Article Text

Abstract
Eclampsia spectrum disorders are a set of serious complications of pregnancy that commonly present after 20 weeks of gestation. There is an association between molar pregnancy, a gestational trophoblastic disease resulting from abnormal fertilisation and gametogenesis, and eclampsia spectrum disorders which can result in manifestation of pre-eclamptic symptomatology earlier than 20 weeks of gestation. We report a case of a gravida 1 para 0 in her mid 20s at 16-weeks gestation presenting with partial hydatidiform mole who developed eclampsia, haemolysis, elevated liver enzymes and low platelets syndrome and posterior reversible encephalopathy syndrome. Ultrasound findings were consistent with molar pregnancy and pathology confirmed partial molar pregnancy with triploid 69, XYY karyotype. This case highlights the early onset potential of eclampsia spectrum disorders in molar pregnancies while suggesting screening such patients for hypertensive disorders.
- Pregnancy
- Hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The term gestational trophoblastic disease encompasses premalignant and malignant conditions arising from trophoblastic cells. Premalignant disorders include complete or partial hydatidiform mole, whereas malignant disorders include invasive mole, choriocarcinoma and placental-site trophoblastic tumour.1 A complete hydatidiform mole typically results from fertilisation of an empty ovum by a single sperm that duplicates its DNA, resulting in a 46 XX karyotype. About 10% of complete moles occur when an ovum lacking chromosomes is fertilised by two sperm, resulting in a 46XY karyotype of paternal origin. Conversely, partial hydatidiform moles are triploid in nature and occur when two sperm fertilise a single ovum.1 2
Pre-eclampsia, a hypertensive disorder of pregnancy complicating 2%–8% of pregnancies, is a syndrome which presents as new-onset hypertension after 20 weeks’ gestation accompanied by proteinuria and/or evidence of maternal acute kidney injury, liver dysfunction, neurological features, haemolysis or thrombocytopenia or fetal growth restriction.3 The occurrence of haemolysis, elevated liver enzymes and low platelet count, referred to as HELLP syndrome, is considered a severe form of pre-eclampsia.4 A related severe manifestation is posterior reversible encephalopathy syndrome (PRES)—a clinico-radiological syndrome characterised by symptoms including headache, seizures, altered consciousness and visual disturbances. PRES is commonly, but not always, associated with acute hypertension.5 The symptoms of PRES vary widely with various neurologic symptoms as well as gastrointestinal symptoms such as nausea and vomiting.6 Although pre-eclampsia and HELLP syndrome rarely occur before 20 weeks of gestation, reports have suggested early occurrences of these hypertensive disorders specifically in the setting of a molar pregnancy.7–11
Case presentation
The patient is a gravida 1 para 0 female in her mid 20s at 16 weeks 5 days dated by 6 week ultrasound who presented to an outside emergency department with a 3 day history of progressive generalised abdominal worse in the epigastric region which ‘felt like someone punched me’ which radiated to her back, arms and shoulders. She has no significant risk factors for pre-eclampsia other than nulliparity. At the outside facility, the patient had multiple systolic blood pressures greater than 160 mm Hg and had a witnessed 30 s seizure which resolved with an intravenous (IV) injection of 2 mg of lorazepam and 4 g magnesium sulfate loading dose. She received a CT scan of her head which was negative for signs of mass effect or gross haemorrhage or ischaemia. She then received two doses of IV labetalol and was initiated on a magnesium sulfate infusion for seizure prophylaxis pending transfer to our institution. At the outside hospital, the patient’s laboratory work up was significant for dipstick urine protein 3+, aspartate aminotransferase (AST) 100 U/L, alanine transaminase (ALT) 57 U/L, platelet count was 169 000/uL, haemoglobin was 12.2 g/dL and her lactate dehydrogenase (LDH) was 387 U/L. On admission, the patient met criteria for eclampsia and her laboratory work up showed a trend towards HELLP (platelets 79 000/uL, AST 144 U/L, ALT 96 U/L, LDH 482 U/L, haemoglobin 8.7 g/dL). Haemolysis was defined by the decreasing haemoglobin and elevating lacate dehydrogenase. The beta human chorionic gonadotropin (HCG) level was greater than 200 000 mIU/mL. Of note, the thyroid stimulating hormone was low at <0.020 uIU/mL with a normal T4 of 1.44 ng/dL. Bedside ultrasound suggested the presence of an enlarged cystic placenta and a growth restricted fetus (estimated fetal weight 124 g, second percentile Hadlock) with heart tones in the 130 s and a biparietal diameter and head circumference less than the first percentile Hadlock. The patient and her family were counselled and the decision was made to proceed with misoprostol induction and termination of the pregnancy. After initiation of the induction, the patient developed significant vaginal bleeding and was taken to the operating room for an uncomplicated dilation and evacuation. After the procedure, the patient developed progressive visual blurring and 4+ hyperreflexia. MRI of the brain with and without contrast was obtained with findings significant for PRES. Specifically, the MRI revealed T2 high-signal lesions within the cortex of the bilateral occipital lobes (figure 1), scattered lesions within the bilateral cerebellar hemispheres, left meningeal enhancement and gyral swelling in the right parietal lobe.

MRI image demonstrating T2 high-signal lesions within the cortex of the bilateral occipital lobe (figure developed by author and retrieved from patient chart).
Neurology was consulted and recommended blood pressure control with extended-release nifedipine and initiation of levetiracetam for seizure prophylaxis. The patient did complete the 24-hour magnesium sulfate infusion for eclampsia prophylaxis. Patient’s visual symptoms stabilised and resolved, and the hyperreflexia abated. Her liver function tests, platelets and LDH also returned to normal soon thereafter. The 48-hour postprocedure beta-hCG was 79 033 mIU/mL, trending down from >200 000 mIU/mL noted prior to the procedure. The patient received contraceptive counselling to prevent pregnancy during postevacuation gestational neoplastic disease surveillance period. She was initiated on oral hormonal contraceptives.
Differential diagnosis
After the patient was transferred, epilepsy was considered briefly but ruled out due to no history of prior seizures and the seizure occurring in a setting of newly elevated blood pressure. Gestational hypertensive disease does not typically occur so early in pregnancy, but this patient had evidence of molar pregnancy (abnormal findings on ultrasound and abnormally elevated beta-HCG) which would explain the early onset. Cerebrovascular accident was on the differential but did not appear on imaging and the neurologic symptoms improved with antiepileptic medications, magnesium sulfate and blood pressure control which is more consistent with eclampsia and PRES.
Treatment
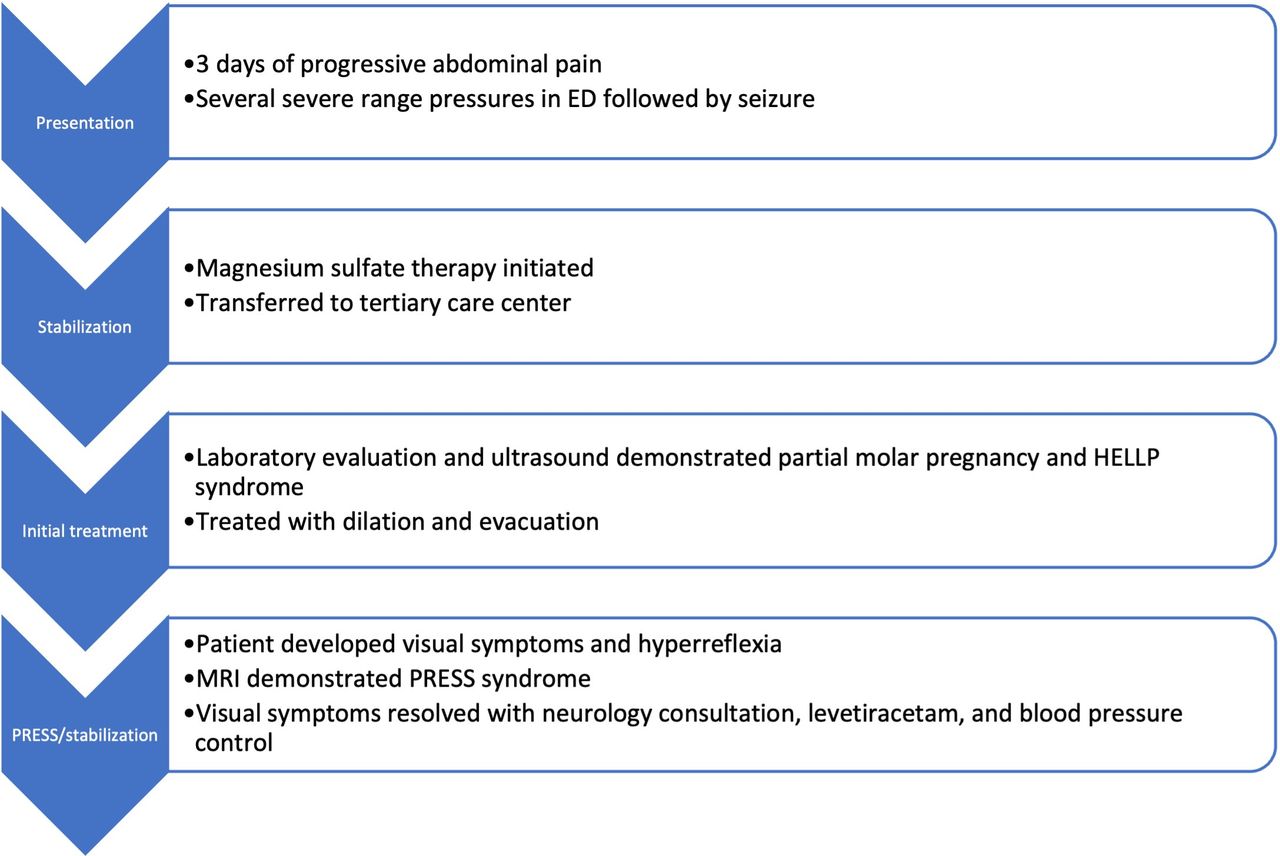
Ultimately, the source of her gestational hypertensive disease was the partial molar pregnancy which was treated with dilation and evacuation. She required stabilisation several times for the various manifestations of her pre-eclamptic disease. She was treated with IV labetalol and magnesium sulfate for maternal stabilisation during her eclamptic seizure. For stabilisation of neurologic symptoms of PRES, she was initiated on levetiracetam for seizure prophylaxis and extended-release nifedipine for blood pressure control. See figure 2 for a summary.

Treatment and stabilisation of severe pre-eclamptic disease (figure developed by author). ED, emergency department; HELLP, haemolysis, elevated liver enzymes and low platelets syndrome; PRES, posterior reversible encephalopathy syndrome.
Outcome and follow-up
The histologic pathology demonstrated the presence of chorionic villi composed of both large hydropic and smaller normal-appearing villi. The gross pathologic examination revealed a 69.3 g female fetus compatible with gestational age of approximately 14–15 weeks with caudal neurocutaneous defect with abnormal localisation of brain tissue, and overall unremarkable fetal membranes. The genetic profile of the villous tissue consisted of two sets of dispermic paternal alleles in addition to one set of maternal alleles consistent with a partial mole diagnosis. Per National Comprehensive Cancer Network (NCCN) guidelines, the patient was advised to undergo weekly beta-hCG until negative, followed by 3 weekly consecutive negative levels before spacing measurements to every 3 months for a period of 6 months. Because the patient was very complaint with follow-up, she underwent modified testing of every 2 weeks until non-pregnancy levels were achieved and then monthly for 6 months (figure 3). She became pregnant at her sixth month of non-pregnancy level surveillance and successfully delivered at term.

{kind=link}
{kind=link}
{kind=link}
Beta-HCG surveillance (figure developed by author). HCG, human chorionic gonadotropin.
Discussion
There is an association between pre-eclampsia and molar pregnancy. Of partial hydatidiform molar pregnancies, 41.9% will develop the symptoms of pre-eclampsia if left untreated.12 Although the pathophysiology of eclampsia spectrum disorders is incompletely understood and appears to be multifactorial, some evidence points to the role of increased death of trophoblasts and the maternal inflammatory response to trophoblast deportation.13–15 Additional evidence points to angiogenic factor imbalance, which becomes of interest when coupled with the observation that molar placentas produce high levels of antiangiogenic factors.16 17 Other causative agents include placental factors that trigger maternal endothelial activation. It is known that trophoblastic debris shed from the placenta into the maternal blood is associated with this condition.18 It has been demonstrated that trophoblastic debris from molar pregnancies also induces endothelial cell activation through heat-shock protein 70 (HSP70) expressed on a hydatidiform molar placenta, which may be a pathogenic signal to endothelial cells.18 This case reiterates the association between hydatidiform moles and the hypertensive disorders of pregnancy possibly supporting the theories that such disorders may share an etiologic linkage through trophoblast debris and angiogenic factor imbalance leading to endothelial damage.
Current management guidelines for molar pregnancy are primarily focused on evacuation of the pregnancy and rigorous beta-HCG monitoring to prevent the progression to gestational neoplasia.2 19 20 Our case is a demonstration that patients with molar pregnancies are also in danger from the morbidity of severe manifestations of pre-eclampsia, as our patient developed eclampsia, HELLP and PRES before 20 weeks’ gestation. Therefore, patients with molar pregnancy with elevated blood pressures and/or neurologic symptoms such as new-onset vision changes should be evaluated for pre-eclampsia, HELLP and PRES with a complete blood count, liver function tests, lactate dehydrogenase, peripheral smear and brain imaging. This case also supports investigative efforts to look for linkages between molar pregnancy and eclampsia to more fully uncover the aetiology of gestational hypertensive disorders.
Patient’s perspective
When I started feeling a really strange kind of pain that would not improve, I knew I needed to get help and suspected that the situation was potentially serious. I already knew about the things that could go wrong during pregnancy for me and the baby, since my doctor and I discuss a lot during my visits. Talking to my doctor made it easier for me to decide to get help, and knowing about risks early on and talking about them helps with improving safety.
Learning points
Gestational hypertensive disease can occur prior to 20 weeks’ gestation.
If gestational hypertensive disease does occur early in pregnancy, molar pregnancy should be suspected.
Patients with gestational hypertension and molar pregnancy should be regularly assessed for neurologic symptoms and promptly evaluated and treated.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors The following authors were responsible for drafting of the text, sourcing and editing of clinical images, investigation results, drawing original diagrams and algorithms, and critical revision for important intellectual content: DC, HV, KL and DZ. The following authors gave final approval of the manuscript: DC, HV, KL, DC, and DZ.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.