Article Text

Abstract
SARS-CoV-2 infection may affect the liver in healthy individuals but also influences the course of COVID-19 in patients with chronic liver disease (CLD). As described in healthy individuals, a strong SARS-CoV-2-specific adaptive immune response is important for the outcome of COVID-19, however, knowledge on the adaptive immune response in CLD is limited.
Here, we review the clinical and immunological features of SARS-CoV-2 infection in individuals with CLD. Acute liver injury occurs in many cases of SARS-CoV-2 infection and may be induced by multiple factors, such as cytokines, direct viral infection or toxic effects of COVID-19 drugs. In individuals with CLD, SARS-CoV-2 infection may have a more severe course and promote decompensation and particularly in patients with cirrhosis. Compared with healthy individuals, the SARS-CoV-2-specific adaptive immune responses is impaired in patients with CLD after both, natural infection and vaccination but improves at least partially after booster vaccination.
Following SARS-CoV-2 vaccination, rare cases of acute vaccine-induced liver injury and the development of autoimmune-like hepatitis have been reported. However, the concomitant elevation of liver enzymes is reversible under steroid treatment.
- LIVER
- LIVER CIRRHOSIS
- LIVER IMMUNOLOGY
- AUTOIMMUNE LIVER DISEASE
- DRUG INDUCED LIVER INJURY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Clinical features of COVID-19 in CLD patients with CLD and healthy individuals
Immunological features of COVID-19 in CLD patients
Induction of autoimmune-like hepatitis (ALH) after COVID-19 vaccination)
Introduction
Since 2019, more than 750 million confirmed SARS-CoV-2 infections with 6.8 million deaths have been reported worldwide with an estimated high number of unreported cases.1 2 SARS-CoV-2 infection may present with symptoms ranging from upper respiratory tract complaints to multisystem organ failure.3 4 The fast development of effective vaccines has been a milestone in the fight against the pandemic. SARS-CoV-2 vaccines approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) are based on various platforms, such as mRNA, inactivated virus or adenovectors. They provide protection against severe SARS-CoV-2 infection by inducing virus-specific humoral and cellular immune responses.5–9 While antibodies may provide protection against infection, virus-specific T cell responses are thought to prevent a severe course of COVID-19.10 11
Numerous studies on the clinical features of SARS-CoV-2 infection and the infection-induced or vaccine-induced immune response have been conducted. However, most of these studies focused on healthy individuals. Thus, knowledge about the clinical impact of SARS-CoV-2 infection and the induction and the role of the adaptive immune response in vulnerable populations, including patients with chronic liver disease (CLD) or immunosuppressed liver transplant recipients (LTR) remains scarce.
Here, we will discuss first, the current knowledge about the clinical features of COVID-19 in patients with liver disease and second, their link to immunological responses induced after natural infection and vaccination.
SARS-CoV-2 infection and the liver in healthy individuals
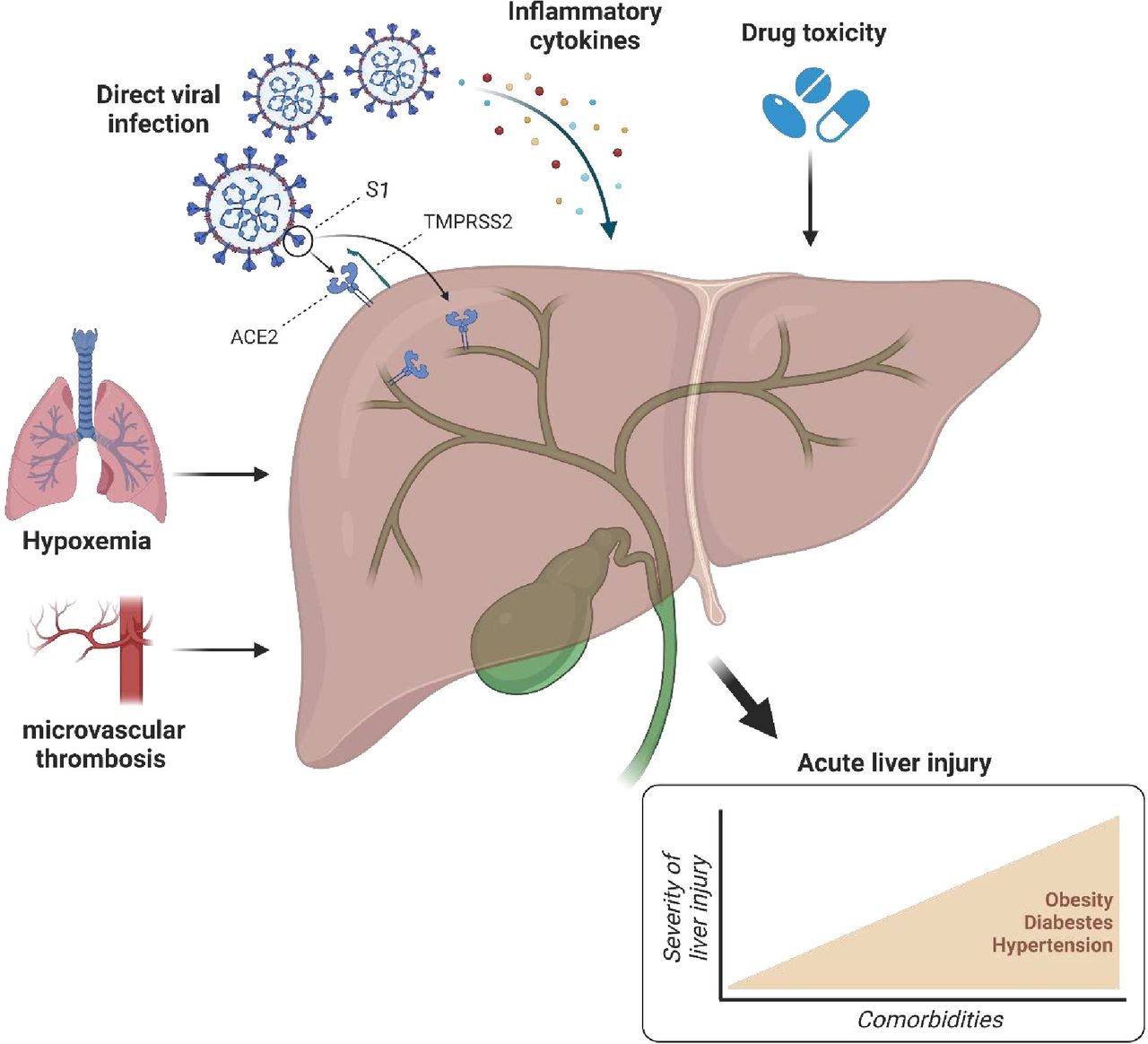
Liver function abnormalities have been observed in more than a third of hospitalised SARS-CoV-2-infected individuals with moderate or severe infection,12–16 while liver function was only rarely impaired in patients with asymptomatic or mild COVID-19.17 SARS-CoV-2-related liver injury is associated with male gender and certain medical conditions such as diabetes mellitus, obesity or metabolic-associated fatty liver disease12 18 (figure 1). The underlying molecular mechanisms are still not well understood. On the one hand, multiple indirect factors are discussed, for example, systemic inflammation, intrahepatic immune activation, hypoxaemia, microvascular thrombosis or drug toxicity12 19–21 (figure 1). On the other hand, in the liver, ACE2 receptors are expressed on cholangiocytes and to a lesser extent on hepatocytes suggesting that SARS-CoV-2 may directly enter these cells.22 23 It has already been shown in SARS-CoV-1 infection, that the virus is detectable in the liver tissue by RT-PCR and associated with mild to moderate lobular inflammation and apoptosis.24 25 Also co-receptors, such as the scavenger receptor class B member 1 (SRB1), could play an important role in the liver tropism of SARS-CoV-2 as it facilitate the entry of the virus in the liver.26 Thus, it is tempting to hypothesise that intrahepatic inflammation in SARS-CoV-2 infection may also be directly caused by viral infection of bile duct cells and hepatocytes. In line with this hypothesis, Chornenkyy et al 27 and Lagana et al 28 were able to detect SARS-CoV-2 RNA in hepatocytes of 4/9 (44%) and 11/20 (55%) patients, respectively, who died of COVID-19. Histological analysis of postmortem liver biopsies from SARS-CoV-2 infected individuals further revealed sinusoidal congestion with microthrombosis, hepatic apoptosis and binucleated hepatocytes as correlates of hepatocyte impairment.29 30 This has been associated to both, COVID-19 particles in the cytoplasm of hepatocytes and hypoxaemia resulting from reduced pulmonary function in patients with COVID-19.16 29 While hypoxia-induced liver injury is usually reversible after clearance of infection, it is still unclear how long hepatocyte damage from direct viral infiltration may persist. However, since a high viral load is likely to be associated with a severe course of infection,31 further studies are needed to determine whether SARS-CoV-2 is also detectable in the liver of patients with mild or moderate infection who have a lower viral load. In contrast to the previously discussed findings, Massoth et al could not detect SARS-CoV-2 in the liver of 8 deceased SARS-CoV-2-infected patients using an RT-PCR assay.32 This may be explained either by a viral load below the detection limit, or it may indicate that the organ damage could be explained by other, for example, immune-mediated mechanisms. Furthermore, it is possible that the presence of ACE2 does not fully explain the liver tropism of SARS-CoV-2 with a discordance between the presence of ACE2 and SARS-CoV-2 in different organs. This hypothesis may be supported by an observation from SARS-CoV-1, where the virus was detectable in colonic epithelium, which does not express ACE2, but not in endothelial cells, which do express ACE2.33 Although not yet confirmed in humans, Brevini et al recently described in a mouse model that ursodeoxycholic acid is able to block ACE2 and may, therefore, be an interesting approach for the treatment and prophylaxis of SARS-CoV-2.34 Since rectal swabs for SARS-CoV-2 can be positive even when oral swabs were negative, liver tropism may also be influenced by the gut-liver axis with viral translocation via the portal vein (reviewed in Mohandas and Vairappan35). Patients with severe liver injury often manifested gut abnormalities,35 suggesting that patients gut abnormalities may benefit from a close monitoring of transaminases and cholestatis parameters in the clinical routine to screen for liver involvement in COVID-19.

Pathophysiology of SARS-CoV-2-induced acute liver injury in healthy individuals. Acute liver injury can have different reasons including microvascular thrombosis, hypoxaemia, drug toxicity, inflammatory cytokines or direct viral infection of hepatocytes and cholangiocytes, which express ACE2. The presence of comorbidities, such as obesity, diabetes and hypertension, is associated with more severe liver injury. S1, spike protein subunit 1; TMPRSS2, transmembrane protease serine subtype 2.
SARS-CoV-2-induced liver injury can also be immune-mediated. SARS-CoV-2 infected individuals display higher levels of cytokines such as tumour necrosis factor alpha (TNFα) or IFN-gamma (IFNγ) and, notably, levels of CXCL10, CCL2 and TNFα are higher in patients with severe disease treated at the intensive care unit (ICU).36 37 This hypercytokinaemia can contribute to endothelial dysfunction and increased generation of reactive oxygen species, resulting in capillary leakage syndrome and subsequent hepatic cell injury by hypoperfusion (reviewed in Anirvan et al 36).
For SARS-CoV-2 infection, several treatment options are available, including dexamethasone, baricitinib in combination with remdesivir or nirmatrelvir/ritonavir that have all been shown to reduce mortality in symptomatically infected patients.38 39 However, some of these drugs may also cause liver injury. For example, remdesivir, a nucleotide analogue RNA polymerase inhibitor, has been described to induce hepatocellular damage with elevated transaminases suggesting close monitoring of liver function tests especially in subjects with CLD.39 40 In contrast, other commonly used antiviral drugs such as the combination of nirmatrelvir (viral 3CL protease inhibitor) with ritonavir (cytochrome P450 inhibitor) or molnupiravir (impairs viral replication) have a favourable hepatic safety profile.39 41
Taken together, acute liver injury in the context of SARS-CoV-2 infection can be caused by different mechanisms including systemic inflammation, hypoxaemia, direct viral infection of hepatocytes and cholangiocytes as well as drug-induced liver injury. However, in our opinion, the systemic inflammatory response and drug-induced mechanisms appear to be more relevant than direct viral infection of liver cells in the development of liver injury. In consequence, the high proportion of SARS-CoV-2-infected individuals with liver function abnormalities corroborates the need for consistent monitoring of liver function in routine clinical practice.
SARS-CoV-2 and clinical impact on CLD
CLD is a global health burden with high morbidity and mortality.42 Currently, the impact of SARS-CoV-2 infection or vaccination on patients with CLD is not fully understood, however, there is a growing body of data available for various CLD entities such as non-alcoholic fatty liver disease (NAFLD), viral hepatitis or autoimmune hepatitis (AIH) that we will discuss in the following.
SARS-CoV-2 and liver cirrhosis
Patients with liver cirrhosis are more susceptible to infections compared with the general population.43 This is partly due to a cirrhosis-associated immune dysfunction with high levels of proinflammatory cytokines that may also explain the higher mortality of infections in this patient group.44 This observation is also applicable for SARS-CoV-2 infection where mortality is higher in patients with liver cirrhosis compared with individuals without CLD.45–47 SARS-CoV-2-associated mortality increases in parallel with the Child-Pugh score and is higher in patients with decompensated compared with compensated cirrhosis.45 48 However, mortality is reduced in fully vaccinated compared with unvaccinated cirrhotics.49
Similar to other respiratory viral infections, such as influenza virus infection, SARS-CoV-2 infection is able to cause acute-on-chronic liver failure (ACLF) or decompensation of a previously compensated cirrhosis.45 50 Most likely, the systemic inflammation induced by the viral infection, serves as a trigger for the development of ACLF as it is accompanied by increased levels of cytokines.51
Another tempting hypothesis for the development of ACLF in COVID-19 is the direct viral infection of the liver by SARS-CoV-2. As discussed above, ACE2 receptors are expressed on cholangiocytes and hepatocytes22 23 and in patients with CLD, the expression of ACE2 is even further increased.52 53 Consequently, this may contribute to a higher viral load in the liver and thus to acute decompensation of liver function.
Taken together, given their increased susceptibility to infection, patients with cirrhosis may particularly benefit from protective measures to prevent infection.
SARS-CoV-2 and NAFLD
NAFLD summarises several histological entities of steatosis that may occur without relevant inflammation (non-alcoholic fatty liver, NAFL) or in an inflammatory stage (non-alcoholic steatohepatitis, NASH) with hepatocyte injury (hepatocyte ballooning).54 The inflammatory process in the adipose tissue is accompanied by an upregulation of proinflammatory cytokines, for example, TNFα, IL-1 and IL-6, as well as by an increased infiltration of immune cells, such as macrophages, B and T cells.55 This inflammatory environment is also important in the context of COVID-19, where patients with underlying NAFLD are at higher risk of developing severe COVID-19 and being admitted to the ICU as well as for higher liver-related mortality.56–59 Indeed, it has been shown that SARS-CoV-2 infection is also associated with the release of high levels of TNFα, IL-1 and IL-6.36 37 60 This accumulation of cytokines may explain the severe COVID-19 courses in NALFD patients compared with the general population, as high cytokine levels can lead to life-threatening manifestations with multiorgan dysfunction.60 Furthermore, it is tempting to speculate that the more severe COVID-19 courses are also promoted by organ manifestations of the metabolic syndrome, including cardiovascular disease, diabetes mellitus type 2 and obstructive sleep apnoea, which are common in NAFLD patients. Additionally, as previously described for patients with cirrhosis, higher expression of hepatic ACE2 was also observed in NAFLD patients. Interestingly, Zhang et al could detect higher levels of ACE2 in the liver of rats with high fat diet-induced NASH.61 Thus, an NAFLD-associated higher ACE2 expression may suggest an increased risk of SARS-CoV-2 entry into the liver resulting in a more severe liver injury compared with individuals without NAFLD. Taken together, the development of severe SARS-CoV-2 infection in NAFLD patients is likely to be multifactorial.
SARS-CoV-2 and viral hepatitis
Viral hepatitis is a global disease burden with >250 million cases of chronic hepatitis B virus (HBV) infection and >70 million chronic hepatitis C virus (HCV) infections worldwide.62 Limited data on SARS-CoV-2 infections in patients with chronic HBV and HCV infection show conflicting results. For example, in HBV/SARS-CoV-2 co-infected patients, some studies have reported a higher severity and mortality of COVID-19 compared with the general population,63 64 while this has not been observed by others.65 66 Similarly, in HCV/SARS-CoV-2 co-infection, some reports have indicated a similar COVID-19 outcome compared with healthy individuals,67 while others have shown a higher SARS-CoV-2-associated mortality in HCV-infected patients.68
There are several possible explanations for these conflicting results. For example, antiviral agents for the treatment of chronic HBV (tenofovir) and chronic HCV (sofosbuvir) infection may have a beneficial effect on the outcome of SARS-CoV-2 infection, since they are able to interact with SARS-CoV-2 by inhibiting the SARS-CoV-2 RNA-dependent RNA polymerase and thus viral replication.69 On the other side, a more severe outcome can be explained by an overexpression of TMPRSS2 in patients with HBV or HCV infection.70 71 Notably, TMPRSS2 is responsible for spike protein priming and is thus essential for viral entry into primary targets. Therefore, higher expression of TMPRSS2 may promote a higher viraemia and consequently a more severe COVID-19 outcome.72 Therefore, blocking TMPRSS2 may be a potential mechanism for treatment and prevention in patients with high expression of TMPRSS2, such as HCV patients. In this context, nafamostat and camostat have been identified as potential drugs against SARS-CoV-2, as they are able to inhibit SARS-CoV-2 infection by binding to the TMPRSS2 catalytic centre, resulting in inhibition of proteolytic activation of the spike protein.73 However, the effect of these drugs has so far not been investigated in patients with CLD.
SARS-CoV-2 and AIH
Patients with AIH often require immunosuppressive therapy, such as corticosteroids or thiopurines, to control the disease and are, therefore, at higher risk for viral infections compared with the general population.74 Along this line, immunosuppressive therapy with glucocorticoids is associated with a higher risk for severe COVID-19 in patients with rheumatoid arthritis.75 However, in SARS-CoV-2-infected AIH patients, who were mostly under immunosuppressive therapy, Marjot et al observed similar rates of hospitalisation, intensive care and mortality compared with the general population.76 This observation confirms previous reports suggesting a similar clinical course of SARS-CoV-2 infection and mortality in healthy controls and AIH patients treated with prednisone or a combination of glucocorticoids and thiopurine.77 78
However, the choice of the immunosuppression drug and the dosage may play an important role in the outcome of SARS-CoV-2 infection. Indeed, Efe et al analysed the effect of immunosuppressive therapy in SARS-CoV-2-infected AIH patients and observed a worse outcome in a small cohort of patients treated with mycophenolate mofetil (MMF) or tacrolismus compared with other immunosuppressive agents such as glucocorticoids or thiopurines.79 However, due to the small sample size, these observations need to be validated in a larger cohort. Efe et al also observed a worse outcome in AIH patients treated with glucocorticoids compared with AIH patients without immunosuppression, and this effect was enhanced in patients with doses >5 mg/day.79
These findings have important implications for the management of AIH patients in the clinical routine, since withdrawal of immunosuppression during SARS-CoV-2 should be a case-by-case decision weighing the risk of a worse outcome of COVID-19 against the risk of AIH relapse.
SARS-CoV-2 and liver transplantation
LTRs require long-term immunosuppression to prevent graft rejection. Similar to immunosuppressed AIH patients, immunosuppressive treatment generally increases the risk of infection in this patient group,80 and therefore, LTR are thought to especially benefit from protective measures to prevent infection. Indeed, LTRs show higher frequencies of SARS-CoV-2 infection compared with the general population.81 Since immunosuppressive agents may also influence the severity of the disease, the question can be raised whether immunosuppressive therapy should be reduced or even discontinued in LTR during SARS-CoV-2 infection. In a cohort of 111 LTR, MMF in particular at doses >1000 mg/day, was associated with severe COVID-19, whereas calcineurin inhibitors and mTOR inhibitors did not show this association.81 This dose-dependent effect of MMF may be explained by its cytotoxic effect on lymphocytes, which may exacerbate the already existing lymphocytopenia observed during SARS-CoV-2 infection, where lymphocyte count, T cells, B cells and NK cells are decreased in parallel with disease severity.82 Thus, a temporary reduction in the dose of MMF may have a beneficial effect on disease outcome.
SARS-CoV-2 and the adaptive immune response
The adaptive cellular and humoral immune response plays an important role in immunity against viral infections of the respiratory tract.83 Antibodies are detectable in almost all healthy individuals following SARS-CoV-2 infection or vaccination and are capable of neutralising the virus by preventing the interaction of the viral spike receptor binding domain with the host ACE2 receptor6 84–86 (figure 2A). Similar to virus-specific antibodies, SARS-CoV2-specific T cells are also rapidly induced by both, natural infection and vaccination8 85 87 88 (figure 2A), and the vaccine-induced T cell epitope repertoire is largely conserved in currently circulating variants, including Omicron.89 90 They are involved in viral clearance and provide protection against severe COVID-19 through the expression of effector molecules such as interferon γ (IFN-γ) or granzyme B.91–94

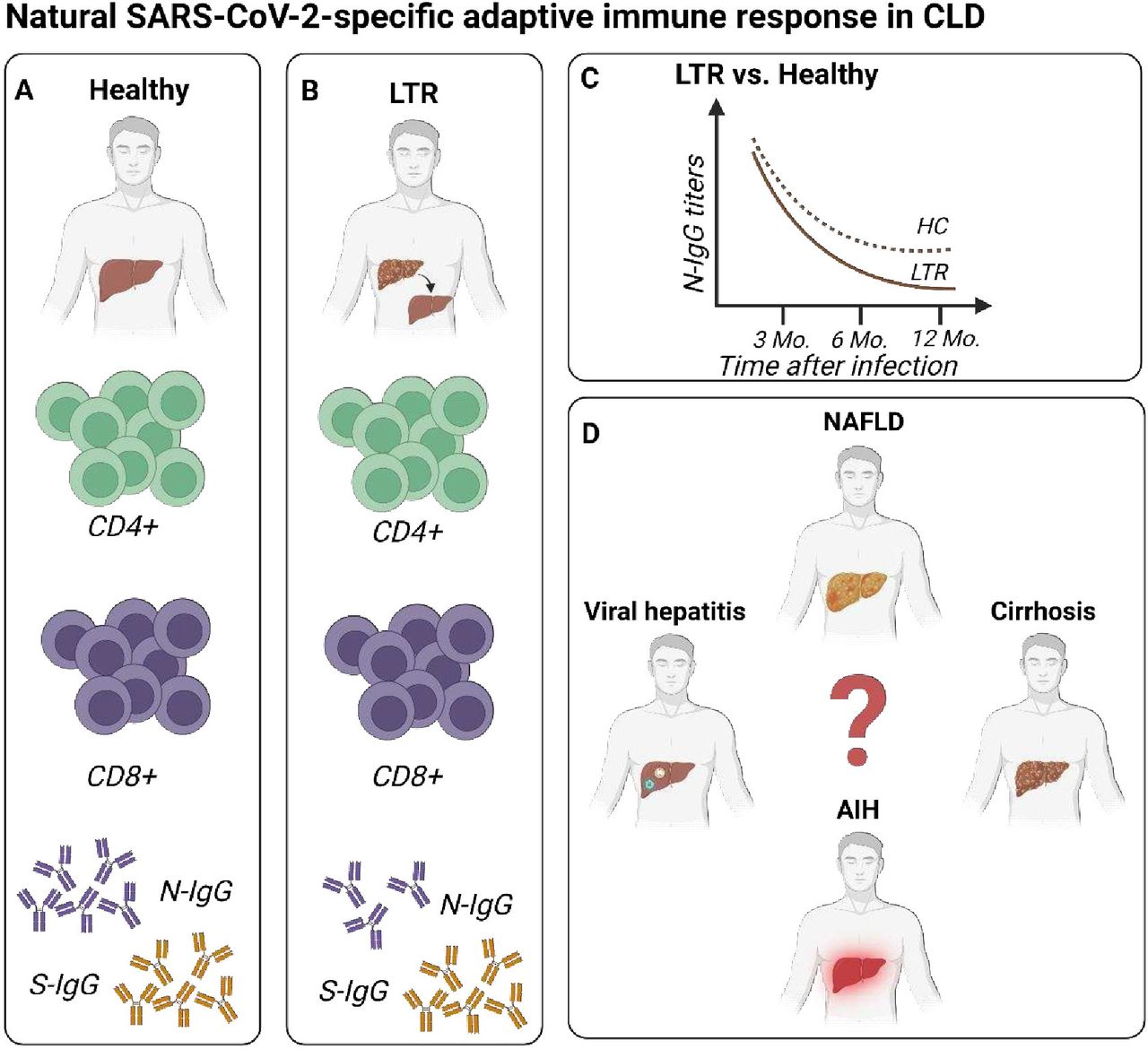
Overview of natural SARS-CoV-2-specific adaptive immune response in chronic liver disease (CLD) (A) Adaptive immune response in helathy individuals display strong CD4+ and CD8+ T cell responses as well as high tites of IgG targeting the nucleocapsid or spike protein. (B) Adaptive immune response in LTR show lower levels of N-IgG and S-IgG. The magnitude of CD4+ and CD8+ T cells is comparable in LTR and healthy individuals. (C) N-IgG titres are lower in LTR at 3 and 6 months and are accompanied by a faster decline in antibody titres compared with healthy controls. (D) The natural SARS-CoV-2-specific immune response has not been described in patients with cirrhosis, NAFLD, viral hepatitis or AIH. AIH, autoimmune hepatitis; HC, healthy control; LTR, liver transplant recipient; NAFLD, non-alcoholic fatty liver disease; N-IgG: nucleocapsid-specific immunglobulin; S-IgG, spike-specific Immunglobulin G.
SARS-CoV-2-specific adaptive immune response in CLD after infection
In contrast to healthy individuals, the knowledge of the natural SARS-CoV-2-specific immune response in patients with CLD is limited and focused on patients with cirrhosis and immunosuppressed LTR (figure 2B).
For patients with cirrhosis, preliminary data suggest a limited immunity following SARS-CoV-2 infection. A recent retrospective cohort study by John et al 95 compared 634 SARS-CoV-2-infected with 27 131 vaccinated (two doses of an mRNA vaccine) cirrhotic subjects and could demonstrate that infection-induced immunity is inferior to the vaccine-induced immunity and associated with a more severe course of infection. However, they did not measure T cell or antibody responses, highlighting the urgent need for further studies investigating the humoral and cellular immunity in this vulnerable cohort.
For LTR, however, several studies have investigated the adaptive immune response following SARS-CoV-2 infection and reported an impaired humoral immune response with reduced antibody levels in LTR compared with healthy controls.96–98 For example, Caballero-Marcos et al compared the nucleocapsid-specific and spike-specific IgG in LTR and observed significantly lower seroconversion rates for both nucleocapsid-specific and spike-specific IgG in LTR.96 97 Levels of nucleocapsid-specific IgG were lower in LTR at 3 and 6 months and were accompanied by a faster decline in antibody titres compared with healthy controls (figure 2C), whereas titres of IgG against spike protein were comparable in both cohorts over time.96 97 However, the cause of this discrepancy between IgG targeting nucleocapsid and spike protein is so far unknown. Further studies are needed to determine whether this disparity in antibodies may affect the risk of reinfection with SARS-CoV-2 and whether LTR with low levels of nuncleocapsid-specific IgG may benefit from prophylactic COVID-19 compared with those with high levels.
With respect to the cellular immune response, most LTR are able to develop T cell responses against the spike, nucleocapsid or membrane protein of SARS-CoV-2.99–101 Notably, the magnitude of T cell responses was comparable in LTR and healthy individuals and the cellular immune responses in LTR were longitudinally detectable and remained stable over 12-month postinfection99 100 (figure 2B). In a recent study, Citores et al performed a functional analysis of virus-specific CD4+ and CD8+ T cells 12 months after COVID-19 and observed a non-significant trend towards lower levels of IL2, IL10, TNF-α and IFN-γ in LTR compared with healthy individuals.101 Collectively, these data suggest a possible cell-mediated long-term protection despite the immunosuppression in LTR patients. In light of the European Association for the Study of the Liver (EASL) position paper,39 which recommends an individualised decision regarding dose reduction or discontinuation of immunosuppression in SARS-CoV-2-infected LTR, it is tempting to hypothesise that T-cell assays (eg, interferon-γ release assay102) may be helpful in these patients to evaluate adjustment of immunosuppressive treatment in case of SARS-CoV-2 (re-)infection. Since functional SARS-CoV-2-specific T cells prevent severe SARS-CoV-2 infection,11 LTR with strong T cell responses may benefit from an unchanged immunosuppressive regimen to minimise the risk of allograft rejection.
Taken together, studies investigating the cellular and humoral immune response in patients with CLD after SARS-CoV-2 infection are currently limited to LTR, however, studies investigating the immune response in other etiologies of CLD are urgently needed for a detailed understanding of the adaptive immunity in these patients (figure 2D).
SARS-CoV-2-specific adaptive immune response in CLD after vaccination
In contrast to the natural SARS-CoV-2-specific adaptive immune response, the vaccine-induced immunity has been described in more detail in patients with CLD with liver cirrhosis, AIH, NAFLD, viral hepatitis and after liver transplantation.
A recent meta-analysis demonstrated that seroconversion rates seem to be similar in patients with CLD compared with healthy individuals except for LTR.103 However, the antibody responses seem to be generally weaker. For example, patients with liver cirrhosis develop a virus-specific antibody response after vaccination with an inactivated virus, mRNA-based or vector-based vaccine, but the response is impaired compared with the general population with lower levels of spike-specific IgG104–106 (figure 3A,B). However, it is important to distinguish between compensated and decompensated cirrhosis. Studies investigating the vaccine-induced immune response in patients with cirrhosis following vaccination against other pathogens, such as HBV or influenza virus, suggest an impaired humoral immune response in decompensated cirrhosis.107 108 This is also the case for SARS-CoV-2, where the antibody response was particularly weak in decompensated patients104 106 109 (figure 3A,B). The impaired humoral immune response in these patients may be explained by an altered cytokine phenotype with higher levels of proinflammatory cytokines such as IL-2 or IL-6 in advanced cirrhosis.110 Basho et al could demonstrate that high levels of proinflammatory IL-2 lead to an impairment of TFH responses particularly in advanced cirrhosis.111 This is important since TFH cells play an essential role in T cell-mediated help to B cells by regulating the differentiation of B cells into plasma cells, which are responsible for the production of antigen-specific antibodies.112 They are also involved in the formation of memory B cells in germinal centres.112 However, it is likely that the hyporesponsiveness to COVID-19 vaccination may be overcome by booster vaccination, as shown in a large cohort of 26 082 patients with cirrhosis where a third dose of a mRNA vaccine was associated with an 80.7% reduction in COVID-19 emphasising the urgent need for booster vaccination in these patients.113

Overview of the vaccine-induced SARS-CoV-2-specific adaptive immune response in patients with chronic liver disease (CLD) (A) Adaptive immune response in helathy individuals has strong CD4+ and CD8+ T cell responses as well as high titres of IgG targeting the spike protein. (B) Reduced S-IgG and T cell responses in patients with cirrhosis, especially in a decompensated state. (C) Lower levels of S-IgG in NAFLD compared with healthy individuals, the cellular immune response has not described so far. (D) Lower levels of S-IgG in HBV-infected patients compared with healthy individuals, the cellular immune response has not described so far. (E) Reduced levels of S-IgG and reduced T cell responses in patients with AIH compared with healthy controls. (F) Reduced levels of S-IgG (induced by immunosuppression with MMF) and reduced T cell responses in LTR compared with healthy controls. AIH, autoimmune hepatitis; HBV, hepatitis B virus; LTR, liver transplant recipient; MMF, mycophenolate mofetil; NAFLD, non-alcoholic fatty liver disease; S-IgG: spike-specific Immunglobulin G.
For AIH, in a cohort of 103 patients and 125 patients with primary biliary cholangitis (PBC) or primary sclerosing cholangitis (PSC), antibodies were detectable in nearly all individuals after a second mRNA-based or vector-based vaccination.114 Interestingly, antibody responses were lower in AIH compared with PBC, PSC or healthy controls irrespective of the level of immunosuppression114 (figure 3A,C).
Comparable seroconversion rates have also been observed in NAFLD patients compared with healthy individuals. Indeed, Wang et al reported similar seroconversion rates of 95.5% in NAFLD patients who received an inactivated virus vaccine, compared with the general population.115 However, the subjects enrolled in this study were rather young, with a median age of 40 years, and lacked NAFLD-associated comorbidities such as diabetes mellitus and advanced CLD. This limitation was addressed in a recent study by Cheung et al who evaluated the humoral immune response in patients with moderate to severe steatosis and reported similar rates of seroconversion but lower antibody titres for both mRNA and inactivated virus vaccines compared with healthy individuals116 (figure 3A,D).
Data on the humoral immune response are also available for HBV-infected patients, where He et al observed the induction of an effective antibody response after administration of an inactivated COVID-19 vaccine117 (figure 3E). This response was increased when preceded by vaccination with an inactivated influenza vaccine.118 A possible explanation for this finding is trained immunity defined by the induction of a faster and greater response against a secondary challenge with homologous or even heterologous pathogens.119
The situation is somewhat different in LTR where Rabinowich et al analysed a cohort of 80 LTR and reported that the seroconversion rate after two doses of an mRNA vaccine was only 47.5% (vs 100% in healthy controls) with also significantly lower IgG titres compared with healthy controls (95.4 vs 200.5 AU/mL in healthy controls, p<0.001)120 (figure 3F). The study has the limitation of a younger age of the healthy controls compared with the LTR, however, a clear association of an impaired antibody response with older age, renal dysfunction and immunosuppressive medications could be observed.120 It appeared that MMF in particular has a negative effect on the humoral immune response.120 121 Thus, MMF represents a modifiable risk factor and prospective studies are needed to determine whether a temporary discontinuation of MMF before COVID-19 vaccination could be beneficial for the development of an adequate humoral immune response in the vulnerable cohort of LTR. This has already been shown in patients with immune-mediated inflammatory diseases under methotrexate therapy, where the discontinuation of the therapy 2 weeks before COVID-19 vaccination booster was associated with a significant boost of the humoral immune response compared with patients with continued immunosuppression.122
Analogous to the impaired antibody responses, patients with liver cirrhosis and especially those with decompensated cirrhosis show impaired virus-specific T cell responses after two doses of an SARS-CoV-2 vaccine106 123 (figure 3B). There is evidence that the combination of both, natural infection and vaccination, may induce a better immune response, so-called hybrid immunity.124 Indeed, this has recently been described in patients with cirrhosis after both infection and vaccination, with an enhanced cellular (and also humoral) immune response, including higher levels of IL-2 and IFN-γ, compared with vaccinated SARS-CoV-2 naïve cirrhotics.106 These results suggest that patients with CLD may particularly benefit from booster vaccination to increase SARS-CoV-2-specific immune responses.
Although NAFLD accounts for a high number of CLD, the cellular immune response induced by COVID-19 vaccine has not been investigated so far in this cohort (figure 3C). Thus, it remains an open important question whether impairments of T cell immunity contribute to the more severe course of disease in NASH patients as has been shown for the overall population.11 This hypothesis is, however, tempting since NAFLD patients display an imbalance of adipokines, for example, leptin and adiponectin, which has been shown to suppress T cell-mediated immune responses.125 In addition, peripheral immune cells from NAFLD patients exhibit differences in frequency and phenotype compared with individuals without NAFLD that are further aggravated during disease progression (reviewed in Lin and Fan126).
In contrast to NAFLD, information is available about the virus-specific T cell responses induced by COVID-19 vaccination in AIH patients. In particular, virus-specific T cell responses are detectable in about half of AIH patients following two doses of mRNA-based or adenovector-based vaccination, but were weaker compared with the general population or to patients with PBC or PSC114 (figure 3C). Although the study is limited by a small cohort size (n=20) and the lack of assessment of T cell functionality, the data nevertheless suggest that AIH patients may benefit from a booster vaccination to enhance the virus-specific T cell response.
LTR, as another immunosuppressed patient group besides AIH patients, similarly exhibit an impaired cellular immune response after two vaccine doses127–129 (figure 3F).For example, Reuther et al could observe a discordance between humoral and cellular immune responses in LTR with detectable T cell responses even in the absence of virus-specific antibodies.105 This is an important finding given that seroconversion rates are significantly lower in LTR after vaccination suggesting that these patients are nevertheless at least partially protected against a severe course of COVID-19 through virus-specific T cell responses.11 120
Influence of booster vaccination in patients with CLD
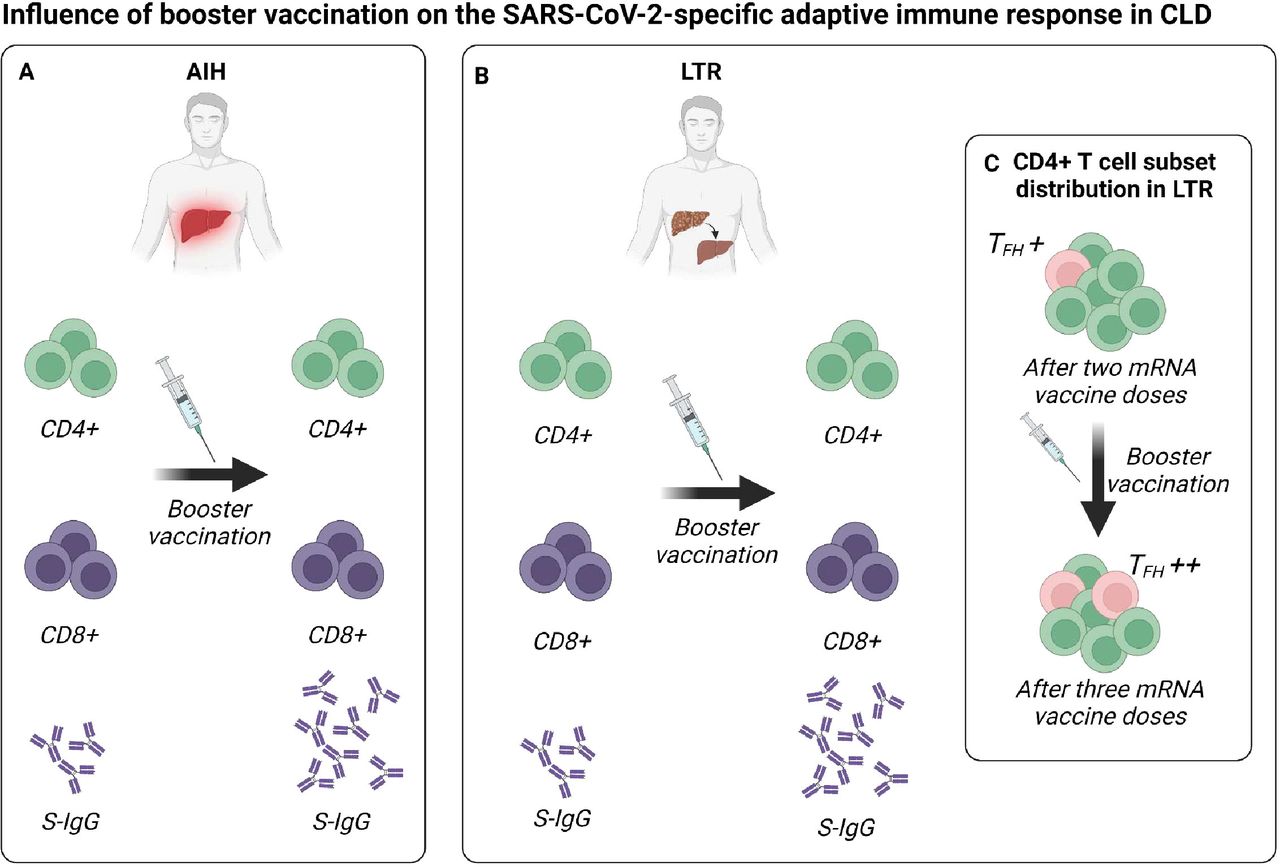
Booster vaccinations with a third and fourth vaccine dose are generally well tolerated and able to boost the virus-specific adaptive immune response in the general population.130 131 The impaired immune response in patients with CLD after vaccination raises the question whether these patients may therefore benefit particularly from booster vaccination. First studies have investigated this question in patients with AIH and LTR. Indeed, Hartl et al investigated the influence of a third mRNA-based or vector-based COVID-19 vaccination on the adaptive immune response in 81 AIH patients.132 Seroconversion was achieved in all AIH patients and antibody levels were significantly increased, especially in those with low antibody titres after the second vaccine dose, but titres were still lower compared with healthy controls132 (figure 4A). However, the magnitude of spike-specific T cells did not increase compared with the second vaccine dose132 (figure 4A). Thus, these data may support the concept of a fourth vaccination in this patient population, as the booster vaccination significantly improved at least the antibody response in those patients with a weak immune response prior to the booster vaccination.

Effect of booster vaccination on the adaptive immune response in LTR and AIH patients (A) Booster vaccination significantly improves the SARS-CoV-2-specific antibody response in LTR, while the frequency of T cells remains stable. (B) Booster vaccination significantly improves the SARS-CoV-2-specific antibody response in LTR, while the frequency of T cells remains stable. (C) After two mRNA vaccine doses, the CD4+T cell subset distribution is altered in LTR with lower frequencies of TFH cells, however, the frequencies increase after booster infection. AIH, autoimmune hepatitis; LTR, liver transplant recipients; TFH cells: T follicular helper cells.
Several studies have investigated the impact of a third127–129 or fourth127 129 mRNA vaccine dose on the adaptive immune response in LTR and could demonstrate a beneficial effect of booster vaccinations in these patients. For example, a recent work from our group compared CD4+ and CD8+ T cell responses after up to four doses of an mRNA vaccine in LTR and healthy individuals in more detail.129 We observed a reduced breadth of spike-specific CD8+T cell responses after three vaccine doses in the cohort of LTR, however, the detected CD8+T cell epitopes were largely conserved in SARS-CoV-2 variants of concern including BA.1, BA.4/5 or BQ.1.129 We also observed significantly reduced frequencies of spike-specific CD8+T cells in LTR versus healthy controls with lower expression of CD38 and T-BET suggesting a reduced activation capacity of SARS-CoV-2-specific CD8+T cells.129 While the humoral immune response could be improved by a third vaccine dose in LTR, the frequency of spike-specific CD8+T cells remained stable in the majority of LTR129 (figure 4B). However, despite the overall reduced number and frequencies of SARS-CoV-2-specific CD8+T cells, the formation of a CD8+T cell memory pool appeared to be intact in LTR and comparable to that in healthy controls.129
In contrast to virus-specific CD8+T cells, the epitope repertoire of CD4+T cells was similar in LTR and healthy individuals after three mRNA vaccine doses.129 However, subset distribution of CD4+T cells was altered after the second vaccine dose, with lower frequencies of TFH cells in LTR. Analogous to TFH cell frequencies, neutralising capacity of the antibodies directed against the omicron variant (BA4/5) increased significantly after the third vaccine shot.129 Thus, since booster vaccination increased the frequency of TFH cells in LTR increased and since this occurred in parallel with the improvement of the humoral immune response129 (figure 4C), these results clearly underline the need for booster vaccination in the vulnerable group of LTR.
In conclusion, and in accordance with the recommendation of the EASL,131 patients with CLD benefit from prophylactic vaccination against SARS-CoV-2. Although the effect of booster vaccinations on the immune response is uncertain in some etiologies of CLD AIH patients and LTR show an improved immune response after administration of a third and fourth vaccine dose.
Vaccine-induced hepatitis
COVID-19 vaccination is associated with some rare severe side events, such as myocarditis, vasculitis or vaccine-induced immune thrombotic thrombocytopenia.133 For example, in Germany, a total of 331 900 suspected adverse events have been reported by October 2022, representing 1.29 reports per 1000 vaccinations administered.134
Recently, also some rare cases of liver injury have been described after SARS-CoV-2 vaccination135–139 and the symptoms of the vaccine-induced liver injury range from elevated liver enzymes to acute liver failure.139 The pathophysiological mechanisms are not fully understood, however, several mechanisms such as molecular mimicry, vaccine adjuvants, bystander hepatitis or direct mRNA effects are suspected to be involved in the development of this immune-mediated liver injury (reviewed in Trontzas et al 136). In a cohort of 470 274 individuals, 177 (0.038%) without pre-existing liver disease developed liver injury after the first or second dose (mean time 29±21 days and 45±25 days, respectively), with most cases of vaccine-induced liver injury occurring after the second dose.140
For diagnosis, exclusion of other causes of liver damage is essential. Of note, the reported cases of liver injury following SARS-CoV-2 vaccination were mild and most cases improved spontaneously or after administration of steroids.135 137 141 With this in mind, physicians should always consider a vaccine-induced liver injury if liver enzymes are abnormal following COVID-19 vaccination. As a result, further vaccination needs to be avoided or a change in vaccine regimen should be considered.
The first case of a vaccine-induced autoimmune-like hepatitis (ALH) has been described by Bril et al 142 who reported pruritus and jaundice in a woman after receiving a first dose of the BNT162b2 mRNA vaccine. antinuclear antibodies (ANA) and double-stranded DNA antibodies were positive, however, liver biopsy revealed a picture compatible with an AIH. Of note, the presence of autoantibodies such as ANA, smooth muscle antibodies (SMA) and, to a lesser extent, anti-mitochondrial antibodies is a common feature in patients with ALH141 143 144 (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
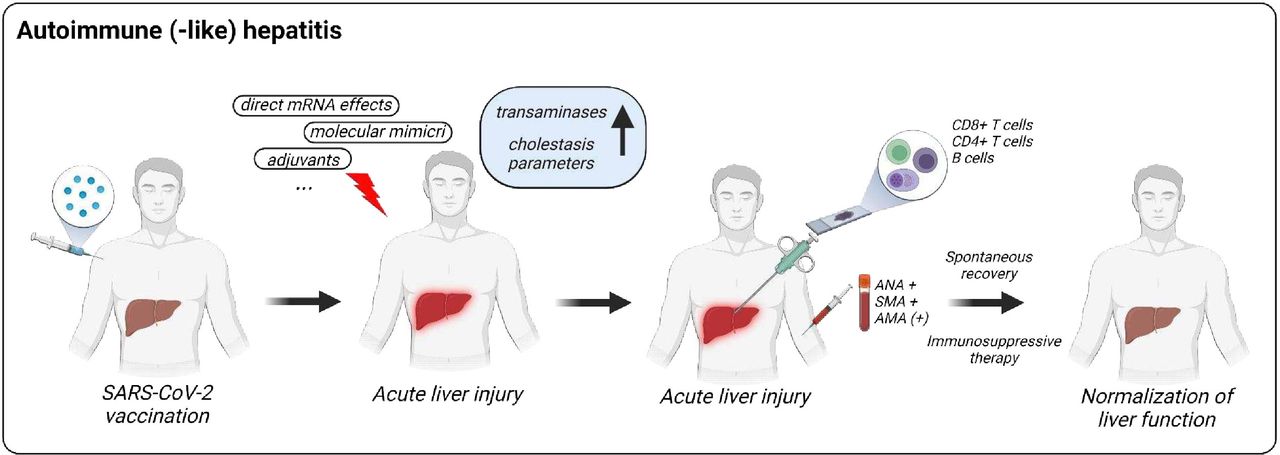
Overview of the autoimmune (-like) hepatitis following COVID-19 vaccination. COVID-19 vaccines can cause liver injury by different mechanism such as molecular mimicry, vaccine adjuvants or direct mRNA effects. This autoimmune (-like) hepatitis (ALH) is frequently associated with the presence of autoantibodies (ANA, SMA, AMA) and virus-specific immune-cells in the liver. ALH generally recovers spontaneously or after immunosuppressive therapy. AMA: anti-mitochondrial antibodies; ANA, anti-nuclear antibodies; SMA, smooth muscle antibodies.
Since the first description by Bril et al,142 many cases of ALH have been reported after vaccination with mRNA-based, vector-based, protein-based and inactivated SARS-CoV2 vaccines.133 For example, a recent study by Codoni et al investigated autoantibodies and histological features in liver injury with autoimmune features following COVID-19 vaccination in a cohort of 59 individuals without preexisting liver disease.141 Similar to the case described by Bril et al,142 autoantibodies were frequently positive, for example, ANA in 74% and SMA in 64% of the patients. Liver histology revealed a lobular injury in most patients (76%) with lymphocytic infiltration, focal necrosis and acidophilic bodies. They reported a significant improvement of serum transaminases after initiation of steroid treatment with a normalisation reached in the majority of ALH cases within 6 months.141 The treatment decision was made without a standardised protocol and according to local standards at the respective centre. However, when re-exposed to COVID-19 vaccine 3/15 individuals exhibited a relapse.141
For a more detailed immunological understanding of vaccine-induced ALH, we performed immune profiling in a 52-year-old man with two episodes of acute hepatitis 2–3 weeks after BNT162b2 mRNA vaccination.145 We observed an infiltration of activated cytotoxic SARS-CoV-2-Spike specific CD8+T cells in the liver accompanied by an enrichment of CD4+T cells, B cells, plasma cells and myeloid cells (figure 5). CD8+T cells expressed high levels of activation and cytotoxicity markers in concert with elevated liver enzymes. However, treatment with steroids in combination with ursodeoxycholic acid led to a normalisation of liver enzymes within 8 weeks.
COVID-19 vaccines have also been suspected to cause cholangiopathy. Zafar et al reported the case of a 51-year-old man with the occurrence of fatigue, malaise and jaundice after vaccination.146 Blood tests showed abnormal liver function with predominantly elevated cholestatic parameters and MR cholangiopancreatography revealed bile duct strictures and irregularities typically found in PSC suggesting that COVID-19 vaccination may also induce immune-related cholangiopathy in some individuals.
Overall, liver damage caused by COVID-19 vaccination is a rare side effect. However, the advantages of SARS-CoV-2 vaccination clearly outweigh the risks for liver injury.147 If transaminases and cholestasis parameters are elevated after SARS-CoV-2 vaccination, physicians should suspect a vaccine-induced effect. These patients require close monitoring as liver injury may progress to acute liver failure. In addition, they will likely require immunosuppressive therapy, under which liver function tests will generally normalise.
Conclusion
SARS-CoV-2 infection can have an influence on the liver in healthy individuals as well as in patients with CLD. This is highly relevant for the daily clinical routine since liver injury in SARS-CoV-2 might aggravate the clinical course of infection also resulting in the necessity for close monitoring of these patients. This is also true for LTR and patients with CLD and especially those with cirrhosis, in whom SARS-CoV-2 infection can be more severe compared with the general population. Thus, patients with CLD in particular benefit from a prophylactic vaccination. Relevant aspects of how SARS-CoV-2 infection and vaccination affect the liver can be summarised as follows:
First, acute liver injury occurs in many cases of SARS-CoV-2 infection and may be related to, for example, induction of cytokines, direct viral infection of bile duct cells and hepatocytes, toxic effects of COVID-19 agents or the infiltration of different immune cell subsets.
Second, COVID-19 may have a more severe course and promote decompensation in individuals with underlying liver disease and particularly in patients with cirrhosis.
Third, compared with healthy individuals, SARS-CoV-2-specific humoral and cellular immune responses are impaired in patients with CLD during both, natural infection and vaccination. Importantly, booster vaccination may at least partially improve these impaired immune responses.
Finally, th development of ALH is a rare side effect of COVID-19 vaccination that should be included in the differential diagnosis of elevated liver enzymes.
Bullet points
Clinical features of COVID-19 in patients with CLD and healthy individuals
In healthy subjects, acute liver injury affects more than a third of hospitalised subjects infected with SARS-CoV-2.
Liver injury during SARS-CoV-2 infection can be multifactorial including systemic inflammation, intrahepatic immune activation, hypoxaemia, microvascular thrombosis and drug toxicity.
In liver cirrhosis, SARS-CoV-2-associated mortality is higher in patients with decompensated cirrhosis compared with patients with compensated cirrhosis.
In LTR, immunosuppression with MMF is associated with severe COVID-19.
Immunological features of COVID-19 in patients with CLD
SARS-CoV-2 infection and vaccination induce a strong humoral and cellular immune response in healthy individuals.
Weak immune responses in patients with CLD present after two doses of a COVID-19 vaccine can be improved by booster vaccination.
Cellular and humoral immune responses are also impaired after two doses of vaccination in patients with decompensated liver cirrhosis and LTR, however, can be increased by booster vaccination.
Induction of ALH following COVID-19 vaccination
ALH represents a rare side events of COVID-19 vaccination.
Autoantibodies are frequently present in patients with ALH.
In ALH an enrichment of CD4+T cells, B cells, plasma cells and myeloid cells can be observed in the liver.
Treatment with steroids improves liver function tests in ALH.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank Drs Maike Hofmann and Christoph Neumann-Haefelin for critical proof-reading.
References
Footnotes
Contributors Conceptualisation, investigation and writing: HL and RT; funding acquisition: HL and RT. All authors have read and agreed to the published version of the manuscript.
Funding This study was supported by grants from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation; 272983813 and 256073931 to R.T.). This work was also supported by the project “Virological and immunological determinants of COVID-19 pathogenesis – lessons to get prepared for future pandemics (KA1-Co-02 “COVIPA”)”, a grant from the Helmholtz Association’s Initiative and Networking Fund (to R.T.). H.L. is supported by the IMM-PACT-Programme for Clinician Scientists, Department of Medicine II, Medical Center – University of Freiburg and Faculty of Medicine, University of Freiburg, funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation, 413517907). The funding bodies had no role in the decision to write or submit the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.