Article Text

Abstract
A 30-year-old man walked into the emergency department after a suicide attempt by firing a nail from a pneumatic nail gun directed at his left temple. He was haemodynamically stable and neurologically intact, able to recall all events and moving all extremities with a Glascow Coma Scale of 15. CT of the brain showed a 6.3 cm nail in the right frontal region without major intracerebral vessel disruption. He was taken to the operating room for left temporal wound washout, debridement of gross contamination and closure with titanium cranial fixation plate. The foreign body was not accessible on initial surgical intervention and was left in place to define anatomy and plan for subsequent removal. Thin slice CT images were used to create 3D reconstructions to facilitate stereotactic navigation and foreign body removal via right craniotomy the following day. The patient tolerated the procedures well and recovered with full neurological function.
- Trauma
- Bone and joint infections
- Mood disorders (including depression)
- Neurosurgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Nail gun injuries to the head are an extremely rare form of neurotrauma with a relatively low mortality and morbidity compared with high-velocity modalities. Due to its rare occurrence, clinical judgement of the neurosurgeon directs immediate and ongoing management. Few evidence-based guidelines for medical and surgical management currently exist.
Case presentation
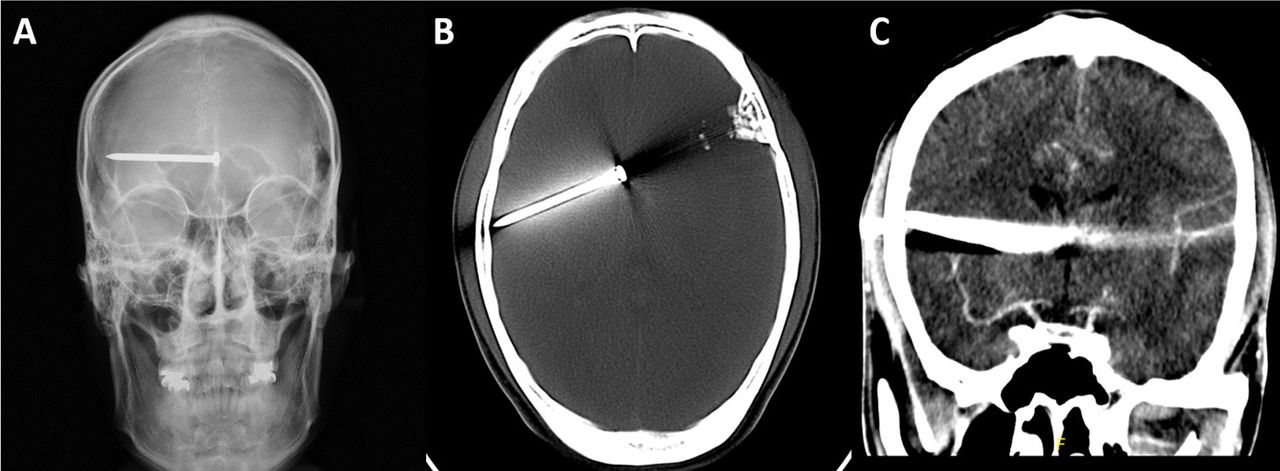
A 30-year-old man, recently initiated on antidepressant therapy for depression, walked into the emergency department with his wife after an apparent suicide attempt by firing a single nail from a pneumatic nail gun into his left temple. He denied any associated fall or loss of consciousness and reported that he walked home after the injury. His vital signs were within normal limits: blood pressure 147/92, heart rate of 72, respiratory rate 15, O2 100% on room air, rectal temperature 98.2°F. His Glasgow Coma Scale (GCS) was 15 and he did not have any neurological deficits. Secondary survey was significant for a 2 cm open wound at the left frontal temporal region with minimal bleeding from the skin edge. Emergent head X-ray confirmed a 7 cm nail in the right calvarium (figure 1A).

(A) Emergent X-ray of the skull, (B) CT scan of the head and (C) CT angiogram of the head.
Investigations
A CT and CT angiogram of the brain were obtained showing a 6.3 cm nail extending from the region of the right frontal horn through the parenchyma to the right inner table of the calvarium with scattered left hemispheric and intraventricular subarachnoid haemorrhage (figure 1B). There was no evidence of major intracranial vessel disruption on CT cerebral angiogram (figure 1C). Three-dimensional reconstruction from the CT head was performed in preparation for the neuronavigational device (figure 2).

Three-dimensional reconstruction from CT of the head showing penetration of the nail through the brain parenchyma from the left temporal entry site to the right temporal area.
Treatment
The patient was transferred to the surgical intensive care unit for haemodynamic and neurological monitoring. He was placed on levetiracetam for seizure prophylaxis and piperacillin/tazobactam for antimicrobial prophylaxis. Due to his stable neurological status and the presence of a contaminated open depressed skull fracture, we decided to manage his penetrating brain trauma and indwelling foreign body in a staged fashion. The patient was initially taken urgently for left temporal wound exploration, left frontal craniectomy and washout with the neurosurgery team. In the operating room (OR), it was discovered that particles of the plastic sheath and other accessories to the nail were embedded in the wound and dispersed in the epidural space. The area was thoroughly cleaned of debris and depressed skull fragments. The craniectomy was reconstructed using a titanium mesh plate. The temporalis fascia and skin were closed after wound washout. Postoperative CT of the brain showed a stable subarachnoid haemorrhage, and the patient recovered well after the procedure without new neurological deficits.
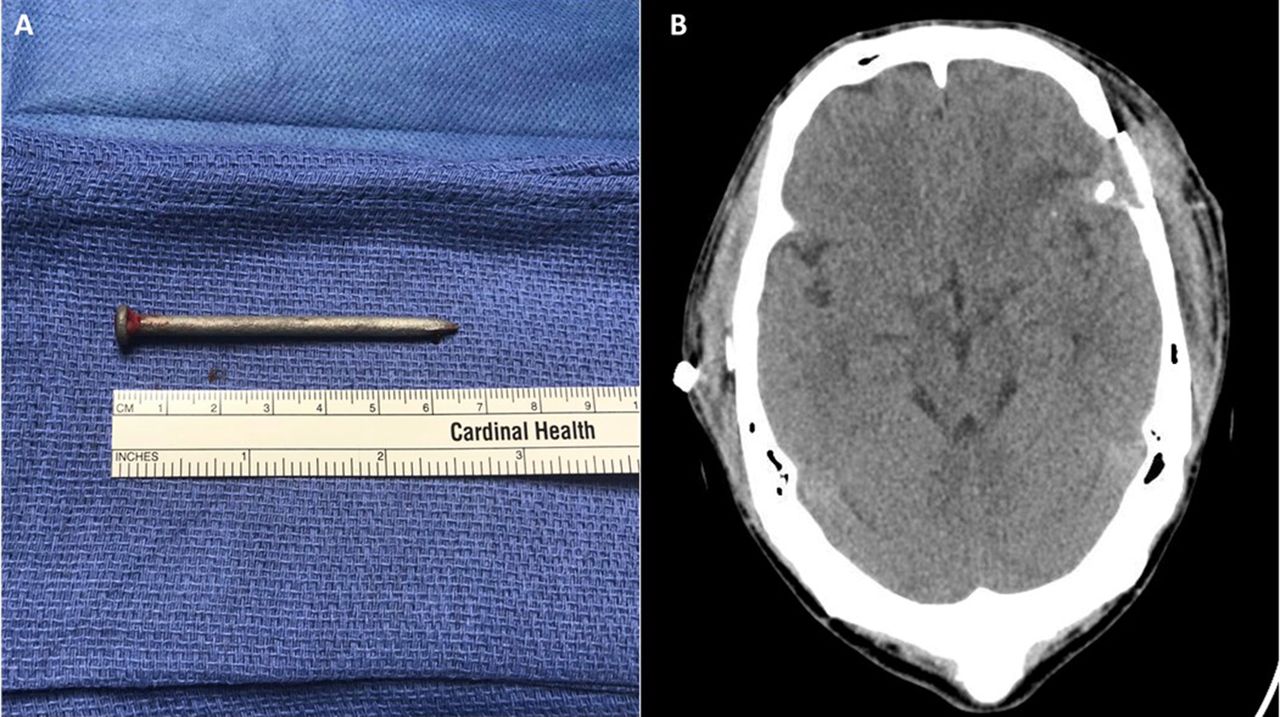
A discussion of the risks and benefits of returning to the OR for removal of the nail was carried out with the patient and his wife, specifically the elevated risk of infection from the nail was discussed. They agreed to undergo a second procedure; and 36 hours after initial presentation, the patient underwent a planned return to the OR for removal of the nail. Using a neuronavigation device (StealthStation Surgical Navigation, Medtronic) with preoperative CT, a small craniotomy was performed over the right frontotemporal region. On opening the skull, it was evident that the nail had penetrated the entire brain but did not maintain enough force to penetrate the skull at the right frontal area. There was an indentation at the right frontal bone created by the nail during the initial impact. After opening the dura, there was apparent brain contusion from the penetration of the nail (figure 3A). Bipolar forceps were used to carefully incise into the cerebral parenchyma. The tip of the nail was then seen and grasped using an Aliss clamp (figure 3B). The nail was then carefully extracted from the parenchyma without resistance (figure 4A). Postoperative CT shows decrease in the intracranial haemorrhage (figure 4B).

(A) Intraoperative image of cerebral parenchyma with an apparent brain contusion from nail (white arrow). (B) Removal of the nail from the cerebral parenchyma.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Removed nail measuring 6.5 cm. (B) Postoperative CT scan of the head.
Outcome and follow-up
Postoperatively, the patient developed persistent fevers with no other clinical findings concerning for possible meningitis. The infectious disease team recommended 6 weeks of broad-spectrum antibiotics (vancomycin and meropenem). However, the patient developed a drug rash and was switched to oral doxycycline. He remained afebrile and recovered well from surgery, without any apparent neurological deficits. He was eventually discharged to an inpatient psychiatric facility for 7 days where he made a successful recovery.
Discussion
Penetrating brain injury (PBI), although less common than closed head injuries, typically carries a worse prognosis.1 Most PBI are caused by high-velocity projectiles which result in more complex anatomical disruption and higher mortality than low-velocity injuries. Low-velocity penetrating injuries to the head are extremely rare and usually confer better outcomes.2
As nail guns become more readily available in industrial and in-home settings, nail gun-related injuries have also increased in numbers. A 2007 report by Centers for Disease Control and Prevention reported nail gun-related injuries increased 200% since 1991 with estimated 37 000 cases annually.3 Most injuries are sustained to the upper extremities, primarily fingers and hands, and only case reports or case series of nail gun injuries exist. Interestingly, most of these injuries are related to nail gun misuse associated with assault or suicide attempts rather than accidental injuries.4 One systematic review found that greater than 65% of nail gun injuries are associated with suicide attempts.5
The majority of penetrating intracranial nail injuries present without focal neurological findings and death is rare.6 However, if present, neurological symptoms described include altered mental status, hemiparesis, paresthesia, ophthalmoplegia and cranial nerve deficits.7–10 In a literature review by Woodall et al, 50% patients had no neurological deficit on presentation, and a GCS of 7 or less was associated with mortality in 75% of included cases.5 The explanation for better outcomes in nail gun injuries compared with other penetrating injuries is the relatively low velocity which confers lower kinetic energy generated by the nail gun.11 Projectiles from nail guns travel at approximately 100 ft/s as compared with conventional firearms which travel at 300–2200 ft/s. Therefore, the mechanism and extent of injuries are significantly more traumatic with firearms.
In general, surgical treatment for PBI primarily focuses on treating mass effect and decreasing the risk of infectious complications.4 12 Small entrance wounds to the scalp and skull can be managed with local wound care; however, large and/or complex wounds should be extensively debrided with subsequent primary closure or grafting to achieve a watertight closure.4 Routine removal of small bone and missile fragments is not recommended due to the associated high morbidity.13 Delayed removal of dirty foreign body such as wood has been shown to increase morbidity in comparison with emergent surgical treatment.14 Several reports of intracranial nails left in place showed no significant clinical deficits, but Spennato et al describe a case in which the nail was discovered approximately 3 years after initial trauma, after the patient presented with focal seizure activity.15 In the presented case, we first took the patient urgently for a debridement of the entry wound to remove foreign bodies and bone fragments. With further imaging and planning, we returned to the OR with a neuronavigation device to remove the nail from the contralateral side of the entry wound.
Vascular complications from nail gun injuries have been reported including secondary pseudoaneurysms and intracranial haemorrhage.16–18 It is vital to have initial and follow-up angiograms due to the high mortality rate of ruptured aneurysms which occur 2–3 weeks after initial injury.4 5 Identified pseudoaneurysms should be aggressively treated via endovascular or open approach. When the initial angiography is negative and there is continued suspicion, it should be repeated in 2–3 weeks.
There is not sufficient clinical data to provide an appropriate antibiotic regimen specifically for intracranial nail gun injuries. However, in general, infection after PBI is associated with increased morbidity and mortality.19 The rate of local wound infection, meningitis and brain abscess are elevated among patients with PBI secondary to the contaminated foreign object, skin and bone fragments brought into the brain parenchyma along the projectile track. Before the advent of antibiotics, the rate of these infectious complications was reported to be as high as 58.8% in the military population.20 Staphylococcus aureus and gram-negative organisms are commonly associated with these complications; therefore, broad-spectrum antibiotic regimens are most often used.4 19 In the literature, various antibiotic regimens are used and proposed for prophylaxis in nail gun brain injuries.7 10 21 In our case, infectious disease recommended piperacillin/tazobactam preoperatively and vancomycin and meropenem for 6 weeks postoperatively.
Prior cases of intracranial nail gun injuries have been associated with psychiatric issues such as schizophrenia and major depressive disorder.22 Psychiatric services should be involved for any suicide attempt survivors for diagnosis and management during and after treatment of injuries. This patient was diagnosed with major depressive disorder and was started on escitalopram 20 mg once a day. He has been followed by the psychiatry service regularly since discharge, which accentuates the importance of maintenance and follow-up for mental health.23
Learning points
Nail gun injuries to the head often present without neurological deficits due to the low velocity of the nail gun, resulting in less tissue and vascular disruption.
Cerebral angiography should be performed in this setting to rule out intracranial vascular injury and pseudoaneurysm.
Care providers should direct attention to determining if there is a need for emergent surgery. Literature review suggests immediate surgical exploration to remove gross contamination and control haemorrhage.
Initiation of broad-spectrum antibiotic therapy is advisable as soon as possible after recognising such injuries.
References
Footnotes
Contributors RCZ and MCY contributed to the writing and editing of the paper; while MK and NL contributed to the planning, conception and editing of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.