Article Text

Abstract
Adrenocortical carcinoma (ACC) is a rare form of cancer with an annual incidence of two per million. The risk of venous thromboembolism increases sevenfold in patients with cancer. This case report describes an iliac vein deep vein thrombosis (DVT) as an atypical presentation of an ACC and highlights the value of further imaging investigation in patients with unprovoked DVTs.
- Vascular surgery
- Endocrine cancer
- Pathology
Statistics from Altmetric.com
Background
The risk of venous thromboembolism (VTE) is up to sevenfold greater in patients with cancer when compared to individuals without cancer,1 and up to one-tenth of patients experiencing a VTE develop cancer within a year.1 The mechanisms of VTE in cancer are multiple: tumours induce a prothrombotic state by releasing procoagulant substances and inflammatory cytokines,2 and larger tumours can directly compress adjacent vessels resulting in venous stasis.
Adrenocortical carcinoma (ACC) is a rare and aggressive form of cancer with an annual incidence of two per million.3 Most tumours occur sporadically; however, in rare cases, ACCs are associated with hereditary syndromes such as Li-Fraumeni syndrome and multiple endocrine neoplasia type I.4 ACC is more common in women, and peak incidence is observed in children in the first decade of life or amongst adults in the fourth decade of life. Cases are typically detected following the onset of sequelae related to the mass effect of the tumour or overproduction of adrenal hormones. As a result of late diagnosis, patients experience a poor prognosis with a median survival time of 3.2 years.5
This case report highlights the case of an iliac vein deep vein thrombosis (DVT) as an atypical presentation of an ACC.
Case presentation
A female patient in her 20s with a background of asthma and a right-sided congenital non-functioning kidney presented to the emergency department with a 1-week history of left-sided lower limb pain and swelling, and a fortnight of abdominal bloating and discomfort.
Investigations
Initial investigations highlighted a raised D-dimer (1062 ng/mL, reference range: 0–230 ng/mL) hence duplex sonography was performed which demonstrated non-occlusive thrombus in the proximal common iliac vein and an occluded distal common iliac vein and external iliac vein (figure 1). The patient was immediately referred to vascular surgery for further assessment with a view to initiating treatment (pharmacomechanical thrombolysis).

Duplex sonography imaging demonstrating an occluded distal left-sided external iliac vein (yellow arrow).
As part of the thrombolysis work-up, a CT of the thorax, abdomen and pelvis (TAP) was performed which demonstrated the presence of a large right-sided suprarenal mass measuring 12.4×9.8×12.9 cm with heterogeneous enhancement and multifocal internal calcification (figures 2 and 3), and a completely calcified left-sided adrenal gland. Furthermore, multiple pulmonary nodules consistent with metastatic disease were observed bilaterally with the largest measuring 18.6 mm (figure 4). Thrombolysis was deemed inappropriate due to the risks associated with the procedure (bleeding) and the presence of metastatic malignancy. Moreover, based on the clinical assessment, the patient’s leg was deemed to be viable hence a decision was made to continue with medical treatment alone (thigh-length class II graduated compression therapy and two times per day 1 mg/kg enoxaparin) until her biopsy.

CT of the abdomen demonstrating a suprarenal mass.

CT of the abdomen demonstrating a suprarenal mass.

CT of the thorax demonstrating a metastatic lung nodule.
Differential diagnosis
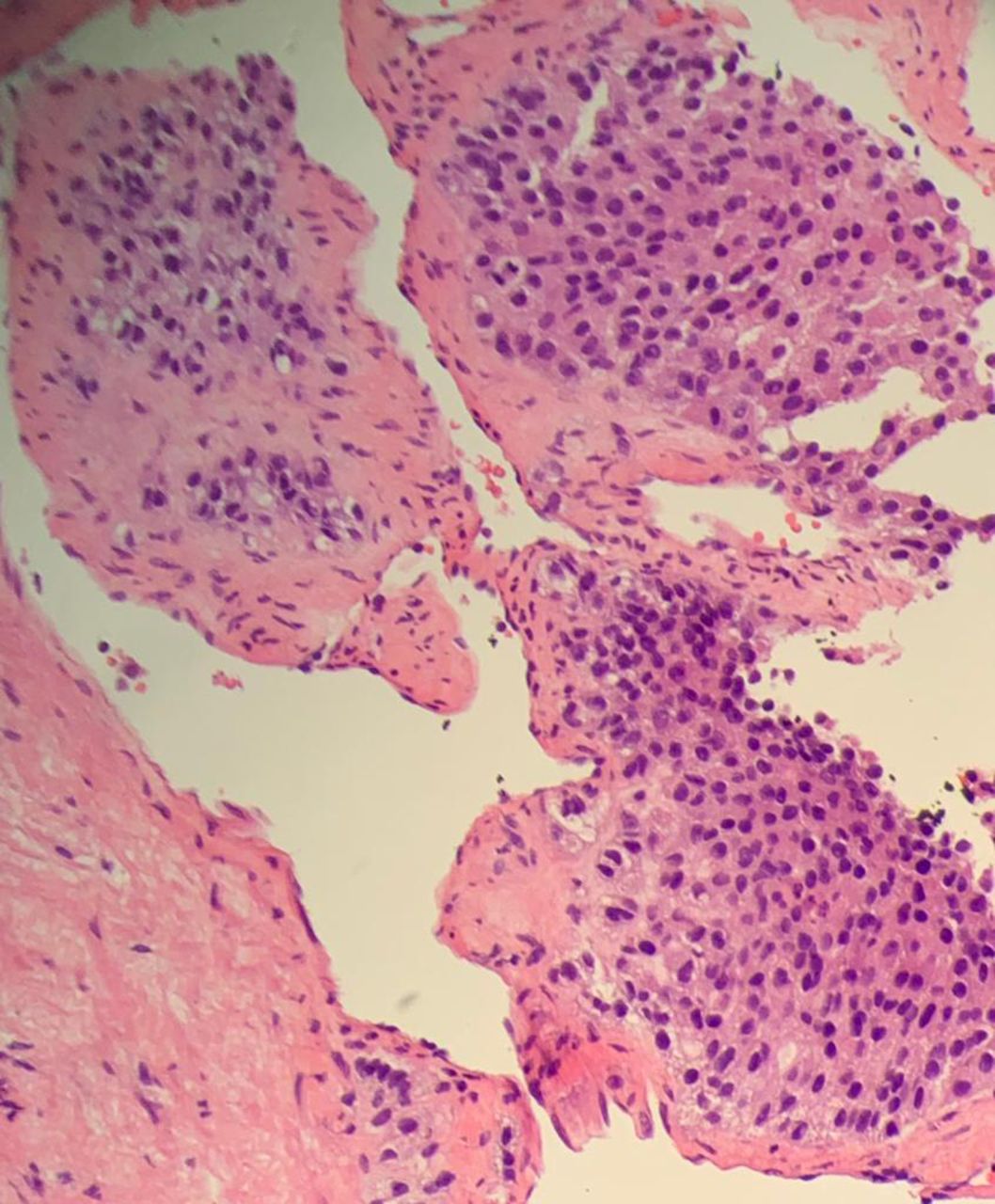
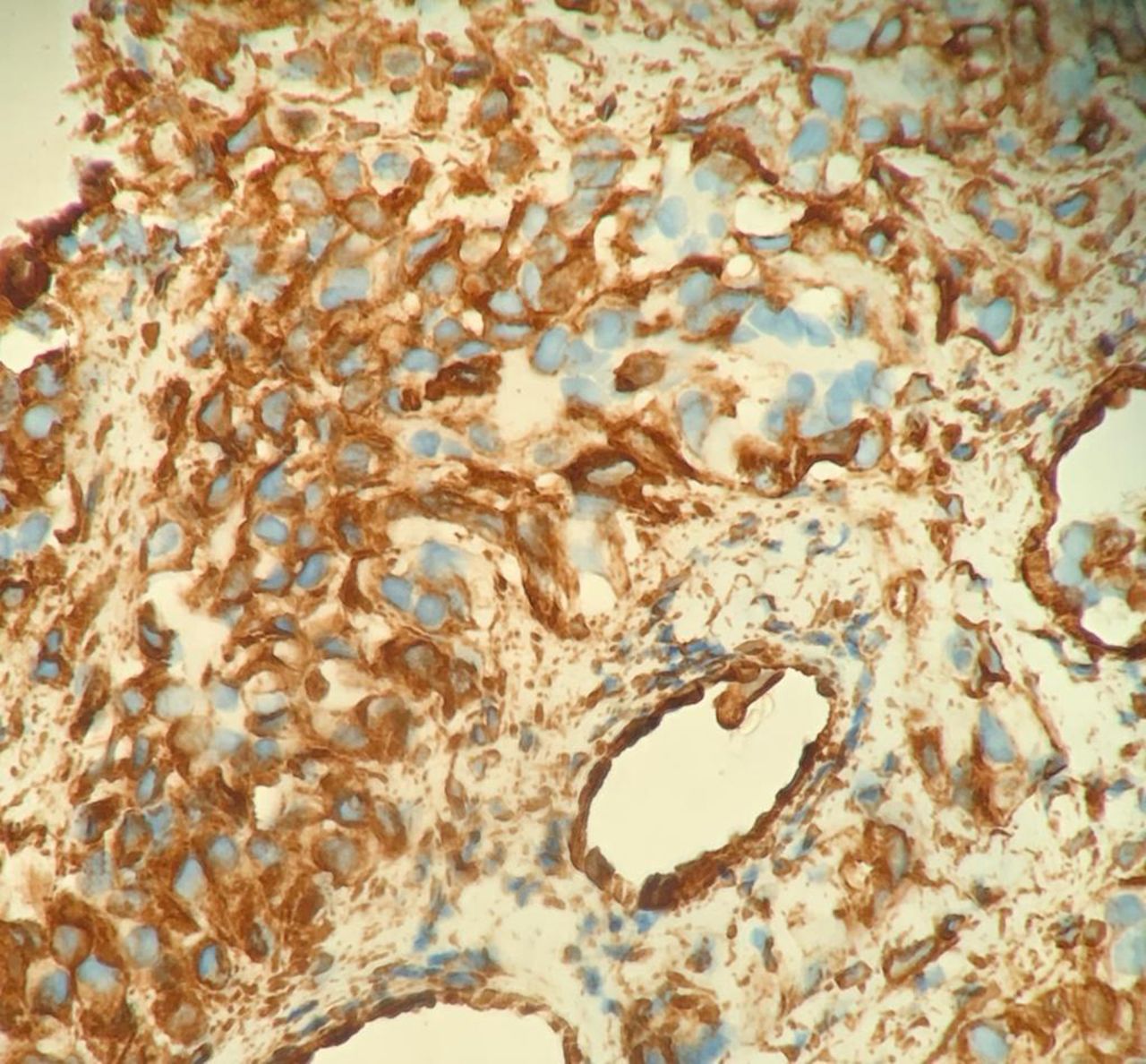
An ultrasound-guided core biopsy of her right suprarenal mass was taken and sent for histopathology assessment. Histological analysis demonstrated neoplastic cells with an epithelioid look arranged in nests (figure 5). Immunochemistry analysis demonstrated positive expression for calretinin (figure 6), CD56 (figure 7), synaptophysin (figure 8), vimentin (figure 9), p53 (figure 10), inhibin, NSE, CD99 and neurofilament, as well as a Ki67 expression of 10% (figure 11). At the time of her diagnosis, the patient’s serum cortisol (695 nmol/L, reference range: 102–535 nmol/L) and free androgen index were elevated (5.3, reference range: ≤4.5). Her serum metanephrine, normetanephrine and testosterone were all within normal range. In light of the known metastatic disease and immunophenotype analysis, a diagnosis of ACC was confirmed.

Histological sample demonstrates neoplastic cells with an epithelioid look arranged in nests; ×20 magnification.

Immunochemistry analysis demonstrates positive expression for calretinin; ×40 magnification.

Immunochemistry analysis demonstrates positive expression for CD56; ×40 magnification.

Immunochemistry analysis demonstrates positive expression for synaptophysin; ×40 magnification.

Immunochemistry analysis demonstrates positive expression for vimentin; ×40 magnification.

Immunochemistry analysis demonstrates positive expression for p53; ×20 magnification.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunochemistry analysis demonstrates positive expression for Ki67; ×20 magnification.
Treatment
Following her biopsy, a referral to oncology was made. Additionally, the patient was transitioned from enoxaparin onto apixaban (10 mg two times per day for 7 days, then 5 mg two times per day thereafter).
Outcome and follow-up
The patient is currently receiving a combined regimen of EDP-M (mitotane in combination with etoposide, doxorubicin and cisplatin) and is being supported by the local MacMillan nursing team throughout her treatment.
She continues to be seen regularly by the vascular team with regard to symptom control using conservative measures such as compression hosiery.
Discussion
Current data indicate that up to 10% of patients with an unprovoked DVT also present with a malignancy within a year,2 hence in patients who are previously fit and well, it is important to consider the possibility of an occult malignancy. The European Society of Vascular Surgery (ESVS) recommends that for individuals presenting with an unprovoked DVT, a thorough clinical history covering red flag symptoms and a meticulous physical examination should be conducted, followed by additional investigations if indicated.6 Evidence on the benefit of CT imaging for the investigation of cancer in patients with unprovoked DVTs is limited; a Cochrane review demonstrated that there was no significant difference in cancer-related deaths or VTE-related morbidity in patients receiving CT imaging for malignancy screening in comparison with standard VTE management.7 Nonetheless, at our vascular centre, we recommend a CT TAP (including a venogram) to plan potential deep venous intervention and to screen for malignancy in patients with unprovoked DVT.
Autopsy studies highlight that the prevalence of clinically unapparent adrenal masses is 2%.8 The Weiss scoring system can be used to distinguish ACCs from benign adrenal tumours; five histopathological features are evaluated: (1) mitotic rate (presence of >5 mitoses for 50 high power fields), (2) cytoplasm (presence of ≤25% clear tumour cells), (3) presence of abnormal mitoses, (4) presence of necrosis and (5) presence of capsular invasion.9 Evidence shows that a Weiss score of ≥3 is 96% specific and 100% sensitive for ACC.9
There are scarce reports of VTE as an initial presentation of an ACC. Both Lee et al10 and Aung et al11 reported cases of a left-sided ACC detected following a pulmonary embolism; however, our case report demonstrates the first published case of an ACC presenting with an iliac vein DVT.
ACCs can induce VTEs through multiple mechanisms. Over half of tumours are cortisol secreting, most commonly resulting in Cushing syndrome which can induce a prothrombotic syndrome.12 Moreover, ACCs can induce VTEs through their mass effect12; tumours have been reported to directly invade the inferior vena cava and in some cases extend into the right atrium,13 resulting in a large saddle pulmonary embolism.14
Curative treatment of stage I–III ACCs (as per the European Network for the Study of Adrenal Tumors classification system) consists of surgical resection with the addition of adjuvant mitotate therapy for a minimum of 2 years.15 In widespread metastatic (stage IV) ACC where surgical resection is not indicated, either mitotane monotherapy or the EDP-M regimen should be given.15 This patient received EDP-M.
In patients with malignancy-associated DVT, the ESVS recommends that patients with non-gastrointestinal or genitourinary cancers should be treated with direct oral anticoagulants. In our case, the patient was transitioned onto 6 months of two times per day 5 mg apixaban to reduce her risk of recurrent VTEs.
In summary, this case report demonstrates an example of rare malignancy-associated DVT and highlights the value of further radiological imaging in patients with unprovoked DVTs.
Learning points
In previously fit and well individuals with an unprovoked deep vein thrombosis, it is important to consider the possibility of an occult malignancy.
A thorough clinical history covering red flag symptoms and a meticulous physical examination should be conducted in patients with unprovoked deep vein thromboses.
Radiological imaging such as CT of the thorax, abdomen and pelvis should be used to identify tumours in patients suspected of having unprovoked deep vein thrombosis.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors ASB and TK designed the case report. ASB prepared the manuscript. TK and EA collected the images. All authors contributed to the revision of the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Case reports provide a valuable learning resource for the scientific community and can indicate areas of interest for future research. They should not be used in isolation to guide treatment choices or public health policy.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.