arterial flow from the internal carotid artery and from the vertebral artery, resulting in an extremely high flow shunt. Different dimensions between cisternal and cavernous segments of the persistent trigeminal artery are also evident.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
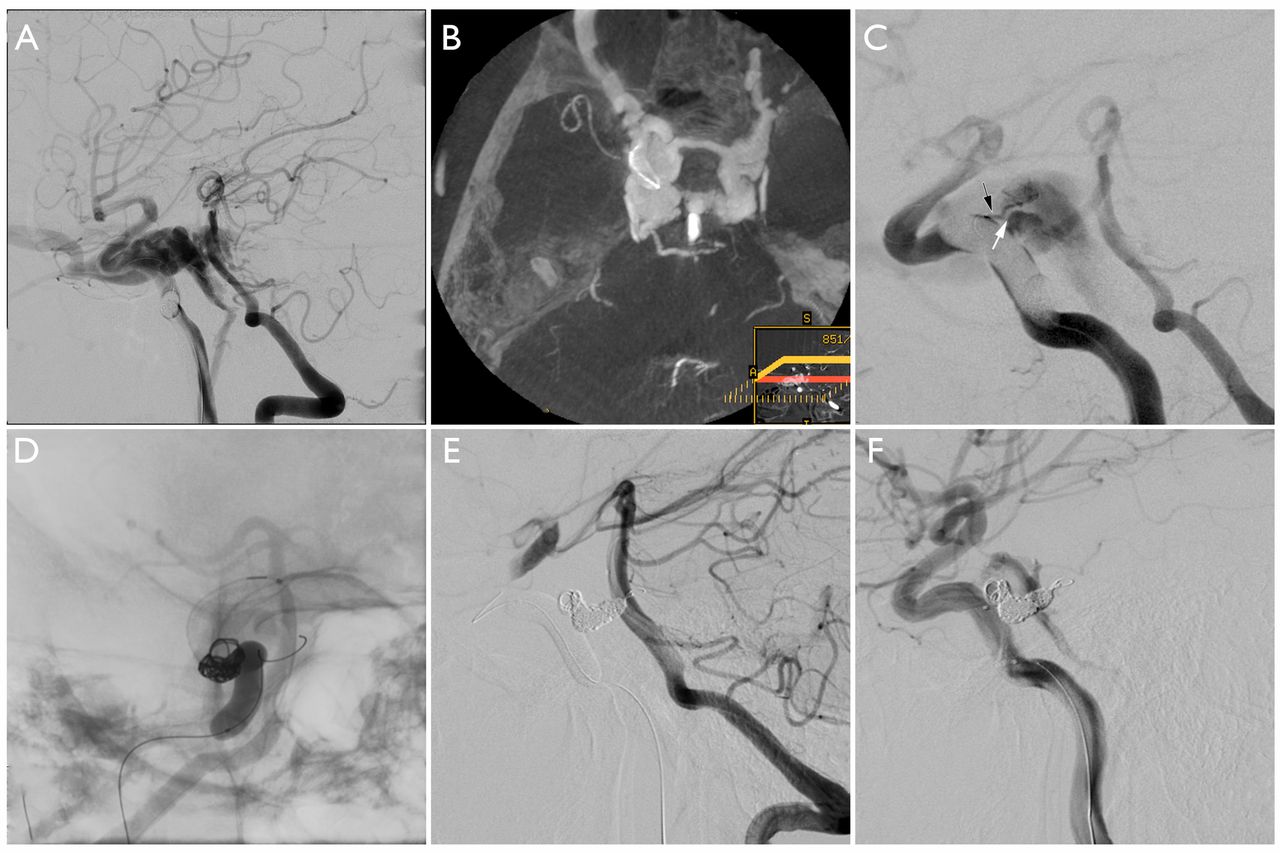
Endovascular treatment of the trigemino-cavernous (T-C) fistula. (A) Double injection in the vertebral artery (VA) and the internal carotid artery (ICA) with a balloon inflated in the petrous segment of the ICA, in order to reduce the blood flow into the fistula. (B) 3D DSA with double injection in the VA and ICA, showing the engorgement of both cavernous sinus and ophthalmic veins. (C) Angiographic run showing different origins of the persistent trigeminal artery (PTA; white arrow) and the meningohypophyseal trunk (black arrow). (D, E) Coiling of the aneurysms and the PTA from the VA, with a balloon inflated into the cavernous ICA. (F) The last control showing a residual T-C fistula with drainage into the inferior petrous sinus.
We decided to occlude the PTAA and the cavernous PTA. A balloon occlusion microcatheter HyperGlide 4×20 mm (Medtronic Neurovascular, California, USA), with a 0.14 in Asahi Chikai microwire (Asahi Intecc, Japan), was inflated into the cavernous ICA. A microcatheter Excelsior SL-10 (Stryker Neurovascular, California, USA), with a 0.14 in Asahi Chikai microwire, was positioned through the posterior circulation into the PTA and used for the coiling (figure 5D). Final DSA runs documented the occlusion of the PTA and a little residual fistula draining only into the inferior petrous sinus. Therefore we decided to stop the procedure and to wait for its probable spontaneous obliteration (figure 5E,F). At 1 month’s follow-up the symptoms had completely regressed and MR angiography confirmed the complete occlusion of the residuum.
Results
After a review of the literature 39 previously published articles about PTAAs were found; three articles were excluded from the quantitative analysis owing to a lack of full text or clinical and imaging data.10–12 The present case has been included in the analysis and reported in table 1. Among these 39 reported patients the mean age was 55 years (range 20–77 years); 31 were female (77%), nine were male (23%).
Twenty aneurysms were ruptured, presenting with subarachnoid haemorrhage (SAH) in nine patients13–21 (45%), a T-C fistula in 10 patients,22–30 and repeated epistaxis in one patient31 (5%). Eight T-C fistulas were spontaneous (40%), while just two were caused by a major or minor head trauma (10%). Twenty aneurysms were unruptured: symptomatic in 16 cases31–46 (80%), asymptomatic in four cases42 47–49 (20%).
PTAAs were localized in the cavernous segment in 30 cases (75%), in the cisternal segment in six cases (15%), and involved both segments in three cases (7%). In one case the PTAA was extradural and located in the sella turcica.
Thirty-two aneurysms were saccular (82%), while seven were fusiform (18%). Among saccular aneurysms 10 were small (31%), eight were medium (25%), 10 were large (31%), and four were giant (13%). In two cases PTAA dimensions were not reported.
In 39 cases (97%) the PTAA was associated with a petrous PTA, while in just one case (3%) with a sphenoid PTA: right side in 24 patients (60%) and left side in 16 patients (40%). PTAAs were associated with a type I PTA in 10 patients (25%), type II in 23 patients (57%), and type III in seven patients (18%), according to the Saltzman classification.
Twenty patients with ruptured PTAAs were treated: 5 of them with a neurosurgical approach, 14 with an endovascular approach. One patient with a T-C fistula refused the treatment.27
Eight patients with unruptured aneurysms were not treated. However, 11 patients underwent endovascular treatment and just one a surgical bypass.
In 14 cases, treatment did not required occlusion of the PTA.
In one case coiling of the aneurysm and the parent artery was performed, assisted with two open-cell stents deployed into the PTA in order to avoid coils prolapse into the ICA.44 No cases of PTAAs treated with flow diverters have been reported.
Mean follow-up time was 8 months and the longest follow-up was 30 months; recanalization of occluded PTAAs has never been reported.
Discussion
The frequency of brain aneurysms in patients with a PTA is controversial. Initial studies reported that 14% of patients with PTA are likely to have aneurysms,47 and subsequent reviews suggested that the prevalence of intracranial aneurysms in patients with PTA is not higher than in the general population.50 51 Proper PTAAs are extremely rare and limited data are available in the literature since only few case reports have been published (online supplementary table 1). To our knowledge this is the first review of PTAAs.
PTAAs are uncommon vascular lesions arising from the most common persistent carotid-basilar anastomosis (≃0.37%), with a strong female predominance of the PTAAs (M:F=2:7). Patients' mean age was 55 years, except for a subgroup of patients presenting with a traumatic T-C fistula, whose mean age was 27 years. In this series there is a high rate of ruptured PTAAs (50%); however, the risk of rupture cannot be estimated owing to a lack of epidemiological data about PTA and PTAAs.52
Unruptured PTAAs are rare incidental findings (21%), generally discovered in patients with SAH due to rupture of a simultaneous intracranial aneurysm. Large and giant cavernous PTAAs could be symptomatic owing to a mass effect (headache, cranial neuropathy, visual disturbances, and facial pain). Small cavernous PTAAs are generally responsible for spontaneous T-C fistula that can present with visual impairment (orbital bruit, chemosis, proptosis, diplopia, vision changes, eye pain), pulsatile tinnitus, and headache. Traumatic T-C fistulas are less frequent, but more common in young men.
Ruptured PTAAs presenting with SAH are purely cisternal small saccular aneurysms or fusiform aneurysms involving both the cavernous and cisternal segments. The SAH is associated with headache and posterior cranial fossa symptoms (vomiting and cervical rigidity), while a sentinel headache has never been reported.
Almost all reported PTAAs were associated with petrous PTA, which is probably the only ‘true’ PTA, while sphenoidal PTAAs are exceptional accidental findings. Petrous and sphenoid types have a different embryonic development, a different origin in the posterior bend of the cavernous ICA (figure 5C), and different vascular territories. The lateral PTA provides the blood supply to the hindbrain and to the trigeminal ganglion, while the medial PTA provides arterial branches to meningohypophyseal trunk territories.3 5 53–55
We speculate that the strict relation between the PTA and fixed points of the cavernous sinus could cause PTA lesions or rupture of pre-existent PTAAs; these fixed points are the anterior part of the cavernous sinus with multiple ligamentous dura-like trabeculae anchoring the ICA to the surrounding bony structures,56 and the transition point of the PTA at the level of the dural foramen.54 At these fixed points the PTA may be subject to strong shear forces and distortion.17 57
To our opinion the incidence of PTAAs in T-C fistulas is underestimated because high-flow arteriovenous shunting may have obscured underlying aneurysms.58 T-C fistula is a ‘double C-C fistula’ in which there is an arterial flow from the ICA, like a conventional C-C fistula, and an adjunctive arterial flow from the BA, particularly in type II PTAs. In reported cases19 27 58–84 (online supplementary table 2) a PTA was documented in only 10 patients, even though the presence of an underlying alteration of the PTA is the most likely scenario.
Ruptured and unruptured cavernous PTAAs have a different diagnostic approach; unruptured trigeminal aneurysms are identified with the CT or MR angiography, while in T-C fistulas DSA is always required. Runs with a high frame rate and flow controlled injections with a balloon catheter in the ICA and vertebral artery could be useful to distinguish arterial and venous structures of the fistula and to discover whether the PTA might be occluded.
Treatment of PTAAs could involve the occlusion of the aneurysm itself, of the PTA, or of the cavernous sinus with preservation of the parent artery, in some T-C fistulas. To detect the target treatment it is important to understand vascular anatomy and the haemodynamic balance between the PTA and the vertebrobasilar system. In Saltzman type I PTA, the PTA must not be sacrificed because this might result in infarction of the posterior circulation.18 In type II PTA, the vertebrobasilar system is well developed and there are the posterior communicating arteries, hence the PTA could be occluded.
Despite some initial cases in which PTAAs underwent neurosurgical treatment, the endovascular approach is the primary choice in almost all patients. Neurosurgical techniques that were used included an extracranial artery-ICA bypass,34 surgical packing of the cavernous sinus,25 carotid artery ligation,23 and clipping of the aneurysm17 or the PTA.14
Endovascular treatment may be performed by various techniques: when the PTA may not be preserved, its obliteration could be obtained with coils, when the preservation of the PTA is mandatory unassisted or assisted coiling could be used. Occlusion of the PTA with detachable balloons has never been described.
In T-C fistulas transarterial and transvenous coiling or balloon embolization of the cavernous sinus has been reported. We think that in Saltzman type II PTA, the transarterial occlusion of the cavernous segment is the aim of the treatment, while in Saltzman types I and III the transvenous occlusion of the cavernous sinus is preferred to avoid occlusion of the parent artery.
Parent vessel occlusion might be the best option also in symptomatic patients with unruptured PTA, while a conservative approach might be the best choice in asymptomatic patients.
Cisternal PTA could have collateral branches to the brainstem and the trigeminal nerve.3 54 When parent vessel occlusion is planned, we suggest that this segment is spared to avoid ischemic complications.
Study limitations
This research, however, has some limitations. Data analysis was conducted on a limited number of published case reports; they are subject to biases that may have influenced our results. The small number of unruptured asymptomatic PTAAs might be underestimated. Therefore, the rate of ruptured PTAAs (5%) is probably overestimated.
Conclusion
PTAAs are rare vascular anomalies and, in our opinion, underdiagnosed in cases of T-C fistula due to its high flow shunt. Treatment of PTAAs requires a thorough knowledge of the underlying PTA anatomy and classification. Parent vessel occlusion seems to be the best therapeutic option for ruptured or symptomatic unruptured PTAAs in Saltzman type II and III PTAs. Patency of the parent vessel is the main target in Saltzman type I PTA.
References
Footnotes
Contributors Conception and design of the work: FD. Data acquisition: FD, SM, AW, and GG. Data analysis and interpretation: FD, VV, AW, and GG. Drafting the work: FD and VV. Critical revision: CC, SM, and MB. Final approval: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.