Article Text

Statistics from Altmetric.com
Description
We report the case of an 81-year-old male patient who was admitted to our hospital because of multiple cerebral ischaemic strokes. On day 2 of hospitalisation, he developed Pseudomonas aeruginosa sepsis, possibly secondary to a concomitant bladder infection. At day 3 of hospitalisation, tenderness of the right wrist with clinical signs of inflammation evolved. The peripheral intravenous access, localised distally of the radiocarpal joint, was initially suspected as the source of local infection (figure 1).

Right wrist: tenderness, hyperaemia and swelling of the ulnar part of the skin over the wrist.
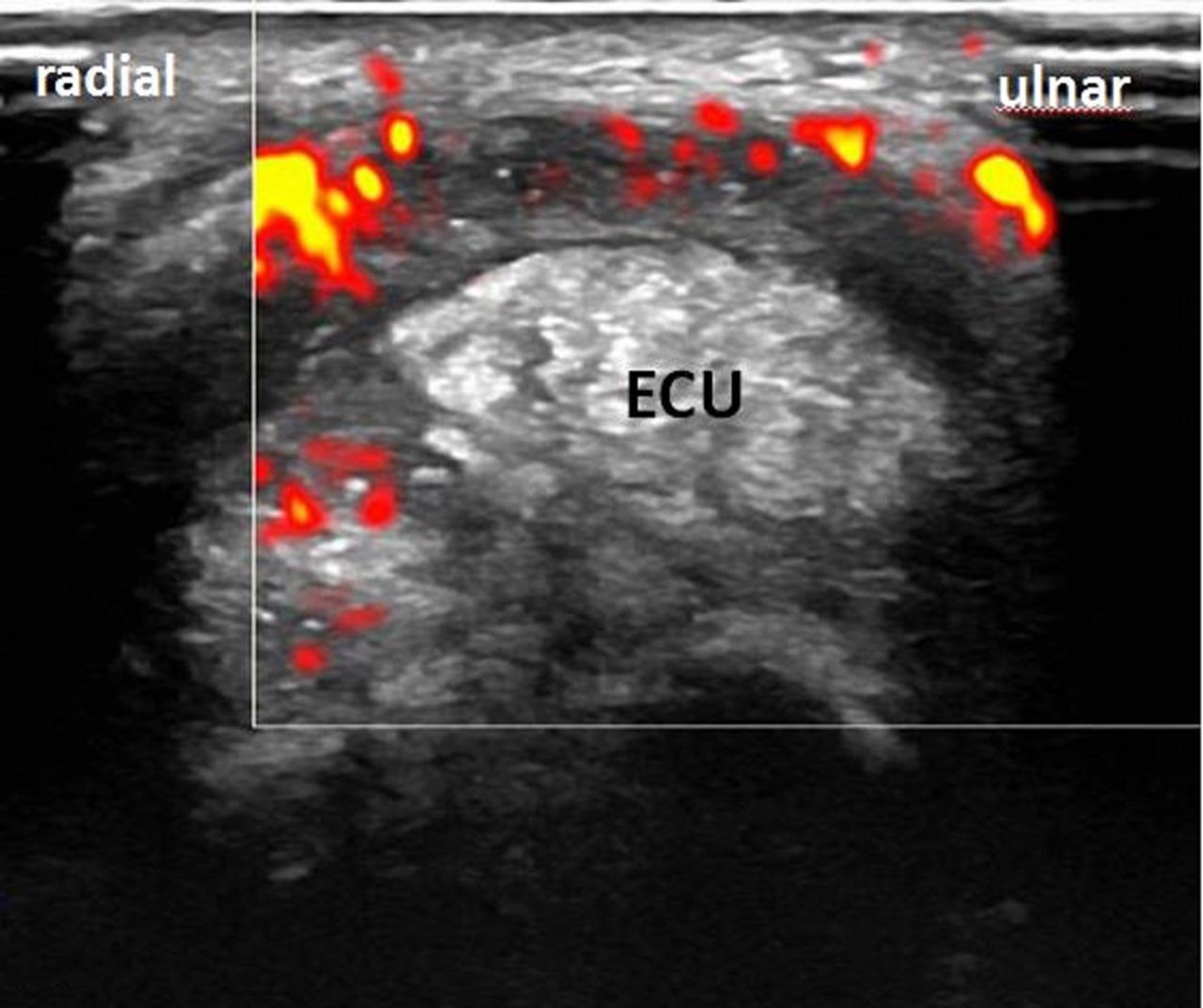
Subsequent ultrasound examination of the wrist showed signs of tenosynovitis of the extensor carpi ulnaris (ECU) tendon with tendon thickening and peritendinous effusion (figure 2), while the radiocarpal joint revealed only grade 1 synovitis which did not explain the overall clinical appearance.1 In the absence of elevated serum urate levels, we suspected infectious tenosynovitis which might occur through haematogenous seeding or puncture wounds.2

Transverse scan of the extensor carpi ulnaris (ECU): hyperaemia on colour Doppler, inhomogenous tendon thickening with hypoechogenic areas and surrounding halo sign.
Tenosynovial fluid drawn by ultrasound-guided puncture of the ECU sheath revealed monosodium urate crystals on polarised light microscopy, and a diagnosis of gouty tenosynovitis was established (figure 3 and figure 4). Injection with glucocorticosteroids into the tenosynovial sheath was performed and symptoms resolved after 3 days.

Longitudinal scan of the ECU: ultrasound-guided centesis of the tenosynovial sheath (arrow indicates the needle). ECU, extensor carpi ulnaris; OsT, os triquetrum; OsU, os ulnar head.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Polarised light microscopy of tenosynovial fluid (x100): strong negative birefringence, needle-shaped crystals identified as monosodium urate crystals.
This clinical image demonstrates the diagnostic value of the examination of joints as well as tendons by ultrasound. Differential diagnosis of tenosynovitis of the wrist include rheumatoid arthritis, psoriatic arthritis, infectious tenosynovitis (may occur by haematogenous seeding or through puncture wounds) and calcium pyrophosphate dihydrate crystal deposition disease.2–5
Our example demonstrates that gout attacks can predominantly affect tendons, without major involvement of adjacent joints. In patients with infectious diseases and sonographic signs of tenosynovitis, centesis of the tenosynovial sheath and microscopic examination for crystals should be performed as gout flares can lead to tenosynovitis and mimic infectious tenosynovitis.6
Learning points
Gout attacks may manifest as tenosynovitis without involvement of adjacent joints.
Centesis of the tenosynovial sheath and microscopic examination should be encouraged in acute tenosynovitis as gout flares may mimic infectious tenosynovitis.
Footnotes
Contributors IFJP was involved in treating the patient, performing of the intervention and in drafting and writing the manuscript. PR was involved in treating the patient and was a major contributor in writing the manuscript and critically revising the manuscript for important intellectual content. JvK was involved in treating the patient, critically revising for important intellectual content and has given final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Next of kin consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.