Article Text

Abstract
Patients with inflammatory bowel disease (IBD) remain at increased risk for colorectal cancer and death from colorectal cancer compared with the general population despite improvements in inflammation control with advanced therapies, colonoscopic surveillance and reductions in environmental risk factors. This guideline update from 2010 for colorectal surveillance of patients over 16 years with colonic inflammatory bowel disease was developed by stakeholders representing UK physicians, endoscopists, surgeons, specialist nurses and patients with GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodological support.
An a priori protocol was published describing the approach to three levels of statement: GRADE recommendations, good practice statements or expert opinion statements. A systematic review of 7599 publications, with appraisal and GRADE analysis of trials and network meta-analysis, where appropriate, was performed. Risk thresholding guided GRADE judgements.
We made 73 statements for the delivery of an IBD colorectal surveillance service, including outcome standards for service and endoscopist audit, and the importance of shared decision-making with patients.
Core areas include: risk of colorectal cancer, IBD-related post-colonoscopy colorectal cancer; service organisation and supporting patient concordance; starting and stopping surveillance, who should or should not receive surveillance; risk stratification, including web-based multivariate risk calculation of surveillance intervals; colonoscopic modalities, bowel preparation, biomarkers and artificial intelligence aided detection; chemoprevention; the role of non-conventional dysplasia, serrated lesions and non-targeted biopsies; management of dysplasia, both endoscopic and surgical, and the structure and role of the multidisciplinary team in IBD dysplasia management; training in IBD colonoscopic surveillance, sustainability (green endoscopy), cost-effectiveness and patient experience. Sixteen research priorities are suggested.
- COLORECTAL CANCER SCREENING
- COLORECTAL NEOPLASIA
- ENDOSCOPY
- COLONOSCOPY
- IBD
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Executive summary
General principles and methods
These guidelines update the 2010 inflammatory bowel disease (IBD) surveillance guidelines, the SCENIC 2015 consensus, which were part of the combined recommendations in the 2019 BSG IBD guidelines. Updated GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodology was used, including a priori risk thresholding and evidence to decision frameworks, with new systematic reviews and Delphi consensus voting. There was a specific focus on using modern data and risk estimates as the risk of IBD-associated colorectal cancer (CRC) has changed significantly over time. A principle of shared decision-making with patients regarding their care is emphasised throughout. The guidelines relate to colorectal surveillance for patients with colonic IBD, aged 16 years or older. Figure 1 summarises the full guideline IBD surveillance pathway.

Infographic summarising full guideline IBD surveillance pathway.
Epidemiology
The risk of CRC and of death remain elevated at 1.4–1.7 times that of the non-IBD population. Although this is significantly lower than previous estimates, it is sufficiently high for patients with IBD to be considered for surveillance. Colonoscopic surveillance reduces the risk of developing and of dying from CRC, primarily by detecting CRC at an earlier stage. Post-colonoscopy CRC rates are sixfold higher than for sporadic CRC, which may reflect difficulties in detection and faster biology; however, some of this difference is due to methodology. Concordance with appropriate surveillance intervals is low, and IBD surveillance services need to implement systems to improve this, including patient education.
Risk stratification
Risk is not evenly distributed in the population with IBD. Patients should have colonoscopy at 8 years after symptoms, or immediately if they have primary sclerosing cholangitis (PSC), to determine risk factors. Surveillance intervals can be determined via classic single highest risk factor methods or via a multivariate risk calculator that potentially offers more precise and personalised risk (https://ibd-dysplasia-calculator.bmrc.ox.ac.uk). Those at population level risk should receive population based CRC screening, with reassessment with colonoscopy every 10 years. For patients with consecutive colonoscopies without inflammation detected, or who have significant comorbidities, or who reach age 75, ongoing surveillance can be reviewed. 5-Aminosalicylates (5-ASAs) may have a chemopreventive effect.
Colonoscopy
Bowel preparation is important to patient experience. A low volume of polyethylene glycol (PEG; 2 L) is recommended rather than 4 L, and oral sulfate and picosulfate-based preparations appear to be as effective as 2 L PEG, increasing choice. High-definition colonoscopes are recommended. Dye-based chromoendoscopy is suggested as it offers a small benefit over high-definition white light for dysplasia detection. No recommendation was possible for virtual chromoendoscopy. Computer-aided detection (artificial intelligence) and biomarkers are not yet ready for clinical implementation in IBD surveillance pathways.
Pathology
Non-conventional dysplasia should be considered alongside conventional dysplasia by pathologists reporting on IBD specimens. Double reporting is recommended for dysplasia cases. Serrated lesions comprise a subset of non-conventional dysplasia, but non-dysplasic serrated lesions are not considered IBD-associated CRC precursors, and should be managed as if sporadic. Serrated epithelial change (SEC) should not increase surveillance frequency. In high-risk cases—for example, previous dysplasia or PSC, quadratic non-targeted biopsy specimens should be taken every 10 cm, or from each colonic segment, in addition to targeted biopsies.
Surveillance
When dysplasia is detected within the colitis segment, all patients should be reviewed at an IBD multidisciplinary team (MDT) meeting. Most dysplasia is resectable endoscopically, ideally en bloc, and subsequently most patients will receive endoscopic surveillance. Surgery is reserved for endoscopically non-resectable dysplasia, high-risk multifocal or invisible dysplasia, dysplasia with other risk factors, CRC or where surveillance is not effective or possible. Segmental resection might be an option in carefully selected cases. Patients with an ileoanal pouch or a retained rectum might require surveillance if they have risk factors.
Quality, training, sustainability and cost effectiveness
There is a need to develop training programmes to support IBD endoscopists to acquire the skills necessary for this role, and audit their performance. Auditable outcomes for IBD endoscopists include: use of high-definition, dye-chromoendoscopy; validated activity scores and quality of bowel preparation. Auditable outcomes of IBD surveillance services include: rates of MDT review after dysplasia detection, and offers of timely surveillance intervals. Patient-reported outcome measures should be collected periodically to improve patient experience. Targeted biopsy strategies might reduce CO2 emissions, but this might be offset by improved concordance with surveillance. Colonoscopic IBD surveillance is probably cost effective at National Institute for Health and Care Excellence (NICE) thresholds.
Patient-friendly summary: IBD colorectal surveillance
Inflammatory bowel disease includes conditions like Crohn’s disease or ulcerative colitis (often shortened to colitis). People with IBD in the large bowel, or colon, may be around twice as likely to develop bowel cancer than the general population. But the risk of developing bowel cancer is still low.
Bowel cancer is also known as colorectal cancer. Over the past 20 years, the number of people with Crohn’s disease or colitis who have developed this type of cancer has fallen. This might be due to better medicines that control inflammation and improved tests that detect bowel cancer early.
The risk of developing bowel cancer may depend on:
How long you have had IBD.
Which part of the bowel is affected.
The level of inflammation you have had since symptoms started.
Other conditions, such as primary sclerosing cholangitis (this is a rare condition that causes inflammation of the bile ducts and can eventually damage the liver).
Not everyone who has IBD will have an increased risk of bowel cancer. To determine this risk, we recommend that:
All patients have a colonoscopy around 8 years after their symptoms started.
Any patients with primary sclerosing cholagitis have a colonoscopy at diagnosis.
This colonoscopy is called a surveillance colonoscopy, and is a ‘check-up’ to look for any precancerous changes (called dysplasia) in the lining of the bowel. These changes might suggest a higher risk of bowel cancer.
After the first surveillance colonoscopy, some patients might not need further colonoscopies. This is because their risk of bowel cancer will be similar to that of people without IBD. Most patients are likely to be offered regular colonoscopies. This allows specialists to check for early changes in the lining of the bowel before cancer develops.
Colonoscopy is the best way to find bowel cancer early and help prevent it. The earlier bowel cancer is found, the more likely it is that it can be treated.
Sometimes cancer or precancerous changes can be missed during a colonoscopy. This might happen because:
It is not always possible to reach the entire bowel during a colonoscopy.
The bowel preparation might not have cleaned the bowel enough to see the cancer or dysplasia.
Ongoing bowel inflammation might make it difficult to see the cancer or dysplasia.
In some cases, a polyp might not have been removed fully, so cancer later develops.
Your IBD team should discuss your risk of bowel cancer with you regularly. This is especially important as you get older, particularly as the amount of time you have had IBD increases.
If a precancerous change or a cancer is discovered, your IBD team will discuss your options with you, and help to come up with a treatment plan. Most precancerous changes can be removed at the time of colonoscopy, much like removing polyps. If there are multiple or advanced areas of precancerous change or cancer, then your IBD team might advise you about surgery to remove part or all of the bowel.
Patients who have a pouch or have had most of the large bowel removed, but still have the lower part of the bowel (called the rectum), might also need regular procedures.
Repeated colonoscopy can be difficult for patients. Special effort should be made to make you as comfortable as possible. Your procedures should be carried out by endoscopists with experience of IBD surveillance. They will have the techniques needed to identify and deal with precancerous changes. They will also perform the procedures with enough sedation and time to ensure a comfortable examination. New options for bowel preparation are available for patients with IBD, and might make bowel cleansing before the procedure more tolerable. Endoscopy units should regularly ask you for feedback about your experience of surveillance colonoscopies. This will help them to improve the service they offer.
Introduction
The British Society of Gastroenterology’s (BSG) last guideline on colonoscopic surveillance in inflammatory bowel disease (IBD) was published in 2010.1 In 2019 the BSG published surveillance guidance within the main consensus IBD guidelines,2 which added in the recommendations of the SCENIC 20153 guidelines, which mainly dealt with detection of dysplasia and its management; however, neither extensive systematic review nor consensus voting was performed.
As the 2019 guidance2 notes, the incidence of CRC in patients with IBD has fallen significantly over time, which might reflect the introduction of drugs that control inflammation more effectively, implementation of surveillance strategies, reduction in modifiable risk factors, such as smoking, or the changing approach to maintenance therapy or colectomy.
The BSG Clinical Services and Standards Committee have commissioned the BSG endoscopy section to update the 2010 guidelines,1 to those which include comprehensive systematic review and consensus voting. The Guideline Development Group (GDG) therefore set out with the explicit aim of using up-to-date population-based estimates of IBD CRC risk that reflect modern IBD practice, where possible, adjusted for other risk factors. Furthermore, the GDG included current GRADE methodology to maximise transparency in the guideline development process, and critically, required explicit risk thresholding to determine clinically important effect sizes before data review.
The guideline considers surveillance for ulcerative colitis, Crohn’s colitis and unclassified IBD with colonic involvement, but not microscopic colitis where CRC risk is not increased above population risk,4 for patients aged over 16 years. Evidence for colonoscopy and biomarkers was reviewed, but radiological techniques—for example, CT colonography and capsule colonoscopy, were not examined.
This document aims to offer high-quality, evidence-based guidance to clinicians and patients with IBD to make patient-centred informed decisions on whether and how to undergo surveillance to detect early, and prevent, colitis-associated CRC, and to promote and inform best practice. It is designed to be read as a companion to the main IBD guidelines, which deal with other aspects of IBD clinical care.5
These BSG guidelines represent a consensus of best practice based on the available evidence at the time of preparation. They may not apply in all situations and should be interpreted in the light of specific clinical situations and resource availability. Further controlled clinical studies might be needed to clarify aspects of these statements, and revision may be necessary as new data appear. Clinical consideration might justify a course of action at variance to these recommendations, but we suggest that reasons for this are documented in the medical record. BSG guidelines are intended to be an educational device, to provide information that might assist in providing care for patients. They are not rules and should not be construed as establishing a legal standard of care or as encouraging, advocating, requiring, or discouraging any particular treatment.
Methods
The methodology and operating procedures for this guideline were devised in line with BSG procedures. They were agreed and submitted for peer review publication before completion of the guideline.6 Therefore, full details of the methods will not be given in this manuscript, but a summary is included below for quick reference.
The development of this guideline is in line with key international procedural documents, including the procedures of the GRADE approach as laid out in the GRADE handbook,7 supported by the WHO handbook for guideline development.8 The GDG used the GIN-McMaster guideline development checklist, an 18-point process map to support the steps in a GRADE-compliant guideline development process.9 10
During the planning and scoping search phase of the guideline, it was apparent that a number of core thematic questions would not be conducive to GRADE recommendations, owing to the lack of randomised controlled trial (RCT) data. Therefore, guidance was employed to guide the production of good practice statements (GPS) in such cases, if the appropriate criteria were met. Finally, for statements that did not meet the criteria for either, these were to be defined as expert opinion statements.11 These statement types are shown in figure 2.

Infographic summarising guideline statement types and risk threshold development. GDG, Guideline Development Group; GRADE, Grading of Recommendations Assessment, Development and Evaluation; PEG, polyethylene glycol.
Organisation, planning and training
In March 2022, the BSG appointed a content and field expert guideline chair. In line with core guidance, a non-voting GRADE and synthesis methodologist was appointed as co-chair.12
Members were selected based on content expertise, UK experience, research contribution and representation of the wider stakeholder community. Additionally, two patient members who were approached through Crohns and Colitis UK (CCUK) joined, together with CCUK representation. All GDG members were invited to take part in voting where they felt they had sufficient expertise (except the methods team), unless they had confilcts of interest.
The two chairs and other GDG members attended a bespoke GRADE training workshop through a collaboration with Professor Schünemann and Dr Miranda Langendam at the Department of Epidemiology and Data Science, Amsterdam University Medical Centres, University of Amsterdam, Netherlands, in November 2022, which had been organised as part of the separate wider BSG IBD guideline. The wider GDG group completed three bespoke online workshops offered by MG (meta-analysis, risk of bias, GRADE decision-making and evidence to decision frameworks).
Thematic/PICO question generation and scope
The generation of new questions occurred through a cyclical and iterative process with the GDG, using the BSG 20101 and SCENIC 20153 guidelines as a baseline. Core topics were proposed, and a topic lead assigned. The chairs together with topic leads produced individual questions within each area. Then, the wider group reviewed and amended these questions.
A categorisation process was completed. This defined Problem/Population; Intervention; Comparison; Outcome (PICO) questions, where possible, and identified their likely use of a GRADE approach to recommendations. For a number of key areas where a PICO question could not be developed, a framework for informing qualitative questions, CAPS (Current state of knowledge, Area of interest, Potential impact, Suggestion from experts in the field), was employed.13
Technical review process
The core methodological team ran searches for evidence in all areas where PICO questions had been devised. These were produced with an information specialist with significant guideline and Cochrane expertise. The searches were run in four phases: a search for papers of all relevant designs for IBD surveillance screening; a second search targeting bowel preparation; a third, targeting surveillance modalities and a fourth, targeting artificial intelligence.
A total of 7599 citations were considered through title screening, and a final sample of 140 full texts were included. The central team performed screening, in duplicate, of all full texts, and these were then categorised into the relevant PICO question theme area for further review and consideration, with some studies contributing to multiple areas.
Thresholds of outcome measures
Key to guideline decision-making is to conceptualise the balance of positive and negative outcomes that considers magnitude.14 15 Therefore, developing explicit thresholds for interpretation of effect sizes of outcomes is also a vital step in this transparent decision-making process,16 as well as supporting judgements on imprecision17 in a more precise fashion than a dichotomous minimal clinically important difference.18
Although these exercises have been well deployed in interventional outcomes,19 the approach is less commonly used when considering risk. Paradoxically, risk, by its nature, supports the concept of thresholds, and previous guidelines in this context internationally discuss bands of risk and various resulting actions.1–3 20
We deployed several Delphi approaches across the GDG membership online before analysis began.6 Each expert was asked to select important clinically relevant outcomes and to categorise the size of the magnitude of the effects in line with GRADE guidance, which proposes the following categories: large, moderate, small, or trivial for each core outcome. Additionally, a novel thresholding exercise was used to define ‘risk’ rather than outcome categories. Questions were framed as neutral statements, without introducing a specific direction. After a first round, main areas of convergence and divergence were calculated, and a second round run to reach consensus. The final thresholds were presented to, and agreed by, the GDG. The final agreed thresholds, as well as a summary of the types of statements in the guideline, are shown in figure 2.
Section 1: Epidemiology
1.1 Expert opinion: People with colonic IBD, on average, are at higher risk of developing CRC than the general population. People with colonic IBD have an increased risk of death from CRC compared with the general population.
The relative risk of CRC incidence in people living with ulcerative colitis (UC) and Crohn’s disease affecting the colon is, on average, higher than that of the background population. A recent meta-analysis of 20 population studies, and subsequent Scandinavian population-based data, have identified a CRC relative risk of approximately 1.4–1.7.21–23 This higher incidence is despite observations of CRC diagnoses in IBD declining with time,22 24 25 which might reflect better endoscopic surveillance and improved control of inflammation with effective advanced treatments (online supplemental tables A and B).21–35 This risk exceeds the predetermined risk threshold of 1.5-fold risk of CRC for patients with IBD compared with that of the general population, determined by the GDG as the level at which colonoscopic surveillance for patients with IBD would be appropriate.
Supplemental material
The mortality risk from CRC is higher in those with IBD than the general population when adjusting for tumour stage with a HR of approximately 1.4–1.5.22 23 This increased incidence and mortality risk has persisted post-201025 in the era of advanced therapies for IBD and technological development in lower gastrointestinal endoscopy.
Several cohort studies have identified a high incidence of CRC in the first year after diagnosis of IBD; however, this might reflect detection bias—that is, that increased investigation when IBD is diagnosed might lead to greater cancer detection or vice versa.22 24 33 Overall, the cumulative risk of CRC in IBD increases with duration of disease, at 0.8% within the first 10 years, 2.2% between 10 and 20 years and 4.5% at >20 years.34 Anal cancers, while rare, are associated with Crohn’s disease and also UC.31 36
1.2 Does colonoscopic surveillance in IBD prevent death from CRC, or the development of CRC?
1.2a GRADE: We recommend colonoscopic surveillance in patients with colonic IBD, as it might reduce the development of CRC and the rate of CRC-associated death through early detection.
A Cochrane review of five observational studies with 7199 patients assessed the effectiveness of colonoscopic surveillance in IBD.37 Findings indicated lower cancer detection rates in surveillance groups compared with those not undergoing surveillance (OR=0.58, 95% CI 0.42 to 0.80). Early-stage CRC detection (Duke stages A and B) was higher in the surveillance group (OR=5.40, 95% CI 1.51 to 19.30), whereas late-stage CRC (Duke stages C and D) was more frequent in the non-surveillance group (OR=0.46, 95% CI 0.08 to 2.51). CRC-associated death rates were lower in the surveillance group (OR=0.36, 95% CI 0.19 to 0.69).
We updated the search up to September 2023. Additional studies support these findings. Narula et al found that patients with UC who had regular colonoscopies had lower rates of high-risk CRC (44.4% vs 77.4%; p<0.05).38 Cole et al showed that adherence to surveillance guidelines decreased the risk of advanced-stage CRC (adjusted OR=0.20, 95% CI 0.05 to 0.85).39 Hata et al reported better 5-year survival rates for patients undergoing surveillance (88.9% vs 69.8%).40 Kim et al linked more frequent colonoscopies to earlier CRC detection and better survival outcomes.41
Despite promising outcomes, the evidence quality is very low according to ROBINS-I42 due to observational study biases, variations in reported outcomes and surveillance intervals, which could not be combined for an updated meta-analysis and GRADE assessment.(online supplemental tables C and D).38–41 43–47 Given the ethical challenges of conducting RCTs, where patients are randomised to surveillance or not, a shared decision-making approach, where individual patient factors and preferences are considered to guide surveillance strategies for patients with IBD, is warranted.
1.3 Post-colonoscopy colorectal cancer (PCCRC) in IBD: measurement, reporting and reduction
1.3a Expert opinion: The PCCRC rate in patients with IBD is substantially higher than in patients without IBD, although there are methodological problems which hamper interpretation of this difference.
Two meta-analyses report IBD-PCCRC rates,48 49 using World Endoscopy Organization methodology.50 Both meta-analyses note a high degree of heterogeneity among studies. The meta-analyses include population-based data on all colonoscopy for IBD and are unable to differentiate between true surveillance and a non-surveillance procedure, and therefore may not reflect an optimised procedure to detect dysplasia or cancer.
A meta-analysis by Scotti et al49 was specific to IBD-PCCRC and was based on three retrospective observational cohort studies.51–53 The pooled IBD-PCCRC 3-year rate was 30.8% (95% CI 24.4% to 37.5%), and in patients without IBD it was 6.8% (95% CI 6.2% to 7.4%). The PCCRC 3-year rate was significantly higher in patients with IBD than in patients without IBD (OR=6.04; 95% CI 4.04 to 9.4). Patients with ulcerative colitis had a significantly higher PCCRC rate than patients with Crohn’s disease: 30.9% (95% CI 27.8% to 34.2%) vs 22.3% (95% CI 18% to 27%), respectively (OR=1.6, 95% CI 1.2 to 2.2).
A meta-analysis by Kader et al48 reports a pooled IBD-PCCRC 3-year rate of 29.3% (95% CI 21.3 to 38.1%), sixfold higher than in patients without IBD (OR=6.17, 95% CI 4.73 to 8.06), based on three studies.51 52 54
It should be noted that there are methodological issues with using PCCRC 3-year rates in IBD, as many patients will be undergoing regular surveillance colonoscopies, and hence a CRC detected on one surveillance colonoscopy is likely to be a PCCRC relating to the previous surveillance colonoscopy. Given that early-stage detection of CRC on IBD surveillance might still be considered a surveillance success, due to the often-rapid IBD CRC pathway progression, we suggest that more refined PCCRC rate analyses are studied in future, either using PCCRC 1 year rates or taking CRC stage into account.
1.3b Expert opinion: Root cause analysis of IBD-PCCRCs has identified several contributory factors, including rapid progression to cancer, ineffective surveillance algorithms, poor concordance with surveillance intervals (whether patient-, clinician- or administrator-derived), and specific endoscopic challenges, such as discriminating subtle neoplasia from IBD mucosa, and incomplete neoplasia resection.
Gordon et al55 found that in 54% (42 of 78) of patients with IBD-associated CRC who were eligible for CRC surveillance, 12% were detected at the recommended surveillance time (non-interval type A PCCRCs); 10% were detected after the recommended surveillance date (non-interval type B PCCRCs); and 14% were detected before the recommended surveillance date (interval-type PCCRCs). An opportunity for colonoscopic surveillance was missed by 64% of patients, of whom, 10/27 secondary care patients and 17/27 primary care patients had not been offered surveillance. In four patients, inadequacy of previous colonoscopies and/or failure to consider previous histological findings were contributory factors.
Kabir et al56 found that 78% of IBD PCCRCs developed in high-risk patients requiring annual surveillance, but 57% had delayed surveillance. Underlying causes for PCCRCs included endoscopically unresectable lesions (41%), where there was deviation from the planned management pathway (eg, administrative/service-, clinician- or patient-related delays) in acting on a detected lesion (41%), or potentially missed lesions located within areas of active inflammation or post-inflammatory change (36%).
Mooiweer et al57 reported inadequate colonoscopies in four patients (24%), incorrect surveillance intervals in nine patients (53%) and inadequate management of dysplasia in two patients (12%). Wintjens et al58 found that 56% of PCCRCs were due to missed lesions, and in addition, 30% of CRCs were diagnosed before any surveillance procedure. In an Italian case–control study, patients with IBD who developed PCCRC at index colonoscopy, more frequently had inadequate bowel preparation, a Boston Bowel preparation score <6 (multivariate OR=5.9, 95% CI 1.11 to 31.4) and the presence of high-risk factors for CRC development (OR=24.03; 95% CI 3.1 to 187.8). Prior exposure to immunosuppressors or biological agents (OR=0.17; 95% CI 0.03 to 0.83) and random quadrantic biopsy sampling (OR=0.19; 95% CI 0.04 to 0.85) were inversely correlated.59
1.4 Organisation of an IBD surveillance programme, and mechanisms to help support IBD surveillance concordance
1.4a Expert opinion: Concordance with IBD colonoscopic surveillance is suboptimal internationally for both initial screening and subsequent appropriate surveillance intervals, and risks undermining the effectiveness of IBD surveillance programmes.
1.4b Expert opinion: The systematic use of automated and personalised reminder strategies for IBD surveillance might help to increase IBD surveillance concordance; however, this is dependent on services being able to identify all patients with IBD who are eligible for surveillance, which is a baseline requirement.
Surveillance for CRC in IBD can be effective only if patients are fully supported to attend for examinations. Previous guidelines have not examined this problem in detail; however, it is recognised that adherence to both the initial screening examination, usually recommended at between 8 and 10 years of disease, and subsequent surveillance examinations, is suboptimal due to a number of organisational and patient factors. Rates of correct timing for initial screening colonoscopy ranged between 43% and 70% of patients, and adherence for subsequent surveillance examinations ranged from 25% to 74% (online supplemental table E).60–67 UK-specific data, available only in abstract form, confirm similarly low levels of concordance.68 69 Higher centre volume, measured either by number of colonoscopies or patients seen, seemed to improve levels of concordance.62 65 In a multicentre study examining causes for post-colonoscopy CRC in IBD, more than half of the cancers were due to inappropriately delayed surveillance.56 In a case–control study of patients who developed PCCRC, 43% of the patients did not adhere to the recommended surveillance interval compared with only 5% of controls without PCCRC.59
Most of the available studies post-2000 had organised surveillance programmes, and associated guidelines were more common, but even the most recent ones show suboptimal adherence, suggesting that further support of patients, clinicians and healthcare systems might increase effectiveness of surveillance programmes. The National Colorectal Cancer Round Table in the USA has set a strategic aim of 80% for CRC screening rates in every community,70 with Targets for Healthy People 2020 setting a 70% standard.
Few studies have looked at the reasons for non-attendance or interventions, specifically in IBD, to increase concordance with surveillance guideline recommendations. However large-scale, population-based studies on improving CRC screening concordance in non-IBD patients suggest that a combination of automated reminders, combined with personalised components for non-responders, was effective for increasing CRC screening uptake across ethnicities, age ranges (more effective for younger patients) and between sexes.71 This requires that all candidates eligible for CRC screening can be identified (by age in USA), but for IBD this will need either a database of all patients with IBD at an institution or a mechanism by which to extract details of patients with IBD from the wider electronic heathcare record.
Data on IBD specific mechanisms to increase engagement with CRC screening are limited, summarised in Box 1. The patient perspective of patients being empowered to engage in the decision-making about having CRC screening, and thereby a recognition of moving from the clinician’s expectation of ‘adherence’ to one of shared ‘concordance’ between clinician and patient, is important when considering interventions. Different units may choose different mechanisms to support concordance, with digital solutions—for example, WeChat is likely to be more prominent in the future. Wider patient education for anyone with an IBD diagnosis is likely to be important as approximately half of patients with IBD reported never having a discussion about CRC risk or the role of screening and surveillance colonoscopy in managing that risk with their healthcare provider.72
Mechanisms to help support patient engagement with IBD surveillance
Telehealth patient support (WeChat).323
Phone and letter reminders, automated where possible.324
Treat anxiety/depression in patients with inflammatory bowel disease (IBD).325
Health maintenance programme checklist.326
Increase patient clinical engagement—for example, by a virtual clinic.327
IBD surveillance multidisciplinary team or equivalent.328
Section 2: Risk stratification
2.1 When should surveillance be started and stopped?
2.1a GPS: We suggest that patients with IBD affecting the colon or rectum should be risk assessed for participation in a colonoscopic surveillance programme starting 8 years after onset of their IBD symptoms. Patients with PSC-associated colitis should be offered participation from the time of diagnosis.
2.1b GPS: We suggest that patients with Crohn’s disease not involving the colon proximal to the rectum, or isolated small bowel disease, or with ulcerative colitis endoscopically confirmed as confined to the rectum should not be offered surveillance but should be encouraged to participate in screening programmes offered to the general population.
2.1c Expert opinion: Any decision to stop colonoscopic surveillance should be taken in partnership with the patient and consider factors including patient tolerance of, and risks from, colonoscopy and the likely practical implications of any finding of advanced neoplasia or cancer. At the age of 75 years, such a discussion is suggested before continuing surveillance.
2.2 Who should or should not receive surveillance?
2.2a Expert opinion: Surveillance should be offered to those at risk of IBD-CRC, and in whom the benefit of surveillance is within their expected life span.
2.2b GPS: We suggest following a baseline procedure where risk is deemed to be low; participation in a surveillance programme should not be considered, and the patient should be advised to take part in population bowel cancer screening when appropriate, unless there is a change to baseline risk factors.
2.2c Expert opinion: Surveillance should be discontinued in those whose comorbidity or frailty risks exceed the risk of future symptomatic CRC.
2.2d GPS: We suggest that patients undergoing colonoscopic surveillance should have their risk reassessed after each surveillance episode to determine if further surveillance is necessary, particularly following two good-quality consecutive colonoscopies in which no active endoscopic or histological inflammation was detected.
IBD CRC surveillance aims to reduce the incidence of CRC in patients at higher risk of cancer, by identifying and resecting dysplastic lesions and cancer.2 73 Colonoscopic surveillance is recommended for those for whom the benefit of surveillance is within their expected lifespan, taking into consideration preparation and procedural risk,74 comorbidity,75 frailty76 and expected surgical morbidity, defined by standard grading systems such as the American Society of Anesthesiologists (ASA) Physical Status Classification.77 78
The GDG determined that a CRC risk of greater than 1.5 times that of the general population would meet the threshold for consideration of surveillance. Patients with IBD have an average CRC risk approximately 1.4–1.7 times that of the general population, which means that all patients with IBD should be considered for surveillance.6 However, this increased risk is not evenly distributed within the IBD population, some patients will have several risk factors which contribute to a higher risk and others may be closer to the general population risk.79 Population registry data provide evidence of increased risk of CRC in patients with UC but not in all patients with Crohn's disease (CD),26 with the risk in the UC population only rising above that of the background population around 8 years after diagnosis. These findings are supported by population meta-analyses, which also show that patients with UC limited to the rectum are not at increased risk of CRC.33 80 Since the extent of disease and distribution of both UC and CD can change over time, and given that diagnostic delay remains common in patients with IBD, we recommend that a baseline procedure is offered to all patients with IBD at 8 years after the onset of symptoms. This can then be used to determine any future surveillance needs. Surveillance should not be offered to those considered to be low risk, below the agreed threshold, such as those with UC proctitis adjusted HR=0.97 (95% CI 0.76 to 1.25)22 or isolated terminal ileal CD HR=1·09 (95% CI 0·89 to 1·34). Patients who have had their proctitis confirmed around 8 years from diagnosis might not need colonoscopic risk stratification.23 Although data are only available from smaller cohort studies, patients with PSC associated with UC appear to be at higher risk of CRC, with one cohort estimating the risk of CRC or dysplasia at 9% within the first 10 years, justifying an immediate start to a surveillance programme within this group.81 Even fewer data are available for patients with PSC associated with CD, with discordant findings.82 83
Cancer risk increases with advancing age. In a study of 211 patients aged >75 years with UC, surveillance procedures detected dysplasia or CRC in 41 (19.8%) patients aged 75 to 79 years, 31 (25.3%) in those aged 80 to 84 years, and in 11 (30.4%) of those aged ≥85 years. In a multivariate analysis increasing age and prior flat dysplasia/CRC were significant future predictors of dysplasia/CRC. Overall survival rate at 5, 10 and 15 years after age 75 years was 79%, 69% and 46%, respectively.84 Yet, even in patients at high risk for CRC, ongoing surveillance might expose them to the immediate risks of the intervention with little likelihood of surviving long enough to benefit, owing to the lag time for development of symptomatic CRC.85 86
No RCT data has addressed the need for ongoing surveillance in a high-risk population. In a simulated study (using data derived from national registries and considering factors other than age), screening was more cost effective for individuals without prior screening than for those with a negative screening colonoscopy 10 years previously, without comorbidities and with a high background risk for CRC.87 Current IBD surveillance algorithms determine future screening intervals based on the most recent procedure.1 Two retrospective studies have suggested that a lack of endoscopic or histological inflammation in previous consecutive procedures predicts a low risk of future CRC.88 89 In a multicentre European and North American study of 775 patients with colonic inflammatory bowel disease (excluding those in the highest risk category), two consecutive negative good quality colonoscopies predicted a very low risk of future advanced colorectal neoplasia. The median interval between the colonoscopies was 2.2 years, the median follow-up from first surveillance was 6.1 years, and no patient with two negative colonoscopies developed advanced colorectal neoplasia with 994 years of follow-up.88 A single-centre study from St Mark’s hospital with a median 13 years follow-up demonstrated that those with no microscopic inflammation over a 10-year follow-up period had an extremely low rate of development of any dysplasia.89 In a complicated disease like IBD, using a single factor to determine the need for future surveillance is likely to be inaccurate, and a more individualised approach to determine ongoing procedure is needed, including patient’s age, comorbidities, previous inflammatory burden, PSC and other risk factors for CRC.79
2.3a IBD CRC risk factors
2.3a (i) GPS: We suggest consideration of colectomy in patients:
Who at surveillance after optimised medical therapy continue to have severe active inflammation (endoscopic or histological).
OR alternatively have a calculated LARGE risk of advanced colorectal neoplasia at 5 years
2.3a (ii) GPS: We suggest annual surveillance for patients:
Who after optimised medical therapy continue to have moderate active inflammation (endoscopic or histological), or dysplasia, or primary sclerosing cholangitis or a colonic stricture.
OR Have a calculated MODERATE risk of advanced colorectal neoplasia at 5 years.
2.3a (iii) GPS: We suggest surveillance every 3 years for patients:
Who after optimised medical therapy continue to have mild active inflammation (endoscopic or histological), or extensive disease (Ulcerative colitis: proximal to the splenic flexure; Crohn’s disease: greater than 50% colonic involvement or inflammation in three or more colonic segments), or post-inflammatory polyps
OR alternatively a calculated SMALL risk of advanced colorectal neoplasia at 5 years
2.3a (iv) GPS: We suggest surveillance every 3 years for patients with colonic IBD and a family history of colorectal cancer in a first degree relative.
2.3a (v) GPS: We suggest patients should receive colonoscopic reassessment every 10 years and age appropriate population-based colorectal cancer screening if they have:
None of the additional risk factors described above
OR alternatively a calculated risk of advanced colorectal neoplasia at 5 years that is close to population risk
Patients with colonic IBD are at risk of CRC, and several risk factors have been identified which contribute to risk.22 23 79 However, this increased risk is not evenly distributed within the IBD population; some patients will have one or more risk factors which contribute to a higher risk, and others without major risk factors may be close to the general population risk.79 To determine the need for future surveillance a baseline procedure should be offered to all patients with IBD at 8 years after the onset of symptoms; patients with a concurrent PSC diagnosis, or following a liver transplant for PSC, should have annual surveillance procedures from the date of diagnosis of IBD. This should ideally be conducted in remission with pan-colonic dye spray (section 3.2b). Risk factors should be reviewed at clinic review at least annually, and surveillance intervals adjusted appropriately.
Previous BSG 2010 guidelines1 were developed on the assumption that all patients with IBD above population risk, specifically those patients with disease extension beyond proctitis, would require ongoing surveillance indefinitely and had limited ability to reflect the change in CRC risk over time. There are fixed risk factors, such as sex, age at IBD diagnosis, family history of CRC, PSC, disease extent and duration, which are not modifiable. The key modifiable risk factor is the severity of inflammation and the subsequent complications which arise owing to chronic inflammation, including strictures, post-inflammatory polyps, dysplasia and cancer. To reduce the overall cancer burden, patients should be supported to optimise modifiable factors, such as stopping tobacco smoking, maintaining a healthy weight and minimising obesity, drinking alcohol within the recommend limits, practising safe exposure to the sun90 and participating in national cancer screening programmes. In a multicentre prospective study of patients with IBD undergoing colonoscopic surveillance, smoking pack-years were associated with an increased risk of developing colorectal neoplasia, HR=1.17 (95% CI 1.03 to 1.32) per 10 pack-year increase.91
Surveillance in high-risk groups
In the 2010 guidelines, those at lowest risk were offered colonoscopic surveillance every 5 years; however, new data on the effectiveness of surveillance and IBD colorectal cancer biology suggest that 3 years may be the appropriate minimum interval if surveillance is to effectively prevent colitis-associated CRC or CRC-associated death. A Cochrane review37 (updated for this guideline) suggests that 3-yearly or more frequent surveillance can reduce the risk of developing CRC by one-third, and the risk of death from CRC by two-thirds compared with those having surveillance at intervals greater than 3 years or not at all (see section 1.2). High rates of post-colonoscopy CRC at 3 years suggest that longer intervals are likely to be ineffective (see section 1.3). Translational studies suggest that colitis-associated CRC occurs via a different molecular-genetic pathway from sporadic CRC, which may have an accelerated inflammation-dysplasia-cancer sequence, and results in ‘field cancerisation’, where the whole colonic mucosa becomes genetically unstable.92 In these scenarios precancerous change may not be endoscopically detectable.93 Approaches similar to surveillance in Lynch syndrome, with relatively short surveillance intervals, where the aim of surveillance is both to prevent cancer by removing precursors and finding early CRC that can be curatively surgically resected, preventing CRC-associated death may be appropriate.94
Surveillance in low-risk groups
The converse of this is that rates of CRC in the IBD population have dropped dramatically over the past 20 years owing to improvements in inflammatory control and other risk factors, and improved surveillance (see section 1.1). Compelling data now suggest that patients with IBD, without significant inflammatory burden or other risk factors, have a very low risk of developing advanced colorectal neoplasia (aCRN) or CRC over long time periods, up to 10 years, and that their risk is very close to that of the general population, and below the 1.5-fold threshold identified as appropriate for IBD-specific surveillance.88 89 In the 2020 BSG polyp surveillance guidelines, those with risk that is minimally elevated and close to population risk continued with population-based screening and not colonoscopic surveillance.78 Accordingly, those patients with IBD with close to population risk (and not receiving 1-year or 3-year colonoscopic surveillance) would continue with age-appropriate population-based CRC screening, with reassessment of risk factors at annual review, or a flare of disease should prompt interim reassessment. However not all IBD-associated CRC risk factors—for example, post-inflammatory polyps or disease extent, can be detected by non-invasive assessment. We therefore recommend colonoscopic reassessment for risk factors and dysplasia every 10 years after the initial 8-year colonoscopy, which is equivalent to the recommended population-based screening for all average-risk patients aged 45 or older in the USA.95 This approach provides an additional level of safety netting for patients with IBD whose risk factors may evolve over time and captures patients who have not met age-appropriate population based CRC screening.
Determination of how risk factors lead to surveillance intervals
A risk thresholding exercise was undertaken to calibrate the cut-off points for relative risk and absolute 5-year risk of aCRN. This categorisation produced four cohorts describing those close to population risk, small risk, medium risk and large risk, which corresponded to population-based surveillance and reassessment at 10 years, 3-yearly colonoscopic surveillance, annual colonoscopic surveillance, and consideration of colectomy, respectively. The GDG reviewed the literature on relative risk, specifically looking for risk estimates derived from more modern cohorts, and risk factors adjusted for other risk factors (multivariate risk), where possible (see online supplemental table F).22 23 79 96 While this gives an indication from the current best available synthesised evidence, significant concerns exist about risk of bias and wide confidence intervals for some risk factors; therefore the certainty of many of these findings should be interpreted with caution. Individual patient details, local context, among many other factors, could modify the risk. Additionally, recognition of shared decision-making is core to these recommendations, and these resources should support these discussions. In situations where risk estimates differed widely between studies, other non-adjusted or older observational data were considered by the GDG to determine which risk factors would trigger which surveillance intervals, and expert opinion was sought. This differs from BSG guidance in 2010 and 2019 when few risk factor data were available adjusted for other risk factors, and explicit risk thresholding was not conducted. Figure 3 summarises how risk factors using relative risks translate into surveillance intervals.

Relative risk-based and Multivariate risk model-based approach to defining surveillance intervals. *If moderate or large risk factors or 6.9+% risk follow that surveillance. Multivariate risk model available at: https://ibd-dysplasia-calculator.bmrc.ox.ac.uk. CRC, colorectal cancer; HPV, human papilloma virus; PSC, primary sclerosing cholangitis; SPS, serrated polyposis syndrome.
Family history of CRC
The population prevalence of patients with IBD who have a first-degree relative (FDR) with CRC ranges from 1.6% to 2.9%.22 23 97 98 Previous international IBD surveillance guidelines1 2 20 99 have used a family history of a FDR with CRC to determine surveillance intensity, with those with an FDR aged <50 being assessed as being at high risk, and those with an FDR aged ≥50 being at moderate risk, on the basis of a Swedish population-based study with observations from 1953 to 1995, where the overall relative risk of CRC for those with an FDR with CRC was 2.4 (95% CI 1.4 to 4.4).98 This is consistent with a 2021 systematic review and multivariable analysis, where a family history of CRC was associated with a risk of advanced colorectal neoplasia of 2.42 (95% CI 1.14 to 5.16), and a Scandinavian population-based study that compared patients with IBD with the general population CRC risk, with a relative risk of having an FDR of 2.94 (95% CI 1.82 to 4.73) for patients with UC and 1.53 (95% CI 0.86 to 2.75) for patients with CD.22 23 79 Those with an FDR with CRC therefore would be within the risk threshold boundaries for a small increase in risk, and 3-yearly surveillance is suggested; however, if they have additional risk factors or a multivariate calculated 5-year aCRN risk, then that would put them into a higher-risk group, and they should receive surveillance for their highest risk.
However, splitting the relative risk in the study by Askling et al98 into those aged <50 compared with those ≥50 resulted in relative risks of 9.2. vs 1.7 respectively.98 It is unclear how many of the patients aged <50 had Lynch syndrome, which it was not possible to test for routinely at that time, but this is likely to have driven up risk in the <50 years age group. Those with IBD and an FDR with CRC, aged <50, should be evaluated with their relatives in accordance with the BSG guidelines on hereditary CRC,100 and those with IBD and Lynch syndrome or other familial syndromes should be treated separately (see Special circumstances). Those with an FDR aged <50 without Lynch syndrome should be considered together with those aged ≥50 for 3-yearly surveillance.
2.3b Multivariate risk models
2.3b GPS: We suggest that multi-variate and dynamic modelling tools may offer more personalised advanced colorectal neoplasia risk estimates to aid shared decision making with patients regarding surveillance strategies
In a complex disease like IBD, using only a single ‘top’ or highest risk factor to determine future surveillance might substantially overestimate or underestimate risk, and a more individualised approach to determine ongoing risk is needed, including patient’s age, comorbidities, previous inflammatory burden, PSC, and other risk factors for CRC.79 Recently, multivariate risk factor calculators for IBD have become available, which include up to eight clinically available risk factors, that are dynamic and can be recalculated as risk factors change over time.96 These have been developed and validated on cohorts which are broadly appropriate for UK-based practice and healthcare systems, including one UK cohort, with the remainder from Europe and North America. These calculators consider multiple risk factors and their interaction over time, and produce an aCRN risk over 5-year and 10-year time scales. Although not perfect, they probably represent an advance for risk prediction over single ‘top’ risk estimation over time, with both greater precision and individualisation for patients. The GDG risk thresholding exercise proposed surveillance intervals for specific cut-off points for future predicted risk of developing aCRN over 5 years, based on this risk calculator; these are summarised in figure 3. The risk calculator is available online at https://ibd-dysplasia-calculator.bmrc.ox.ac.uk. As the risk calculator does not include a family history of CRC in a first-degree relative, which remains a significant risk in multivariate analysis, this is dealt with separately.
For the cohort with a predicted aCRN risk <3.6% at 5 years, the average risk of aCRN is calculated to be approximately 1.8%,96 which is similar to estimates of the 5-year aCRN risk of 2.2–2.7% for the non-IBD age-matched general population.101 102 On this basis, population-based screening and endoscopic reassessment at 10 years is now recommended in these guidelines for this low-risk group
The risk model behind the web calculator is based on a large and diverse dataset from North America and Europe96; however, at extremes of age or after very longstanding surveillance the dataset is more limited, and risk estimates might be less precise. Therefore, the calculator is restricted to ages 18–75 and to a maximum of 30 years' surveillance follow-up. Equally some relatively common clinic scenarios are not accounted for—or example, a family history of CRC, nor does the model consider ‘special circumstances’, see narrative below. Clinicians should apply the model within these parameters and take into account the wider clinical context and patient preferences when making surveillance decisions. Use of the calculator and model is not a replacement for clinical care and shared decision-making by an experienced clinician.
Special circumstances
Anal cancer risk and HPV
In the United Kingdom, there is no national screening programme for anal cancer as this is a rare cancer in the general population.103 The established risk factors for anal cancer include human papillomavirus (HPV) infection, a history of sexually transmitted diseases, a history of vulvar or cervical carcinoma, immunosuppression by disease or therapy and smoking.104
Chronic perianal fistulising disease increases anal cancer risk,105 106 and other risk factors, such as concurrent HPV infection and chronic immunosuppression, may influence risk.107 In the absence of chronic perianal fistulising CD, a meta-analysis of 33 patients reported the annual incidence of anal squamous cell cancer to be 0.009 cases per 1000 patient-years in UC and 0.02 cases per 1000 patient-years in CD, which is similar to that of the general population.108 In this study, there were more cancers in women, they occurred at an earlier age of onset than in other high-risk groups, the 5-year survival rate was 37% compared with >60% in the general population109 and, when tested, two of five cancers were positive for HPV.108
The overall natural history of anal cancer in IBD is more aggressive, and therefore patients with IBD are encouraged to consider the HPV vaccine when available through the national screening programme. The national HPV programme recommends vaccination for all children aged 12 to 13 years old and for gay people, bisexuals, men who have sex with men up until the age of 45 years old.110 Additionally, other lifestyle factors, such as stopping tobacco smoking and modifying sexual practices, can minimise HPV infection implicated in anal cancer. Although suggested by others, there are no data to suggest that regular anal smears would minimise anal cancer risk.105
Endoscopists should be aware of the risk of anal cancer in patients with IBD and carefully examine the anal canal both digitally and endoscopically. Use of narrowed spectrum endoscopy (NBI, FICE, iSCAN) with magnification can highlight dilated intrapapillary capillary loops in the anal squamous mucosa suggestive of anal intraepithelial neoplasia.111
Perianal disease and anal and rectal cancer risk
Perianal fistulising disease is an aggressive CD phenotype with a prevalence of 14–43%112 and is associated with an increased risk of anal108 and rectal cancer.113 114 The prevalence of CD fistulae-related adenocarcinoma is estimated at 0.17–0.7% after 10 years from fistulae detection.115 The CESAME113 group reported on 2911 patients with past or current anal/or perianal Crohn’s disease with incidence rates of 0.26 per 1000 patient-years for anal squamous cell carcinoma, 0.38 per 1000 patient-years for perianal fistula-related adenocarcinoma, and 0.77 per 1000 patient-years for rectal cancer. In the 16 575 patients with IBD without anal or perianal lesions, the incidence rate was 0.08 per 1000 patient-years for anal cancer and 0.21 per 1000 patient-years for rectal cancer. Although the absolute risk is low, for patients with fistulising disease, the cancer risk exceeds those on annual IBD CRC surveillance programmes.106
The need for surveillance in perianal fistulising CD has not been defined in current guidelines,99 112 116 117 and the optimal intervals and modalities are unknown. In the absence of a dedicated consensus or guidelines, we would suggest careful assessment at regular intervals and especially when symptoms change, with standard techniques, including endoscopy, imaging and direct examination under anaesthesia with biopsy of the fistulous tracts112 to detect cancer early.
Colonic strictures in IBD
In a meta-analysis of 11 studies, reported in abstract form, the pooled 10-year colonic stricture rate was 3.2% (95% CI 1.5% to 6.8%) in IBD. In this study, the pooled incidence of strictures with associated high-grade dysplasia (HGD) or CRC was 21.9% (95% CI 12.2% to 36.5%).118 In a more recent meta-analysis, the pooled univariable analysis of patients with IBD with colonic stricture resulted in an OR of 7.78 (95% CI 3.74 to 16.18) for aCRN.79 The association between strictures and neoplasia has not been universally confirmed. In a single-centre study of 789 patients with IBD undergoing CRC surveillance, 9% had colorectal strictures on index colonoscopy, and there was no significant association with future aCRN after a median of follow-up of 3.4 (IQR 1.3–5.4) years.119
The detection of a new stricture should include complementary assessment with ileo-colonoscopy, biopsies and cross-sectional imaging as suggested in the main BSG IBD Guidelines GPS numbers 11 and 82.
Young age at diagnosis
In a large UK primary care population-based study from 2000 to 2017, involving over 11 million patients, 65 700 cases of IBD were identified in paediatric patients with IBD (PIBD) diagnosed at age <17 years, and the incidence rose at an average rate of 2.9% (95% CI 1.3% to 4.4%) per calendar year.120 The risk of CRC in 9405 paediatric patients (diagnosed at age <18 years) with IBD was assessed in a Swedish nationwide, register-based cohort study from 1964 to 2014. There was an increased risk of CRC in those with UC (HR=33.3, 95% CI 23.1 to 49.1) and CD (HR=5.8, 95% CI 3.2 to 10.4) respectively, compared with age- and sex-matched reference individuals from the general population during follow-up into adulthood.121 Although the absolute incidence rate is low for UC, 0·42 (95% CI 0·31–0·56) per 1000 people per years and CD, 0·24 (95% CI 0·15–0·39), there is an excessive HR for CRC death in UC of 34.2 (95% CI 18.8 to 62.2) and in CD of 9.27 (95% CI 4.36 to 19.7).22 23 A meta-analysis of cancer in PIBD found a 2.4-fold increased rate of cancers (mainly of GI tract origin) among patients with paediatric-onset IBD.122 The relevant problem for PIBD services is that so few of these CRCs occur before transition to adult services; the EPIMAD group reported none of the five cases of CRC occurred at <18 years of age in 12 957 years of follow-up in 1344 paediatric patients with IBD.123
No evidence-based guidelines exist for surveillance of CRC in childhood-onset IBD, and contemporary guidelines refer to adult recommendations.124 125
While the absolute risk of developing CRC in patients diagnosed with IBD below the age of 18 is low, the relative risk is very high. Clinicians and patients should consider colonoscopic surveillance as they transition to adult services at 1–3-yearly intervals, starting at age 16–18 years.
IBD and hereditary CRC syndromes
IBD and hereditary CRC syndromes such Lynch, familial adenomatous polyposis, MYH-associated polyposis (MAP), serrated polyposis syndrome and hamartomatous polyposis syndromes are independently associated with an increased risk of CRC.100 126 127 It is uncertain whether the co-occurrence of these conditions increases cancer risk cumulatively, and the optimal surveillance interval in these patients has not been defined (online supplemental table G).128–132
In the largest study from the USA, involving 205 centres and including 24 584 patients, of whom 568 also had IBD, CRC risk was significantly increased when both conditions were present together (multivariate OR=1.55, 95% CI 1.10 to 2.18).133
In the 2022 ECCO CONFER multicentre case series, 26 cases of patients with IBD (10 with UC, 15 with CD and 1 with IBD-U) and co-occurrence of Lynch syndrome (n=16), familial adenomatous polyposis (n=7), aFAF (n=1) and MAP (n=2) were described. In this study 10/26 patients developed cancer, with a median CRC age of diagnosis at 35 years (IQR 24–44). The cancer in 8/16 of those with Lynch syndrome and in 2/7 of those with familial adenomatous polyposis.132
In a separate study from the Netherlands in 2016, CRC risk was assessed in patients with Lynch syndrome and IBD concurrently. The cumulative incidence of CRC was similar between groups, 4 of the 15 patients (26.7%) with Lynch syndrome and with IBD compared with 311 of the 1031 patients (30.2%) with Lynch syndrome without IBD developed cancer. The median age of cancer diagnosis was 10 years younger (36 years vs 46 years) in patients who had both Lynch syndrome and IBD, and all four patients had UC.128
In the absence of consensus guidelines, once concurrent IBD and a hereditary CRC syndrome has been diagnosed, the patient should continue with the most intensive surveillance programme.
2.4 The role of biomarkers pre-dysplasia detection to guide surveillance and colectomy risk
2.4 Expert opinion: There is insufficient evidence to generate a statement on the role of biomarkers before colonoscopic assessment of baseline risk to guide surveillance and colectomy risk.
The non-neoplastic colitic epithelium not only accumulates genomic alterations at a much faster rate than that of the healthy colon, but there is also positive selection for these genomic changes, resulting in the topographic spread of mutant non-neoplastic clones across large colonic segments, which is a phenomenon unseen in the non-inflamed colon.134 Studies using point mutation analysis in surveillance biopsies,135 136 stool samples137 and blood samples138 to predict cancer risk pre-dysplasia detection are limited by small patient cohorts and/or low sensitivity for routine clinical use. Of note, the presence of TP53 mutations in random surveillance biopsies was not predictive of future cancer risk.135 136 Commercially available multitarget stool testing panels for CRC screening (modified for IBD by eliminating FIT from the panel) demonstrated only a fair sensitivity of 79% for detection of advanced colorectal neoplasia in a single screening round.137
Chromosomal copy number alterations (aneuploidy) are a recognised, early feature of IBD-related carcinogenesis,139 with aneuploidy detected in non-neoplastic colitic epithelium.140 In a recent meta-analysis, aneuploidy was an independent prognostic factor for colitis-associated advanced colorectal neoplasia after multivariable analysis, with a HR of 4.3.79 Nevertheless, larger studies with prospective validation are required prior to the use of aneuploidy burden in routine clinical practice.
2.5 IBD CRC chemoprevention
2.5a (i) GPS: We suggest when monotherapy non-sulfasalazine mesalazine is prescribed as the only treatment for ulcerative colitis it may also have a chemopreventative effect. It is not clear whether there is an additional chemopreventative effect with non-sulfasalazine mesalazine for patients with ulcerative colitis receiving advanced therapies, where the mesalazine is not needed for control of inflammation.
2.5 (ii) Expert opinion: We do not suggest the use of thiopurines solely for their chemopreventative effect.
In our systematic review and meta-analysis, 32 observational studies with 5-ASAs, including 462 408 patients—9847 with CRC and/or dysplasia—and 35 studies with immunomodulators (IM), including 544 380 patients—10 794 with cancer/dysplasia—were assessed for their impact on the occurrence of CRC and dysplasia in patients with IBD.141 The overall standardised RR for 5-ASAs was 0.78 (95% CI 0.70 to 0.86; p<0.0001), with moderate heterogeneity (I2=52.1%, 95% CI 24.6% to 66.6%; p=0.0002). For IM the RR was 0.91 (95% CI 0.82 to 1.02; p=0.09), with high heterogeneity (I2=82.7%, 95% CI 77.3% to 86.4%; p<0.0001). An Egger test showed no publication bias for 5-ASA (p=0.11) or IM (p=0.33). The data were further subdivided by several clinically relevant groups. For 5-ASA, most studies suggested a protective effect against the development of cancer except in Asian populations, mixed IBD populations, pure surveillance groups, studies reporting unadjusted univariate ratios and sulfasalazine users. For IM, data interpretation was limited by a moderate to high degree of heterogeneity between the studies; however, studies involving European populations, hospital-based cohorts, case–control studies and mixed IBD phenotype suggested a protective effect against the development of cancer/dysplasia. One study,142 contributed to 71% of the overall study population and was graded as moderate risk of bias on the Newcastle Ottawa Scale. Owing to the inherent limitations of observational studies, we were unable to determine if the reduction in CRC and/or dysplasia risk was independent of effective control of colonic inflammation.
Section 3: Colonoscopy
3.1 Choice of bowel preparation in IBD surveillance colonoscopy
Patients with IBD consider bowel preparation as the most important element in acceptance of CRC surveillance.143 144 Guidelines on bowel preparation recommend low- or high-volume PEG-based bowel preparation in IBD.144 A split dose preparation was recommended. Repeat colonoscopy within 1 year was recommended if the bowel preparation was inadequate, although this was non-IBD specific. Given the potentially accelerated inflammation-dysplasia-carcinoma sequence in IBD, and an IBD surveillance case–control study that showed PCCRC was more commonly associated with poor bowel preparation, Boston bowel peparation score (BBPS) <6 (multivariate OR=5.9; 95% CI 1.11 to 31.4), a shorter interval of 3–6 months might be more appropriate for patients with IBD and failed preparation (see section 6.1 for key performance indicators (KPIs)).59
The European Society of Gastrointestinal Endoscopy (ESGE) guidelines currently recommend high- or low-volume PEG-based bowel preparation for IBD colonoscopy.144 Recently available, non-PEG sulfate-based options provide additional choices.145 146 We conducted a systematic review and meta-analysis on the efficacy and safety of bowel preparations for patients with IBD undergoing colonoscopy, using data from RCTs covering all preparation types.147 Primary outcomes included bowel preparation success (defined using validated bowel preparation quality scores), tolerability, willingness to repeat and safety. Secondary outcomes included caecal intubation rates and abnormal serum electrolyte levels.
Ten RCTs, involving 1479 patients with IBD, compared various preparations: 4 L PEG with/without simethicone,148 castor oil versus senna,149 two commercial low-volume PEG-based preparations,150 2 L PEG versus 4 L PEG,151–153 and low-volume PEG (≤ 2 L) with additives versus non-PEG-based preparations.145 146 154 155
For 2 L versus 4 L PEG, there was no significant difference in bowel preparation success (RR=0.98, 95% CI 0.88 to 1.09; I²=33%, two RCTs; moderate certainty evidence).152 153 However, willingness to repeat the preparation was higher for 2 L PEG (RR=0.69, 95% CI 0.59 to 0.80; I²=18%, two RCTs; high certainty evidence).152 153
Comparisons between low-volume non-PEG and PEG preparations indicated similar bowel preparation success (RR=0.96, 95% CI 0.90 to 1.01; I²=6%, three RCTs; moderate certainty evidence).145 146 155 The evidence on tolerability and willingness to repeat these preparations was less certain (RR=0.81, 95% CI 0.67 to 0.99; I²=76%, three RCTs; very-low certainty evidence and RR=0.77, 95% CI 0.59 to 0.99; I²=83%, three RCTs; very-low certainty evidence, respectively).145 146 155 There was no significant difference in caecal intubation rates (RR=0.98, 95% CI 0.93 to 1.03; I²=0%, two RCTs; low certainty evidence),145 146 and no abnormal electrolyte levels were reported post-bowel preparation in either group.
Subgroup analysis revealed comparable effectiveness of picosulfate-based (RR=0.89, 95% CI 0.78 to 1.01; I²=0%, one RCT)155 and sulfate-based preparations (RR=0.98, 95% CI 0.91 to 1.05; I²=28%, two RCTs)145 146 compared with low-volume PEG-based preparations. Similar trends were noted for tolerability (RR=0.86, 95% CI: 0.73 to 1.01; I²=22%, one RCT with picosulfate-based and RR=0.76, 95% CI 0.45 to 1.26; I²=91%, two RCTs with sulfate-based versus low-volume PEG-based) and willingness to repeat (RR=0.62, 95% CI 0.33 to 1.16; I²=86%, one RCT with picosulfate-based and RR=0.88, 95% CI 0.65 to 1.20; I²=86%, two RCTs with sulfate-based versus low-volume PEG-based).145 146 155
Moderate certainty evidence from two trials supports low-volume PEG with additives as comparably successful to high-volume PEG, with increased willingness to repeat.152 153 Moderate certainty evidence from three trials indicates similar success between non-PEG-based and PEG-based preparations.145 146 155 Both low-volume PEG-based and non-PEG-based preparations have evidence supporting their clinical usefulness for patients with IBD, broadening choices beyond the ESGE guidelines.144 Further research, including network meta-analysis and head-to-head comparisons with standardised outcomes, is essential for a more nuanced outcomes assessment. Furthermore, the current studies included bowel preparation assessments for surveillance and disease activity, which might affect endoscopist perception of what would be considered acceptable bowel preparation.
3.2 Choice of colonoscopic modality for IBD surveillance colonoscopy
3.2a GPS - We recommend when performing surveillance colonoscopy with White Light, High Definition is used over standard definition for dysplasia and CRC detection
High-definition (HD) endoscopy provides image signals of higher pixel density (>1 million pixels) than standard-definition (SD) (approximately 100 000 to 400 000 pixels) with faster line scanning on HD monitors, leading to sharper images with fewer artefacts.156A retrospective observational study from 2012 (n=203) found that dysplasia was detected in approximately twice as many patients with HD colonoscopy as among those undergoing SD colonoscopy (adjusted prevalence ratio 2.2; 95% CI 1.1 to 4.5).157
A network meta-analysis (NMA) in 2019 showed that HD colonoscopy with white light (WLE) was significantly better at detection of non-polypoid neoplasia compared with SD WLE colonoscopy (OR 0.12, 95% CI 0.02 to 0.93) and was better than SD WLE for detection of any dysplasia (OR 0.54, 95% CI 0.27 to 1.08).158
· 3.2c Expert opinion: We cannot make a GRADE recommendation on the use of Virtual chromoendoscopy (NBI, FICE and iScan) for colonoscopic surveillance in patients with IBD
We conducted a network meta-analysis,159 which included 26 randomised controlled trials involving 4159 participants.160–185 It compared six endoscopic modalities for IBD surveillance: HD white light endoscopy (HD-WLE), HD virtual chromoendoscopy (HD-VCE), HD dye-based chromoendoscopy (HD-DCE), HD-WLE with segmental re-inspection, auto-fluorescence imaging and full-spectrum endoscopy.
For the primary outcome of patients with at least one dysplastic lesion detected, 23 studies160–173 175–179 181–183 185 reported this outcome, with 19160–164 166–173 176–179 183 185 connected in the main network meta-analysis. Direct evidence from head-to-head comparisons showed that HD-DCE was superior to HD-WLE (RR=1.60, 95% CI 1.09 to 2.35). The network evidence supported this finding, showing that HD-DCE might be better than HD-WLE (RR=1.42, 95% CI 1.02 to 1.98, low GRADE certainty). Full-spectrum endoscopy may be no different from HD-WLE (RR=3.24, 95% CI 0.66 to 15.87, low GRADE certainty). Other modalities showed very low GRADE certainty results: HD-WLE with segmental re-inspection (RR=1.35, 95% CI 0.66 to 2.77), auto-fluorescence imaging (RR=1.18, 95% CI 0.55 to 2.57) and HD-VCE (RR=0.99, 95% CI 0.69 to 1.43).
For the outcome of patients with at least one dysplastic lesion detected from targeted biopsies, 16 studies160–164 166 167 169–173 176 179 183 185 were connected in the network meta-analysis. Direct evidence again favoured HD-DCE rather than HD-WLE (RR=1.64, 95% CI 1.11 to 2.42). However, the network evidence for this comparison had very low GRADE certainty (RR=1.41, 95% CI 1.00 to 1.98).
For the outcome patients with at least one lesion of any type detected, direct evidence suggested a potential benefit of HD-DCE over HD-WLE, but the result was not statistically significant (RR=1.46, 95% CI 0.92 to 2.32). The network evidence for this or this comparison had very low GRADE certainty (RR=1.34, 95% CI 0.89 to 2.01).
Subgroup and sensitivity analyses were performed for the primary outcome. The subgroup analysis for modality subtypes, including high or low concentration HD-DCE and HD-VCE subtypes, did not reveal major deviations from the main analysis. Sensitivity analyses were conducted for studies including participants with inactive disease only, studies where serrated lesions were not considered and studies where more than one endoscopist performed the trial endoscopies. These analyses also did not show significant deviations from the main findings, supporting the robustness of the primary results.
Limited data on serious adverse events precluded meta-analysis, with only two serious events reported among 2164 patients (very low GRADE certainty). The analysis was limited by the low frequency of dysplasia outcomes and the inclusion of various endoscopic technologies with different resolutions and capabilities.
Overall, both direct and network evidence suggest that HD-DCE may be more effective for detecting dysplasia and any lesions than HD-WLE, although the certainty of evidence is low. Other modalities showed very low GRADE certainty results, making it difficult to draw definitive conclusions about their effectiveness. The subgroup and sensitivity analyses support the main findings, indicating the consistency of the results across different study conditions and patient populations; however, high-grade dysplasia or CRC may be less frequent but more important outcomes for surveillance in IBD, which were not examined in this meta-analysis. A recent conventional pairwise meta-analysis comparing HD-WLE and HD-DCE, which used most of the studies included here, did not see a significant improvement in the detection of high-grade dysplasia (OR=2.21; 95% CI 0.64 to 7.62, low GRADE certainty due to very serious imprecision) or CRC with dye spray.186
3.3 Artificial intelligence system support in IBD colonoscopy
3.3 Expert opinion: Current artificial intelligence systems—compuer-aided detection/computer-aided diagnosis (CADe/CADx)—for IBD neoplasia detection and/or characterisation are not recommended. Further studies on IBD-specific CADe systems are required.
Artificial intelligence (AI) devices that offer CADe have been shown to improve adenoma detection rates by 1.24-fold (95% CI 1.17 to 1.31) in a meta-analysis of 24 randomised controlled trials.187 However, these devices are not suitable for, and do not have marketing authorisation for, use in patients in IBD. The algorithms used in these devices have been trained from datasets, which specifically excluded patients with IBD.
US and UK studies found that using generic CADe systems in patients with IBD produced poor results for dysplasia detection.188 189 The US study using their own version of CADe developed with non-IBD datasets had a sensitivity of 50% and accuracy (F1 score) of 64% for IBD-related polypoid lesion detection.188 The UK study using a commercially available CADe system showed a sensitivity of 71.7% and a specificity of 72.5% for detection of IBD-related neoplastic lesions189; however, in both cases these were significantly improved when retrained with IBD-specific images: US study IBD-CADe sensitivity 95%, accuracy 95%, UK study IBD-CADe sensitivity 93.5% and specificity 80.6%.188 189
Some attempts have been made to develop AI systems for polyp characterisation (CADx) and detection in patients with IBD (online supplemental table H).188–190 A retrospective Japanese study of 99 dysplastic lesions, tested for diagnostic accuracy against endoscopists using a 186 test images, showed no improvement in diagnostic performance compared with expert endoscopists.190 Another retrospective study from the USA, used still images for developing a detection algorithm, which was then tested on nine HD white light videos collected from patients with IBD. On subgroup analysis, the sensitivity for detection of small <5 mm polyps was 93% compared with a sensitivity of 83% for detection of >10 mm polyps.188 A third study from the UK was trained on 18 051 images from both patients with IBD and non-IBD patients and tested on 30 consecutive surveillance colonoscopies with white light in patients with IBD. Their AI algorithm detected 90.4% of lesions with a characterisation accuracy of 82.55%.189
Section 4: Pathology
Colitis induces cycles of ulceration and repair, resulting in damage to surrounding epithelial cells. In surviving cells, it is hypothesised that the inflammatory milieu drives a selective pressure for the acquisition of mutations to enhance cell-intrinsic fitness advantage and permit residual epithelial cell survival. The most frequently reported mutation is of TP53, with loss of function (the guardian of the genome), followed by MLH1, KRAS and APC; other changes are also seen frequently, such as aneuploidy and microsatellite instability.191 Consequently, TP53 mutation and aneuploidy are frequently seen in patients with longstanding colitis, even after resolution of acute inflammation.192–196
It is hypothesised that recurrent cycles of ulceration and restitution can lead to the rapid and widespread distribution of these mutated cells across the length of the colon,197 presenting a risk for subsequent multifocal dysplasia development and a significant challenge for endoscopic surveillance and prevention. The presence of important oncogenic driver mutations, which can even be found in phenotypically non-dysplastic crypts, is referred to as ‘field cancerisation’.93
4.1 Reporting dysplasia and non-conventional dysplasia in IBD
4.1a GPS: We recommend that double reporting is used whenever dysplasia is suspected.
4.1b Expert opinion: Pathologists evaluating biopsies from patients with longstanding IBD should adopt a pragmatic approach to dysplasia classification, recognising the diverse spectrum, including conventional, non-conventional and mixed types. In pathology reports, it is suggested that comments should be included on whether observed dysplasia aligns with conventional adenomatous-like dysplasia or exhibits characteristics indicative of non-conventional dysplasia. The Harpaz classification may be referenced in discussions but is not mandatory for reporting.
4.1c GPS: Upon the diagnosis of any form of dysplasia in patients with IBD, we recommend a referral for discussion with an appropriate Multidisciplinary Team (such as an IBD or CRC MDT).
4.1d Expert opinion: While not mandatory, pathologists might consider using p53 immunohistochemistry as an adjunct to differentiating dysplasia from reactive changes.
The identification of conventional (adenomatous) dysplasia and non-conventional colitis-associated dysplasia and its differentiation from sporadic dysplastic lesions, such as sporadic adenomas, can be very challenging.198 Features favouring an area of conventional dysplasia being colitis-associated include its presence within a segment of colon in which active inflammatory bowel disease is or has been present. Colitis-associated dysplasia might also present as a less well-defined lesion than a sporadic adenoma, and a mixture of dysplastic and non-dysplastic crypts may be present. Biopsies from the mucosa surrounding a focus of conventional dysplasia might reveal further evidence of dysplasia that is not endoscopically apparent.
Non-conventional dysplasia might not be identified as a form of dysplasia unless the pattern present is recognised by the pathologist as a pattern of non-conventional dysplasia. Several classifications systems have been proposed for non-conventional dysplasia, of which the Harpaz system is the most recent (box 2).199According to this system, non-conventional dysplasia can be subdivided into intestinal, gastric and mixed intestinal-gastric types. Intestinal patterns include goblet cell-deficient, crypt cell, sessile serrated lesion-like, traditional serrated adenoma-like and serrated not otherwise specified types. Gastric patterns include adenoma-like and serrated types. Non-conventional dysplasia appears to have a similar, or higher, risk of future development of advanced colorectal neoplasia compared with conventional dysplasia.200 201
Dysplastic and non-dysplastic lesion pathological categorisation in inflammatory bowel disease
Dysplasia
Intestinal
Tubular/villous adenoma-like (ie, ‘conventional’ dysplasia)
Goblet cell-deficient
Crypt cell
Sessile serrated lesion (SSL)-like
Traditional serrated adenoma-like
Serrated not otherwise specified
Gastric
Tubular/villous adenoma-like
Serrated
Mixed intestinal-gastric
Non-dysplastic
SSL without dysplasia
Hyperplastic
Serrated epithelial change
The detection of conventional or non-conventional dysplasia has very significant implications for patients on the intensity of surveillance and potential to undergo major resectional surgery. Inflammation can mimic dysplastic changes, and non-conventional dysplastic changes can be subtle or unfamiliar. Therefore, when dysplasia is suspected, we recommend review by a second pathologist (double reporting), ideally a GI specialist, and review at an appropriate MDT meeting which should comprise at a minimum: an IBD gastroenterologist, interventional endoscopist, colorectal surgeon, pathologist, radiologist, IBD nurse specialists and an MDT coordinator.202 203 A ‘hub-and-spoke’ model might help smaller institutions.
While TP53 mutation is considered to be a relatively late event in sporadic colorectal carcinogenesis, such mutations typically occur early in IBD-associated neoplasia.204 This allows for the use of p53 immunostaining as an adjunct in the diagnosis of IBD-associated dysplasia. An abnormal p53 staining pattern (either overexpression or no expression/null phenotype) might be useful in supporting a diagnosis of dysplasia rather than reactive atypia,205–207 and might also be useful if favouring IBD-associated low-grade dysplasia rather than sporadic low-grade dysplasia.
4.2 What is the role of serrated lesions and serrated epithelial change?
4.2a Expert opinion: The importance of serrated epithelial change (SEC) seen on biopsy, without a corresponding mucosal lesion and with no pathological evidence of conventional or non-conventional dysplasia, is unclear, and is not currently suggested to lead to more intensive surveillance; however, SEC with dysplasia, or hypermucinous and/or villiform changes should have MDT review and a repeat colonoscopy with an expert endoscopist.
4.2b Expert opinion: Sessile serrated lesions (SSLs) without dysplasia, either within or outside the colitis segment, should be managed in accordance with guidelines for sporadic serrated lesions. Where there is uncertainty about whether an SSL is dysplastic, an expert second pathological opinion should be sought
Serrated epithelial change (SEC) might be difficult to distinguish from serrated forms of non-conventional dysplasia. Serrated epithelial change is characterised by architectural serration without cytologic atypia—namely, without the nuclear changes that are characteristic of dysplasia. It is unclear whether SEC is a consequence of previous longstanding inflammatory disease or a separate risk factor in its own right.208–210 Serrated epithelial change showing a hypermucinous growth pattern or a pronounced villiform architecture is more concerning and should prompt MDT review and repeat expert colonoscopy.211
SSLs without dysplasia are not thought to be part of the inflammation-dysplasia-carcinoma sequence that leads to the development of IBD-associated CRC.92 In 6602 patients with IBD with 78 serrated lesions, no patient with a non-dysplastic serrated lesion developed advanced neoplasia over a 10-year follow-up period.212 In a Dutch cohort of 198 patients with IBD with serrated lesions, SSLs without dysplasia did not affect the subsequent advanced CRN risk (HR=0.87, 95% CI 0.11 to 6.88).213 The risk of metachronous neoplasia for patients with IBD with serrated lesions appears similar to that of the general non-IBD population who have serrated lesions.214 SSLs with dysplasia may be encountered as part of the spectrum of non-conventional dysplasia spectrum, although it is accepted that there is very considerable interobserver variation in this assessment, and so where there is uncertainty, a second expert pathological opinion should be obtained.198
4.3 Role of non-targeted biopsies
4.3a Expert opinion: Biopsies should be carried out to assess histological disease activity and disease extent during surveillance examinations.
4.3b Expert opinion: Additional quadrantic mapping non-targeted biopsies every 10 cm or from each colonic segment for specific patient risk groups should be considered even when dye spray is used: patients with primary sclerosing cholangitis, a history of dysplasia (visible or invisible) within the colitis segment in the past 5 years, patients undergoing segmental colectomy, patients with a retained rectum, and the rectal cuff of an ileal pouch are all considered to be in this category.
Inflammation is a key driver of IBD-associated CRC with risk proportional to severity, extent and duration of inflammation.89 Biopsies from each segment of the colon and from the rectum may be useful during surveillance colonoscopy in order to gain a histological measure of the disease activity and extent. It should be remembered that the colorectal mucosa in IBD that is quiescent might appear histologically normal. It is important that the pathologist is aware of the anatomical site of the biopsies so that an accurate assessment can be made of disease extent.
Targeted biopsies following a technique such as dye spraying are more likely to identify dysplasia in patients with longstanding IBD than are non-targeted random biopsies215–217; however, in some scenarios, random four quadrant biopsies every 10 cm or from each colonic segment might increase dysplasia yield for those with previous neoplasia or PSC218; or enhance confidence in the absence of field cancerisation prior to segmental resection; or assist when mucosal assessment is challenging—for example, diversion colitis. Non-conventional dysplasia is frequently not detectable endoscopically (‘invisible dysplasia’) and may be more frequent in PSC.200 219 An Italian case–control study reported that patients with IBD who developed PCCRCs were less likely to have had quadratic random biopsies as well as targeted biopsies at index colonoscopy (multivariate OR=0.19; 95% CI 0.04 to 0.85).59 In a modelling study, 32 random biopsies were estimated to detect dysplasia affecting ≥5% of the colon with 80% confidence.220
In a French 1000 patient community-based study, which used pan-colonic dye-spray, non-targeted biopsies (median 30 per patient) detected dysplasia in only 1.2% of colonoscopies, but in 12.8% of patients with previous neoplasia.221 Detection with random biopsies was also higher in patients with PSC and a tubular colon. A 300-patient study from the USA which used high-definition colonoscopy, with 87% performed with white light identified PSC, disease duration and active inflammation as being associated with a higher dysplasia yield on random biopsies.222 In a US study with 808 unique colonoscopies with HD-WLE and some chromoendoscopy (n=150), PSC (multivariate OR=2.1; 95% CI 1.02 to 5.07), previous polyp (OR=3.9; 95% CI 1.48 to 10.35), previous random dysplasia (OR=12.6; 95% CI 4.58 to 34.67) and moderate (OR=9.9; 95%confidence interval 2.66 to 36.94) or severe (OR=8.0; 95% CI 1.27 to 50.07) endoscopic inflammation were all significantly associated with increased dysplasia detection via random biopsies (32 biopsies mandated).218
While quadrantic random biopsies have implications for pathology resource and sustainability, only approximately 1:10 patients at high risk (8% previous dysplasia+2–3% PSC) would require these additional biopsies.
Section 5: Surveillance
5.1a Endoscopic management of dysplasia
5.1a (i) GPS: We recommend that an adenoma or serrated lesion detected outside of a colitis affected segment of the colon should be managed as dictated by sporadic post-polypectomy guidelines as the future risk of advanced neoplasia is low.
In a St Mark’s UC surveillance cohort study,28 the 5-year and 10-year cumulative incidences of CRC were only 3.2% and 6.5%, respectively, after a diagnosis of sporadic adenoma (included adenoma detected outside of a colitis-affected segment), and significantly higher at 21.2% and 32.8%, respectively, after a diagnosis of colitis-associated low-grade dysplasia. Due to the low risk, adenomas or serrated lesions which have been resected from a segment of colon where there is no macroscopic or microscopic evidence of inflammation, can be followed up as recommended in the BSG/Association of Coloproctology of Great Britain and Ireland sporadic post-polypectomy guidelines.78
The subsequent statements in the following sections are relevant only to patients who have had dysplasia detected within a colitis-affected segment (ie, where there is current or prior macroscopic or microscopic evidence of inflammation). The management pathway is summarised in figure 4.

Management and surveillance after detection of dysplasia in IBD. LDG, low-grade dysplasia; HGD, high -grade dysplasia; MDT, multidisciplinary team; PSC, primary sclerosing cholangitis.
5.1a (ii) GPS: We suggest that clearly delineated visible dysplastic-looking lesions without optical signs of invasive cancer should be considered for endoscopic resection, preferably en bloc.
Complete endoscopic resection of dysplasia from within a colitis-affected segment is associated with a low risk of advanced neoplasia progression. In a meta-analysis of 1037 patients with IBD colitis (UC, n=933; Crohn’s disease, n=126) with 1428 dysplastic lesions endoscopically resected, the pooled risk of developing CRC was 0.2 per 100 person-years follow-up (95% CI 0.0 to 0.3).223 The future risk of recurrence or post-resection progression to advanced neoplasia appears to be lowest if en-bloc resection and R0 resection margins have been achieved.224 In a multicentre cohort study of resected visible colitis-associated dysplasia (n=119), R1 resection margins were associated with a fivefold increased risk of recurrence compared with R0 resection (HR=5.06; 95% CI 0.98 to 26.2).225 R0 resection margins additionally allow for full histological evaluation to dictate the follow-up surveillance strategy required.
When a dysplastic lesion is encountered within a colitis-affected colonic segment during colonoscopy, the endoscopist should consider the optical characterisation of the lesion and the surrounding mucosa in their decision-making (see box 3), and only attempt resection at the index colonoscopy if complete endoscopic resection is likely to be achieved within the limits of their competency. En-bloc resection is unlikely to be achieved in the presence of features suggesting underlying submucosal fibrosis or invasive cancer, such as ulceration or mucosal depression, poorly defined lesion borders, irregular surface architecture, mucosal depression, tethering or surrounding active inflammation. These should prompt careful photo documentation and discussion at an MDT meeting. Biopsies of the lesion may be taken if invasive neoplasia is suspected, but otherwise best avoided if endoscopic resection is still to be considered as this might hamper future attempts by promoting submucosal fibrosis formation.
Standardised reporting of a visible dysplastic lesion should include:
Site
Morphology using modified Paris classification in accordance with SCENIC consensus statement (figure 5)
Diameter
Whether the lesion is clearly delineated
If there is an ulcer present
If there are features of submucosal fibrosis or invasion (irregular surface architecture, mucosal depression, tethering)
Evidence of surrounding inflammatory activity

Infographic summarising SCENIC IBD lesion morphology descriptors. Reproduced from Kaltenbach TR et al.329
We recommend that all patients with IBD who have been diagnosed with dysplasia, even if already endoscopically resected, are discussed in an MDT meeting to evaluate the histological grade of dysplasia and resection margins, and to achieve consensus on the recommended management and follow-up strategy (see sections 4.1c and 6.1b). Complex cases where there is uncertainty over the suitability of a lesion for endoscopic resection, or where multifocal or invisible dysplasia or indefinite for dysplasia has been detected, would benefit from an MDT meeting which includes input from an expert gastrointestinal histopathologist, IBD gastroenterologist, surgeon and an interventional endoscopist with expertise in optical characterisation of advanced colonic lesions. Centres without access to such an MDT might consider referral to a regional centre MDT meeting for advice if available.
5.1a (iii) GPS : We suggest that larger (2cm or more) non-polypoid lesions require advanced methods of resection to achieve en bloc (R0) resection.
Independent risk factors for progression to advanced neoplasia on multivariate analysis include lesion diameter and non-polypoid morphology. Dysplastic lesion size greater than 1 cm was associated with a HR 2.7 (95% CI 1.2 to 5.9) in a UK multicentre cohort study of colitis associated LGD.226 Non-polypoid morphology was associated with a HR of 8.6 (95% CI 3.0 to 24.8) in a St Mark’s cohort227 and RR 13.78 (95% CI 3.11 to 61.19) in a Belgian multicentre cohort of dysplasia.228 In a single centre cohort study on outcome of endoscopic resection of polyps>10 mm in patients with IBD, polyp size≥2 cm was associated with greater risk of recurrence with a HR 3.8 (95% CI 1.4 to 10.0) and 2 year recurrence risk estimate of 44%.229 Large non-polypoid lesions are challenging to resect en bloc due to underlying inflammation-induced submucosal fibrosis and therefore advanced polypectomy therapy such as endoscopic mucosal resection, endoscopic submucosal dissection and hybrid techniques should be considered.230 If this expertise is not available locally, referral to a regional endoscopy centre with this expertise is suggested.
5.1a (iv) GPS : We suggest that mucosal biopsies surrounding a resected lesion are not required unless there are concerns about the completeness of resection.
There is a low diagnostic yield of random biopsy specimens taken from visually non-dysplastic mucosa surrounding a polyp in patients with IBD. Dysplasia was diagnosed from none of the 300 polyp-adjacent biopsies taken in a UK tertiary single-centre study,231 and in only 7 (5.0%) of the 140 polyp-adjacent biopsies taken in a Dutch multicentre cohort study.232 Taking biopsies of a potentially resectable lesion and its surrounding mucosa is discouraged unless there are concerns about an underlying cancer. If a lesion has been endoscopically resected, but concerns remain about resection completeness from histological evaluation, then a re-look colonoscopy within 3 to 6 months, with biopsies of the polypectomy site and adjacent mucosa, to evaluate for residual dysplasia is suggested (GPS 5.3a (iii)).
5.1a (v) GPS: We suggest that all surveillance colonoscopies are performed by endoscopists with the necessary competencies.
Surveillance colonoscopies following up a prior dysplasia diagnosis should be performed by an endoscopist with competency in chromoendoscopy use and both lesion optical characterisation and IBD colitis evaluation. See section 6.2 for suggested guidance on training and section 6.1 for key performance indicators to inform the suggested competencies to perform surveillance colonoscopy.
5.1b Recommendation for consideration of colectomy
5.1b (i) GPS: We suggest surgery for dysplasia is considered for patients where the current, or future, risk of neoplasia is substantial and alternative endoscopic approaches are unsuitable.
5.1b (ii) Expert opinion: The timing of bowel resection for dysplasia must incorporate the ongoing risks of neoplastic change to support informed decision-making with the patients’ regarding surgery.
5.1b (iii) GPS: We suggest the indications for discussing bowel resection with patients with dysplastic change include:
Visible dysplasia – where endoscopic management is not possible
Invisible dysplasia – in cases where the future advanced neoplasia risk is high.
Multifocal dysplasia – where the future advanced neoplasia risk is high.
Surveillance not effective or possible—for example, very severe pseudopolyposis, strictures.
Benefit of colectomy may outweigh surveillance due to coexistent neoplasia risk factors (for example PSC, uncontrolled active inflammation).
If surgery for dysplasia is indicated an early discussion with a surgeon will facilitate the patient’s understanding of the surgical options and potential sequelae to them. Patient and MDT decision-making should take into consideration the patient’s individualised long-term overall cancer risk, based on their baseline risk factors, high-risk dysplasia features (eg, incomplete endoscopic resection, high-grade, or multifocal dysplasia) and limitations with surveillance efficacy (eg, very severe pseudopolyposis, obstructing stricture). However, a paucity of evidence exists, rendering hazardous accurate individualisation of patient risk of dysplasia progression to adenocarcinoma. In an IBD surveillance cohort study (n=12 289 patients undergoing 23 751 examinations between 2010 and 2019), where 668 patients (5.4%) developed low-grade dysplasia (LGD), the 1-, 2-, and 5-year cumulative incidence rate of progressing from LGD to HGD were 1.6%, 4.8% and 7.8%, respectively, and the 1- and 2-year cumulative incidence rates of progressing from LGD to adenocarcinoma were 0.7% and 1.6%, respectively.233 There were no significant differences in progression observed among those with unifocal and multifocal dysplasia, but PSC, male gender, a diagnosis of UC and increasing age were significantly associated with neoplastic progression on multivariate analyses. The risks of advanced neoplasia associated with invisible and multifocal dysplasia are detailed further in section 5.3.
The extent of surgery (and likelihood of stoma) depends on the indication for surgery and likelihood of synchronous or future metachronous dysplasia. Invisible and multifocal dysplasia are most likely to indicate ‘extensive’ surgical resection, such as proctocolectomy, in patients physically fit and willing to undergo such a procedure. Unifocal lesions may be amenable to limited resection if the likelihood of synchronous or future metachronous dysplasia is low. This risk has been estimated in a recent systematic review of 33 studies.224 From five studies where meta-analysis was feasible, the proportion of incidental synchronous cancers identified at colectomy was 14% for those with visible HGD, 11% with invisible HGD versus 2.7% for visible LGD and 2.4% for invisible LGD.
5.1b (iv) GPS: We suggest counselling for surgery must balance neoplasia treatment, or prevention, surgical risks/sequalae, alongside the goals of the patient, with discussions documented accordingly.
5.1b (v) Expert opinion: A full understanding of neoplasia risk as well as operative choices and post-surgical sequelae are fundamental to informed shared decision-making in cases of IBD dysplasia.
5.1b (vi) Expert opinion: Counselling and the use of decision aids might facilitate description of oncological and surgical risks to patients considering surgery.
Counselling regarding surgery for dysplasia (as prophylaxis) and cancer (for treatment) is complex. It often requires multiple and lengthier consultations. Increasingly, the use of decision aids is facilitating these consultations and can improve patients’ informed values-based choices.234 The input of a specialist stoma nurse is essential where temporary or permanent stoma is likely. There is recent international Delphi consensus guidance on how to involve patients with IBD with high-risk dysplasia in shared decision-making over their management, complete with visual decision aids.235
5.1b (vii) Expert opinion: A pragmatic approach to the extent of surgical resection (which can include segmental, subtotal, total and proctocolectomy) is warranted. The distribution and grade of dysplasia, the extent and severity of bowel inflammation, patient comorbidity, as well as informed preferences towards surgery (and stoma) will influence the extent of resection required.
Various studies examining population datasets have demonstrated that a high proportion of patients with colorectal neoplasia undergo segmental resection rather than proctocolectomy. Birch and colleagues in England,236 and Bogach and coworkers in Canada237 have demonstrated that for IBD neoplasia segmental resection is used more frequently than proctocolectomy. This is despite most historical guidelines advocating the latter—that is, ‘extensive’ resection (proctocolectomy). It requires stating that ‘limited resection’ (such as segmental colectomy) is controversial.
In comparison with sporadic CRC, IBD-CRCs tend to occur in younger patients, are more often right-sided and are associated with a poorer survival prognosis. It has not, however, been established that ‘limited resection’ for IBD-CRCs is associated with reduced survival in comparison with more extensive surgical procedures, although synchronous and metachronous dysplasia/neoplasia are feasible owing to remaining colorectal mucosa following treatment. Certainly, high-quality preoperative endoscopic assessment to exclude synchronous multifocal lesions is essential when segmental resection is being considered (see section 4.3). Various single-centre studies evaluating the use of segmental resection have observed low rates of metachronous neoplasia on follow-up (online supplemental table I).236–243 Small study populations and short follow-up duration limit the impact of some of these studies. Furthermore, one investigator followed up a cohort of 75 patients with Crohn’s colitis undergoing segmental resection for cancer and observed a 39% metachronous neoplasia rate.240 Thus a considered and pragmatic approach to surgical decision-making is warranted for patients with IBD dysplasia or cancer requiring operative intervention. Careful documentation of estimated ongoing dysplasia/neoplasia risk, acknowledging the limitations of currently available evidence in this context, is essential, as well as highlighting the need for ongoing surveillance of any remaining large bowel.
5.1b (viii) GPS: We suggest that patients who undergo limited resection (either segmental, subtotal or total colectomy with preservation of the rectum) for dysplasia or cancer, as opposed to proctocolectomy, should be offered endoscopic surveillance at 3–6 months and then annually for 5 years.
Patients who have warranted surgery for the management of dysplasia and undergone limited resection should be deemed ‘high risk’ for further dysplasia. Thus, endoscopic surveillance of the remaining large bowel is recommended 3–6 months after surgery and then annually for 5 years, provided that no dysplasia has recurred.
5.2 The role of biomarkers after dysplasia detection to guide surveillance and colectomy risk
5.2 Expert opinion: There is increasing evidence for the role of aneuploidy analysis of dysplastic lesions as a risk stratification tool for future CRC risk. However, a robust, validated technique for copy number analysis is not yet available for routine clinical practice.
Histopathological assessment of dysplasia has several limitations, most notably the interobserver variability in dysplasia grading, even among expert gastrointestinal pathologists,244 as well as tissue sampling error when using superficial endoscopic biopsies.
Chromosomal copy number alterations (aneuploidy) are a recognised, early feature of IBD-related carcinogenesis139, with aneuploidy detected in non-neoplastic colitic epithelium.140 A significant proportion of LGD lesions demonstrate aneuploidy burden at levels comparable to that of established CRCs.192 This is in stark contrast to sporadic colorectal adenomas, where large-scale aneuploidy occurs late in the adenoma–carcinoma transition.245
Published studies that aim to stratify LGD by cancer risk using aneuploidy measures are limited by their small size, and the need for large quantities of DNA from fresh tissue samples.246–248 Novel next-generation sequencing techniques, such as shallow whole genome sequencing, can reliably generate cost-effective, high-resolution chromosomal copy number profiles, even when used on archived formalin-fixed, paraffin-embedded biopsy specimens containing limited quantities of epithelium. Provisional studies using shallow whole sequencing show real promise at stratifying LGD by future cancer risk.249 Nevertheless, larger studies with prospective validation are required before the use of copy number alteration analysis in routine clinical practice.
5.3 Follow-up after visible dysplasia resected from within a colitis-affected segment
5.3a (i) GPS: We suggest that overall cancer risk is low enough for continued endoscopic surveillance to be considered the mainstay of management after complete resection of dysplasia from within a colitis-affected segment.
In a meta-analysis of 1037 patients with IBD who had 1428 colonic lesions endoscopically resected, the pooled estimated CRC incidence was low at 0.2 per 100 person-years of follow-up (95% CI 0 to 0.3).223 Estimated pooled CRC incidence was 0.5 cases per 100 person-years (95% CI 0.3 to 1.0) after endoscopic resection of polypoid dysplasia in a meta-analysis of 376 patients with UC.250 Pooled CRC incidence was higher at 3.3 per 100 patient-years (95% CI 1.2 to 8.7) after resection of non-polypoid dysplasia, using endoscopic mucosal resection, endoscopic submucosal dissection and hybrid techniques, in a meta-analysis of 96 patients with IBD.251 However, there was no progression to CRC in four of the five studies252–255 in this meta-analysis, with R0 resection rates above 70%, and CRC progression in the other study, with a lower en bloc and R0 resection rate of 40%.256 These findings justify continued endoscopic surveillance after complete resection of either polypoid or non-polypoid dysplasia has been achieved. Continued optimisation of other modifiable risk factors, such as colitis activity, are also advised to minimise future cancer risk. Summary data for aCRN rates after detection of invisible dysplasia or resection of visible dysplasia are presented in table 1.
Summary table of videoendoscopic era studies reporting on advanced neoplasia rates after detection of invisible dysplasia or resection of visible dysplasia
5.3a (ii) GPS: We suggest that polypoid LGD <2 cm, if resected en bloc, can be followed up annually for 5 years if no recurrence.
Small polypoid LGD lesions resected en bloc from a colitis-affected segment are associated with the lowest risk of CRC and therefore can undergo annual colonic surveillance. On systematic review, there were 11 studies from the videoendoscopic era where data on the incidence of advanced neoplasia could be extracted for patients followed up after endoscopic resection of polypoid colitis-associated LGD (see online supplemental table J).226 229 257–265 In a large multicentre cohort study of 211 patients with UC and 1155.2 person-years follow-up after endoscopic resection of unifocal polypoid LGD from within a colitis-affected segment, the calculated incidence of advanced neoplasia was low at 0.7 per 100 patient-years (95% CI 0.3 to 1.3).226 There was no progression to CRC over a median follow-up of up to 4 years in the three most recent studies with polypoid LGD endoscopically resected after 2010.229 258 259
5.3a (iii) GPS: We suggest that patients with high-grade dysplastic lesions or low-grade dysplastic lesions with higher risk features (polypoid ≥2 cm, non-polypoid, multifocal or that have not been resected en bloc) and who have not had a proctocolectomy, should undergo surveillance after 3–6 months and then annually for 5 years if no recurrence.
Specific features of colitis-associated dysplasia are associated with a higher future dysplasia recurrence and/or CRC risk, even if they have been endoscopically resected. These include a high grading of dysplasia (HGD), morphology that is non-polypoid, a lesion diameter ≥2 cm, or where there are multifocal lesions or the dysplastic lesion has been resected piecemeal and clear resection margins cannot be histologically evaluated. These cases warrant closer surveillance with a colonoscopy after 3–6 months before reverting to annual surveillance for 5 years if no further dysplasia is detected. For the highest risk cases (eg, HGD), follow-up with endoscopic surveillance should be considered at closer to 3 months post-resection.
Studies found on systematic review reporting on CRC incidence after resection of polypoid257 260–264 266 and non-polypoid252–255 259 260 267–270 HGD from the videoendoscopic era are presented in online supplemental tables K and L. The most recent studies reporting on endoscopically resected polypoid HGD (online supplemental table K), demonstrated either no progression to cancer over a median follow-up time of 4.3 years260 or 25% (n=3/12) progression to CRC over a median of only 1.7 years follow-up.261 Eight of the ten studies reporting on endoscopically resected non-polypoid HGD (online supplemental table L),252–255 259 260 267–270 reported no progression to CRC over a follow-up time ranging from 0.5 to 4 years. However, in two studies a CRC developed in 33.3% (n=1/3)259 to 50% (n=1/2)270 of cases over a median follow-up time ranging from 4 to 10.8 years. In a Belgian retrospective multicentre cohort study, 14.8% (n=4) of the 27 patients with IBD with visible HGD developed CRC over a median surveillance follow-up of 6.4 years (50% polyps were polypoid and 50% non-polypoid; 85% endoscopically resected).228 Although interpretation of these study results is limited by their small numbers of patients and wide-ranging results, the data support continued and early endoscopic surveillance after resection of visible HGD.
The 13 studies found on systematic review reporting on the incidence of advanced neoplasia after resection of non-polypoid LGD from the videoendoscopic era are presented in online supplemental table M.226 229 252–256 259 260 267–270 The results are again wide-ranging, with 0–40% developing advanced neoplasia over a median follow-up time ranging from 0.5 to 10 years. Two of the largest cohort studies show low CRC incidence of 0% and 1.5% and advanced neoplasia incidence up to 13.8% over a median og 4 years' follow-up. The risks associated with non-polypoid morphology and lesion diameter ≥2 cm are additionally discussed in the narrative for GPS 5.1 a (iii) and justify closer follow-up surveillance.
No studies with clear follow-up data after resection of multifocal HGD were available from the systematic review as these cases normally are referred for colectomy. Multifocality has been shown to be an independent risk factor for LGD progression to advanced neoplasia on multivariate analyses: OR=3.5 in a meta-analysis (95% CI 1.5 to 8.5; three studies)271 and HR=2.9 (95% CI 1.3 to 6.2) in a large LGD cohort from St Mark’s (n=248).226 However, in the same St Mark’s cohort, risk of developing CRC was lower at 1.7 per 100 patient-years (95% CI 0.7 to 3.5) if multifocal LGD was completely endoscopically resected versus 12.6 per 100 patient-years (95% CI 5.9 to 24.0) if multifocal LGD was not fully resected. Current evidence supports continued endoscopic surveillance after complete resection of multifocal LGD if there are no other risk factors, but the low quality of data should be acknowledged. Web tools like the externally validated UC-CaRE advanced neoplasia risk calculator226 can be useful to predict multivariate risk to facilitate decision-making. For example, the UC-CaRE calculated that the 5-year risk of advanced neoplasia if multifocal LGD lesions <1 cm in diameter were completely endoscopically resected is 7.3%; the 5-year calculated risk if at least one of the multifocal LGD lesions was ≥1 cm or greater in diameter is much greater at 18.3%. Therefore, discussions with the patient about the risks and benefits of bowel resection surgery over continued endoscopic surveillance should include individualised risk.
5.3a (iv) Expert opinion: De-escalation of colonoscopic surveillance might be considered in patients who have had 5 years of annual surveillance with no recurrence of dysplasia, and who have no high-risk patient factors.
Distinguishing sporadic dysplasia from colitis-associated dysplasia arising from field cancerisation of an inflamed colon is difficult in current clinical practice from endoscopic or histological evaluation alone. The data suggest that the majority of patients with IBD with a dysplasia diagnosis who go on to develop advanced neoplasia tend to do so in under 5 years, which might indicate an underlying field cancerisation effect.249 The median time to advanced neoplasia after a LGD diagnosis in a Dutch population-based study was 3.6 years.272 Therefore, it is suggested that patients undergoing annual surveillance after a dysplasia diagnosis can be considered for de-escalation of the surveillance interval if no recurrence or metachronous dysplasia has been detected over a 5-year period. The decision to de-escalate from annual surveillance to 3-yearly surveillance, or re-evaluation of cancer risk with a 10 year colonoscopy, should be guided by the patient’s individualised risk. This should be based on their risk factors (eg, extensive colitis) as indicated in the risk stratification algorithm in section 2.3.
5.3b Follow-up after invisible dysplasia detection
5.3b (i) Expert opinion: Invisible dysplasia is defined as dysplasia diagnosed from random biopsy taken from a mucosal site where there is no corresponding mucosal lesion visible on colonoscopy.
5.3b (ii) GPS: We suggest that if invisible dysplasia has been identified from random biopsies, a repeat colonoscopy with chromoendoscopy and segmental or mapping biopsies should be performed by a experienced IBD endoscopist within 3–6 months. The aim is to exclude a visible lesion suitable for endoscopic resection.
Estimation of the cancer risk associated with invisible dysplasia is limited by reliance on retrospective data from historical studies, where many of the ‘invisible’ lesions detected were likely to have been visible had surveillance with high-definition imaging endoscopic technologies been usual practice. A retrospective cohort study by Ten Hove et al has shown a lower incidence of invisible dysplasia over time, with 88% of the invisible LGD being detected before 2010 and 12% being detected after 2010 when chromoendoscopy and higher definition imaging were being used.273 Therefore, patients with dysplasia detected on random non-targeted mucosal biopsies should have their colonic mucosa reinterrogated by a specialist IBD endoscopist experienced in using high-definition, white-light imaging and chromoendoscopy. This is to confirm whether the dysplasia detected is truly endoscopically invisible or whether there was a missed visible lesion on the prior examination. Due to differing service capacity across endoscopy units, a logistically pragmatic timeframe of 3–6 months for the repeat colonoscopy has been suggested. However, cases associated with the highest CRC risk—that is, invisible HGD and multifocal invisible LGD, should have their repeat colonoscopy scheduled as early as possible within this time period.
Taking mapping non-targeted biopsies during this repeat colonoscopy is also suggested to assess for the presence of multifocal invisible dysplasia. In a large prospective multicentre cohort study, prior diagnosis of neoplasia was associated with an approximately 13-fold greater yield of dysplasia detection using a non-targeted biopsy protocol (2–4 biopsies every 10 cm) on multivariable analysis (OR=12.7 (95% CI 4.9 to 33.3)) even though dye spray chromoendoscopy had been used.221
5.3b (iii) GPS: We suggest that if unifocal invisible LGD is not confirmed again on repeat surveillance colonoscopy, further endoscopic surveillance is an option, and should be repeated at 3–6 months and then annually for 5 years, if there is no recurrence.
If a prior finding of unifocal invisible LGD is not reconfirmed on repeat surveillance colonoscopy performed by a specialist IBD endoscopist using dye-spray chromoendoscopy and mapping non-targeted biopsies, we suggest that endoscopic surveillance is repeated after a further 3–6 months and then annually for 5 years. If LGD is confirmed from the multiple random biopsies carried out at the repeat surveillance colonoscopy, then this should be managed as multifocal invisible LGD. Therefore, invisible dysplasia—that is, separated in ‘time’on more than one colonoscopy, or in ‘space’—that is, dysplasia seen in more than one biopsy, should be managed as multifocal invisible dysplasia.
A meta-analysis224 has suggested that the pooled estimated rate of synchronous cancers detected in colectomy specimens resected soon after a preoperative diagnosis of unifocal invisible LGD is lower in the more modern videoendoscopic era (2.4% (95% CI 0.0% to 8.5%); I2>50%; n=208) than previously reported.274–276 Systematic review of studies from the videoendoscopic era that report on CRC incidence on surveillance follow-up after invisible LGD diagnosis, identified nine studies with CRC incidences ranging widely from 0% at a mean of 4 years to 28% over a median of 2 years (online supplemental table N).227 265 273 277–282 The largest and most modern cohort study by Lightner and colleagues,278 where most of the surveillance was performed with high-definition, white-light endoscopy without chromoendoscopy, reported a low CRC rate of 2.0% (n=4/200) of the patients with CD over a median of 2.2 years (1.6–3.5) and 2.6% (n=7/275) of the patients with UC over a median of 0.5 years' (0.3–1.4) follow-up. The short follow-up time, however, should be noted. A Dutch multicentre study where high-definition chromoendoscopy were routinely used, also reported a low CRC incidence of 3.8% (n=1/26) over a median of 4.7 years' follow-up.273
5.3b (iv) GPS: If invisible HGD or multifocal invisible LGD is confirmed on repeat surveillance colonoscopy, then we suggest that a colectomy is the preferred management option rather than 3–6 monthly continued endoscopic surveillance.
The rate of synchronous cancer found in the colectomy specimen, resected soon after invisible HGD had been detected within an extent of inflamed mucosa, was 22.2% (n=8/36) in a retrospective cohort study from the Cleveland Clinic.283 A high risk of CRC was associated with an invisible HGD diagnosis in the one follow-up surveillance study found on systematic review by Lightner et al.278 CRC incidence was 27.3% (n=6/22) in the UC cohort with invisible HGD who had a median 0.5 year (0.3–1.4) surveillance follow-up period. Of nine patients with CD and invisible HGD, a third (n=3) developed CRC over the median 2.2 years (1.6–3.5) surveillance follow-up period.
Multifocal LGD and invisible LGD were found to be independent risk factors for advanced neoplasia incidence on multivariate analysis in a meta-analysis (multifocal LGD: OR=3.5 (95% CI 1.5 to 8.5); invisible LGD: OR=1.87 (95% CI 1.04 to 3.36))271 and UK multicentre cohort study (multifocal LGD: HR=2.9 (95% CI 1.3 to 6.2); invisible LGD: HR=2.8 (95% CI 1.0 to 7.5)).226
Given their high associated CRC risk, we suggest that confirmation of invisible HGD or multifocal invisible LGD should prompt a recommendation for an urgent proctocolectomy to the patient. This requires an individualised discussion between the patient and MDT using a shared decision-making approach. If the patient declines surgery or wishes to postpone, then they should be offered 3–6 monthly continued endoscopic surveillance.
5.3c Follow-up after indefinite for dysplasia detection
5.3c (i) GPS: We suggest if indefinite for dysplasia is identified after assessment by two gastrointestinal histopathologists, medical therapy should be optimised to reduce inflammation, and another surveillance colonoscopy should be performed within 3–6 months, with targeted and segmental mapping biopsies.
5.3c (ii) Expert opinion: Repeat confirmation of indefinite for dysplasia should prompt annual surveillance until active inflammation is controlled. Negative findings on repeat colonoscopy should prompt de-escalation of surveillance frequency.
The presence of active inflammation makes histological differentiation between reactive atypia and dysplasia difficult, and therefore if a biopsy or lesion is diagnosed with indefinite for dysplasia (IND), assessment by a second gastrointestinal histopathologist is recommended. A Dutch cohort study of patients with invisible IND (n=26) demonstrated a revision in the 5-year cumulative incidence of advanced neoplasia from 21% to 5% after histological re-review and reclassification by an expert gastrointestinal pathologist.281 Medical therapy should be optimised for better disease control, and another surveillance colonoscopy should be performed within 3–6 months with targeted and non-targeted segmental mapping biopsies to look for invisible dysplasia.
On systematic review, seven studies from the videoendoscopic era were found reporting on advanced neoplasia incidence after detection of IND (online supplemental table O).212 247 265 281 284–286 Advanced neoplasia progression rates range from 2.4% to 14.6% at 2 years and 4.8% to 36.5% at 5 years. The pooled risk of future advanced neoplasia after a diagnosis of IND (2.4 cases per 100 person-years (95% CI 1.2 to 3.6)) was comparable to that of LGD (2.1 cases per 100 person-years (95% CI 1.0 to 3.3)) in a meta-analysis.287 The 5-year cumulative incidences of CRC after an IND and LGD diagnosis were also similar at 24.9% and 21.2%, respectively, in a St Mark’s surveillance cohort study spanning four decades.28 However, a recent retrospective cohort study demonstrated that if the surveillance colonoscopy was repeated after an IND diagnosis and no IND or neoplasia was detected, the risk of future neoplasia was significantly lower than if IND had been reconfirmed or dysplasia was detected (3.1% vs 23.3% per patient-year; p<0.0005).285 Therefore, if no IND is detected on the repeat 3–6-month surveillance colonoscopy then patients can revert to the risk stratification algorithm to determine surveillance frequency as presented in section 2.3. If IND is reconfirmed, however, patients should undergo annual surveillance until optimisation of active inflammatory control has been achieved.
5.4 Surveillance after pouch surgery or for a retained rectum
5.4a (i) GPS: We suggest annual surveillance of the pouch or retained rectum (including a defunctioned rectal stump) for patients who have had bowel resective surgery for colitis-associated dysplasia or cancer.
5.4a (ii) GPS: We suggest surveillance of the pouch or retained rectum every 1–3 years for patients with primary sclerosing cholangitis, chronic inflammation of the pouch (pouchitis), cuffitis, CD, long duration of UC or a family history of CRC in a first-degree relative
5.4a (iii) GPS: We suggest if there are no risk factors after bowel resective surgery with ileal pouch-anal anastomosis (IPAA) or retained rectum, no additional surveillance is a reasonable option until endoscopic reassessment at 10 years.
Neoplastic lesions in patients with an IPAA include low-grade dysplasia, high-grade dysplasia, adenocarcinoma and very rarely, squamous cell carcinoma and lymphoma. The overall risk for neoplasia in patients with IBD and IPAA is low. A systematic review of 2040 patients with UC and IPAA patients reported the pooled prevalence of dysplasia involving the pouch, anal transitional zone or rectal cuff was 1.13% (95% CI 0% to 18.75%).288 A meta-analysis including 8403 patients revealed a pooled prevalence of adenocarcinoma in the ileoanal pouch of 0.5% (95% CI 0.3% to 0.6%).289 The strongest and most consistent risk factor for pouch neoplasia in patients with IBD is prior colorectal neoplasia. One Dutch registry study reported an adjusted HR of 3.7 (95% CI 1.4 to 10.2) for pouch patients with preoperative dysplasia and 24.6 (95% CI 9.6 to 63.4) for patients with preoperative CRC.290 A review of 49 pouch carcinoma cases in patients with IBD reported that 28 (57.1%) of these patients had prior colorectal neoplasia.289 Other less established risk factors for neoplasia in patients with IBD with IPAA include PSC, chronic pouchitis (arbitrary cut-off point of 4 weeks based on persistent symptoms despite therapy, or more than 3–4 acute episodes per year), chronic cuffitis, CD of the pouch, long duration of UC (a total≥8 years) and a family history of CRC in a first-degree relative.291
Pouch surveillance is a matter of controversy. While most will agree that annual pouchoscopy is indicated in high-risk patient groups, such as those with prior colorectal neoplasia,2 99 291 there is disagreement regarding pouch surveillance in patients without the above-mentioned risk factors. Previous BSG guidelines recommended either performing no surveillance or 5-yearly surveillance in this low risk group,2 the International Ileal Pouch Consortium recommend 3-yearly surveillance291 and recent ECCO guidelines recommend no surveillance at all.99 See online supplemental table P for detailed surveillance recommendations from these guidelines.
Patients with IBD who have undergone surgery but remain with their rectum in situ are at risk of rectal carcinoma. The overall risk for neoplasia in patients with IBD after total colectomy is low. In a recent systematic review and meta-analysis the pooled incidence of rectal carcinoma was calculated to be 1.3%.292 Subgroup analysis showed an incidence of 0.7% for patients with a de-functional rectal stump, and 3.2% for patients with an ileorectal anastomosis. Lower rates of malignancies were reported in the more recent studies included in this meta-analysis.
Prior colorectal neoplasia is the major risk factor for neoplasia in patients with IBD and a retained rectum. The above-mentioned systematic review and meta-analysis292 reported an adjusted HR of 5.1 (95% CI 3.1 to 8.2) for preoperative dysplasia and 7.2 (95% CI 2.4 to 21.1) for preoperative CRC. One study identified PSC and disease duration until colectomy as risk factors for rectal stump cancer.293 figure 6 summarises the recommended clinical pathway

{kind=link}
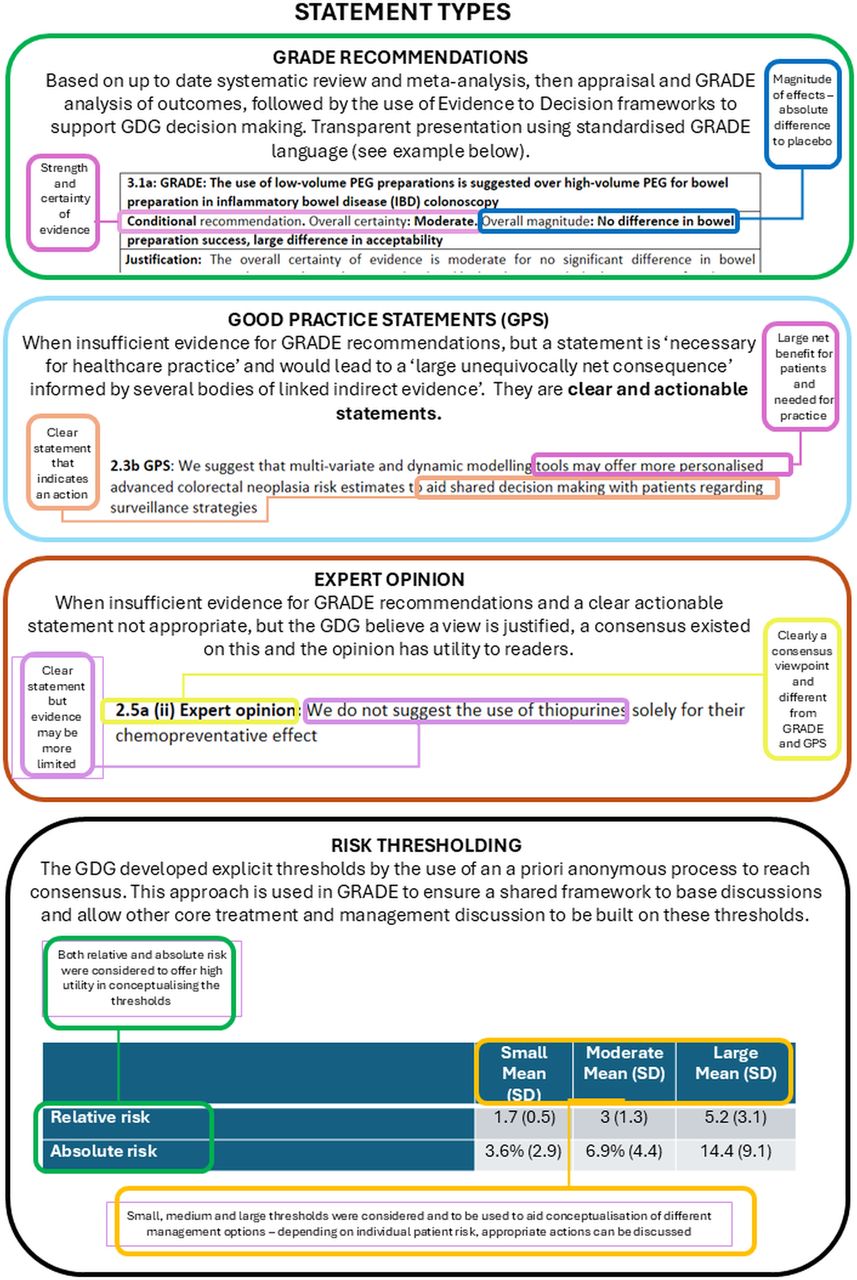{kind=link}
{kind=link}
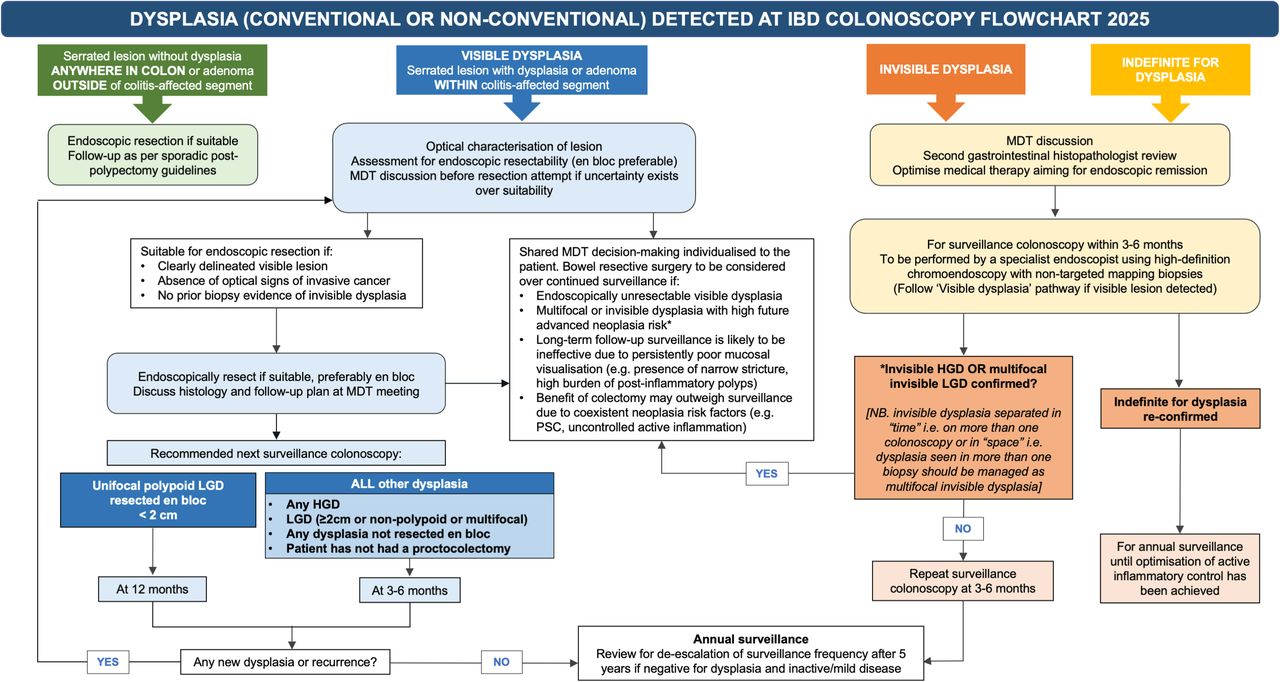{kind=link}
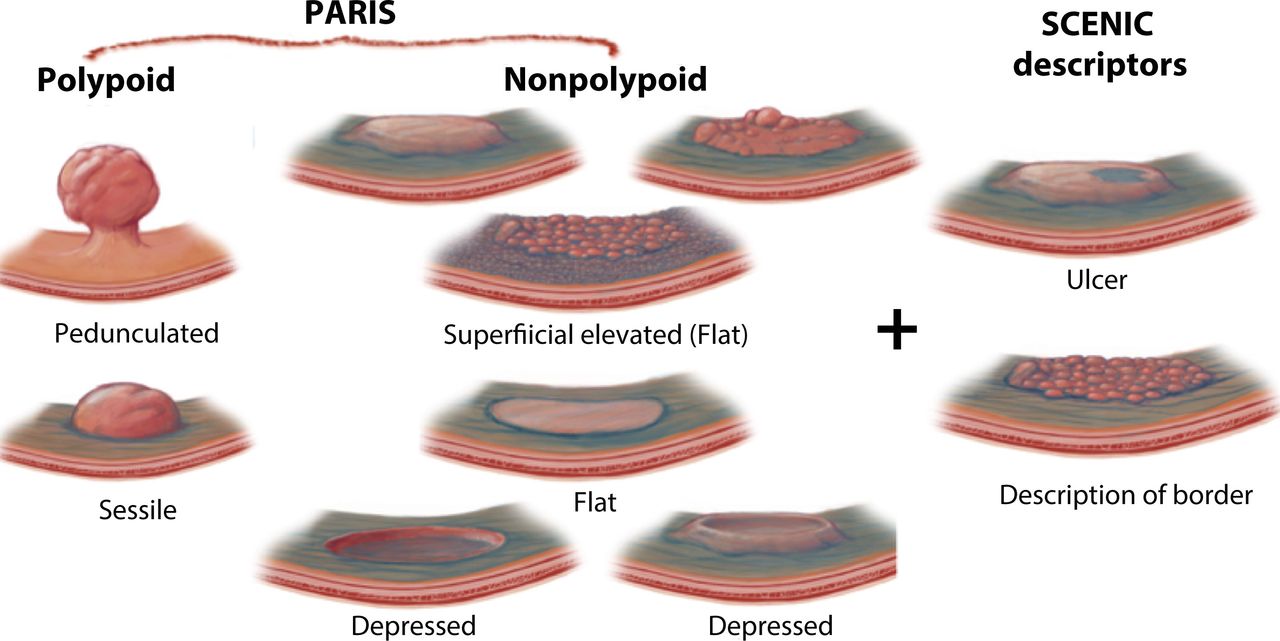{kind=link}
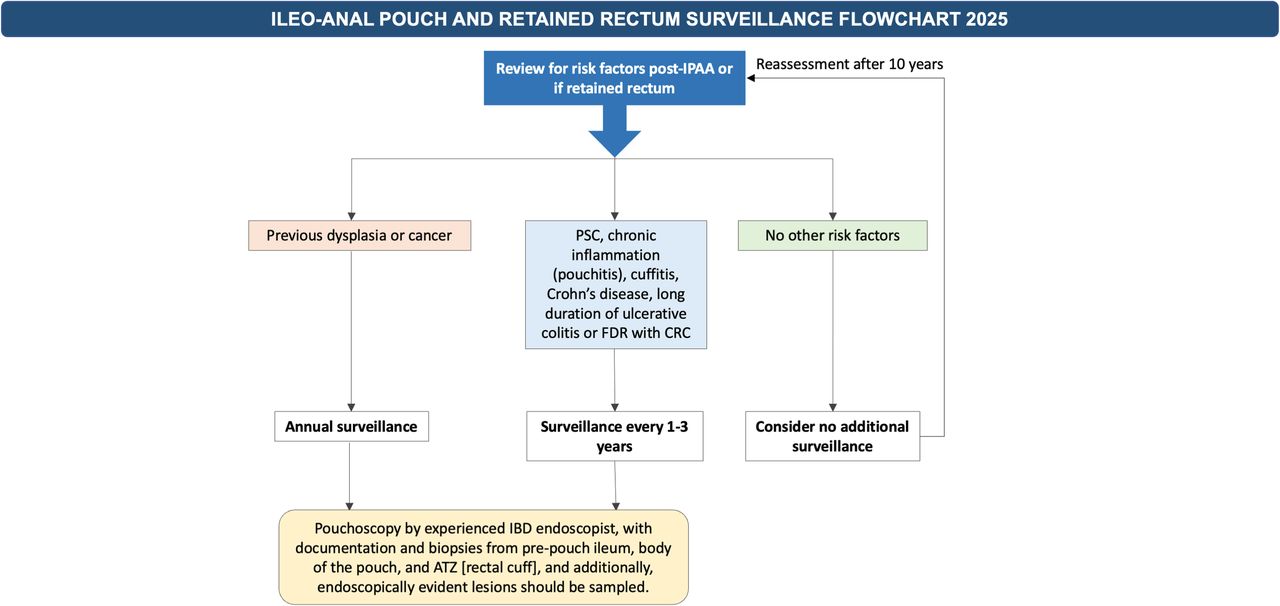{kind=link}
Management pathway for surveillance of pouch or retained rectum. ATZ, anal transition zone; CRC, colorectal cancer; FDR, first degree relative; IPAA, iIeal pouch-anal anastomosis; PSC, primary sclerosing cholangitis.
5.4b (i): GPS: We suggest that surveillance pouchoscopies are performed by experienced IBD endoscopists, with documentation, and biopsies from pre-pouch ileum, body of the pouch and anal transition zone (rectal cuff), and additionally, endoscopically evident lesions should be sampled.
5.4b (ii): Expert opinion: Multimodal assessment (for example, with examination under anaesthesia with histology and/or cross-sectional imaging) might be necessary if there is clinical uncertainty in order to detect rare lesions.
Surveillance pouchoscopies should be performed by experienced IBD endoscopists. Each pouchoscopy report should clearly describe the pre-pouch ileum, the body of the pouch and the rectal cuff, with biopsy specimens taken from each area.294 Additionally, endoscopically evident lesions should be sampled.291
Section 6: Quality, training, sustainability and cost-effectiveness
6.1 Quality in IBD surveillance colonoscopy and KPIs
6.1a Expert opinion: Endoscopists and units wishing to benchmark the quality of their colonoscopy procedures for IBD surveillance can use the modified key performance indicators from ESGE 2022 ‘Performance measures in IBD endoscopy’ position statement (see box 4).
6.1b Expert opinion: IBD colorectal surveillance service performance standards:
Modified key performance indicators from ESGE 2022 in inflammatory bowel disease (IBD) endoscopy:
Rate of reported indication for colonoscopy (≥95%).
Rate of adequate photodocumentation (≥90%).
Ileal intubation rate (≥80%).
Rate of adequate biopsies for IBD diagnosis (≥80%)
Rate of endoscopic validated activity score use (≥90%).*
Rate of high-definition endoscopy use (≥90%).*
Rate of adequate bowel preparation (≥90%) Aronchick ‘excellent’ or ‘good’; Boston bowel preparation score ≥6 and ≥2 in each segment; rate of dye-based chromoendoscopy use (≥70%).*
Minor performance measures:
Dysplasia detection rate ≥8%* (non-dysplastic serrated lesions now not thought to be IBD CRC related)
*Specific for IBD surveillance.
Italics indicates modification to the guidelines described by Dekker et al.296
IBD colorectal surveillance services should offer all eligible patients with IBD a colonoscopy 8 years after diagnosis (or at diagnosis if PSC) and within 6 months of their subsequent recommended surveillance date (minimum standard 70%, aspirational target 90%).
Patients with IBD diagnosed with dysplasia of any form within their colitis segment, including indefinite for dysplasia, should be reviewed at an MDT meeting (minimum standard 95%, aspirational target 100%).
6.1c Expert opinion: IBD colorectal surveillance services and IBD endoscopists should collect patient-reported experience measures (PREMs) for patients with IBD experiences at colonoscopy, and use the feedback received to optimise their service.
High-quality surveillance in IBD is crucial to increasing the detection rate of early colonic lesions that might progress to advanced neoplasia and cancer.295 However, heterogeneity of disease and patients’ preferences make quality standardisation difficult. The ESGE has defined KPIs for IBD to standardise patient care, improve colonoscopic quality and to reduce the risks of development of advanced neoplasia.296 Poor-quality surveillance in IBD—for example, performed with the presence of inflammation or incomplete colonoscopy, is associated with an increased risk of colitis-associated dysplasia.297 Disease activity is considered the main promoter for cancer progression in IBD, reduces accurate visualisation of dysplastic lesions in the colonic mucosa during surveillance and makes histological assessment more challenging. Accurate endoscopic assessment of the grade of inflammation using validated endoscopic scoring systems is important to define future risk and surveillance intervals. High-definition endoscopy for IBD surveillance is endorsed by all major international IBD guidelines and this guideline (section 3.2a). Online supplemental table Q summarises the key quality measures according to current international guidelines.99 295 296 298
We endorse the ESGE KPIs as core quality benchmarks for IBD colonoscopy, against which endoscopists and endoscopy units can assess their performance; however, some modifications to reflect recent data or changes from the current guideline are included (box 4).
High-quality ‘good’ bowel preparation is needed to effectively perform dye-based chromoendoscopy, which is now recommended (section 3.2b), without stool obscuring a significant portion of the mucosa. In a recent Austrian population-based study in a CRC screening programme, Aronchick ‘fair’, ‘poor’ or ‘inadequate’ was associated with a higher rate of PCCRC-related death than for ‘excellent’ or ‘good’ HR=2.56 (95% CI 1.67 to 3.94).299 Therefore, Aronchick ‘fair’ preparation would not be acceptable in IBD colonoscopy, nor would a BBPS of 1 or 0 in any segment.300 Virtual chromoendoscopy is no longer recommended (section 3.2c).
We have retained the detection rate for dysplasia (low-grade dysplasia, high-grade dysplasia or cancer including non-conventional dysplasia, within the colitic segment) rather than neoplasia at ≥8% on the basis of the GETAID 1000 patient chromoendoscopy study (rate 8.2%, all high-definition chromoendoscopy) and a recent 600 patient Canadian study at 12 centres, which achieved similar detection rates (rate 7.5%, all high-definition white light, 50% random biopsies, no chromoendoscopy).221 301 Serrated lesions without dysplasia are not now thought to be precursors of IBD-associated CRC (section 4.2b).
At an IBD colorectal surveillance service level, the fundamental issues are whether the patients receive surveillance at the appropriate intervals for their risk, and if dysplasia is detected, that it is appropriately managed. Neither of these operational issues have received much attention in guidelines in the past. Concordance with IBD surveillance is poor in the UK and internationally for a range of reasons, and is associated with IBD PCCRC (sections 1.4a and 1.3b). Dysplasia and early cancer cannot be detected at a curable stage if patients do not receive timely colonoscopy. Levels of concordance with initial risk assessment at 8 years for all patients with IBD with colonic disease beyond proctitis, and subsequent surveillance intervals above 70%, are achievable, but require organisation and systematic, automated and personalised reminders (section 1.4b).
Dysplasia or cancer detection within the colitis segment is a significant event for patients with IBD and the team treating them, raising challenging questions about inflammatory control, intensive endoscopic surveillance, advanced endoscopic therapy or major resectional surgery. It is therefore appropriate that in all cases where dysplasia is suspected within the colitis segment that input is sought from an appropriately constituted MDT (section 4.1 c).235
Patients can experience feelings of shame and inferiority at repeated colonoscopies, which remind patients of a lifelong disease, but colonoscopy is also potentially life-saving.302 Patients with IBD are more likely than other patient groups undergoing colonoscopy to find the procedure embarrassing, burdensome and painful.303 Unfortunately patient perceptions of pain, which were moderate or severe for 65.8% of a UK IBD cohort, correlated only weakly with the perception of the endoscopist (r=0.225; p=0.015).304 Patients rate control of discomfort, adequate endoscopist technical skill and effective communication as the most important aspects of their experience.305 In order for colonoscopic screening programmes in IBD to be successful, patients need to return repeatedly for colonoscopy. Therefore, individual IBD endoscopists and endoscopy units need a clear and detailed understanding of the patient experience they are providing to improve and optimise their service. Periodic collection of the colonoscopy experiences of patients with IBD with a validated tool such as Newcastle ENDOPREM, and actioning feedback received, will improve patient experience.306
6.2 Training in IBD surveillance colonoscopy and KPIs
6.2a GPS: We suggest that endoscopists performing surveillance endoscopy in IBD should acquire the necessary skills to diagnose IBD-related lesions accurately during their training.
6.2b GPS: We suggest that endoscopists performing surveillance endoscopy in IBD should audit and review their results within the service's governance structure and as part of their local appraisal process to demonstrate sustained competence.
6.2c Expert Opinion: Owing to both the diagnostic challenges of IBD surveillance, and the imperative to maintain patient comfort to maximise ongoing patient concordance with surveillance, we suggest that IBD surveillance is limited to a small number of dedicated and appropriately IBD-trained colonoscopists within an organisation.
IBD surveillance is the most challenging diagnostic colonoscopic procedure, due to the wide range of subtle neoplastic appearance, which overlaps with a wide range of inflammatory and post-inflammatory appearances. There is, therefore, a need for training in IBD surveillance, both for the dye-spray technique and for optical diagnosis.
Training in colonoscopy in the UK uses a standardised certification process,307 based on the UK key performance indicators and quality assurance for colonoscopy.308 Neither the quality assurance standards nor the Joint Accreditation Group (JAG) certification process include training in IBD surveillance. Previous BSG IBD surveillance guidelines did not provide advice on the acquisition of the skills required to perform the procedure.1 The international SCENIC consensus document recognised the need for training in endoscopic IBD surveillance.3 However, routine training and incorporation in national guidance has not occurred in the UK (online supplemental table R).1–3 307–310
The ESGE published a position statement to guide endoscopists on optical diagnostic skills.309 Evidence of the efficacy of training to improve outcomes from surveillance endoscopy has been lacking. However, Iacucci et al have improved accuracy with the online OPTIC-IBD training system, and showed sustainability in confidence and accuracy in lesion recognition.310 The new English regional endoscopy academies and their equivalents in the devolved nations, together with JAG and its stakeholders, should develop appropriate IBD surveillance training. There is also an opportunity to use dedicated lists to provide focus and maximise learning for endoscopists wishing to acquire the skills.
More than for almost any other colonoscopic procedure, patient comfort in IBD surveillance is imperative. This is because such patients will often undergo dozens of procedures during their lifetime; just one bad experience might result in the patient declining further surveillance, to the detriment of their long-term care. This is a further reason why IBD surveillance should be performed by a small number of dedicated experienced colonoscopists within an organisation. If colonoscopy cannot be achieved comfortably by an expert colonoscopist with conscious sedation, propofol deep sedation should considered, which has been shown to improve patient pain scores and satisfaction in a RCT of patients with IBD.311
6.3 Sustainability in IBD surveillance endoscopy (green endoscopy)
6.3a Expert opinion: Adherence to a targeted biopsy strategy incurs a lower carbon footprint than a non-targeted one, but more intensive surveillance (ie, more colonoscopy) would increase environmental impact overall. Research is needed to determine the magnitude of effect, given that a proportion of patients might be directed toward less frequent colonoscopic surveillance.
A worldwide interest in the environmental impact of healthcare has begun to influence the clinical practice and delivery of endoscopy.312 The overriding concern in a surveillance programme, where alternatives to colonoscopy are not available (or appropriate), is not to reduce the ‘absolute’ environmental impact but to minimise ‘wasteful’ procedures: ensuring appropriateness, optimising preparation and reducing the need for patient travel.
Four variables have most impact in surveillance colonoscopy for IBD: overall procedure numbers resulting from adherence to guidance; avoidable repeat procedures due to inadequate bowel preparation; a targeted biopsy strategy; and the impact of treating late-stage disease if surveillance fails (or is not deployed).
The carbon footprint (measured in carbon dioxide equivalents: CO2e) of colonoscopy varies considerably internationally, estimated as between 6 and 29 kg CO2e, and depends on whether analysis ‘boundaries’ extend to include patient and staff travel. Single-use instruments contribute minimally (estimated 0.31–0.57 kg CO2e per accessory313), whereas histology specimens incur 0.29 kg CO2e per ‘pot’. Following a targeted biopsy strategy or combining multiple biopsies into one specimen container would reduce this carbon footprint.
Improved concordance with guidelines will balance an increase in appropriate ‘index’ colonoscopy against a reduction in surveillance procedures. Reported guideline concordance varies considerably (27–72%314; see section 1.4). There are no data on the numerical impact of concordance (ie, patients not offered surveillance when they should vs those inappropriately offered or subjected to inappropriately long—or short—intervals).
These updated guidelines, overall, will ensure healthcare resource is used most appropriately with a focus on outcomes.
6.4 Cost effectiveness
6.4a Expert opinion: Colonoscopy for surveillance in IBD may be cost-effective at incremental cost-effectiveness ratios supported by NICE; however, very limited UK practice-specific data are available.
In general, NICE considers interventions with incremental cost-effectiveness ratios (ICERs) below £20 000 to be cost-effective,315 and those with ICERs between £20 000 and £30 000 may be an effective use of NHS resources. Our systematic search identified seven studies that evaluated the cost-effectiveness of colonoscopic surveillance in IBD (online supplemental table S).316–322 NICE, in the 2011 guidelines on ‘Colonoscopic surveillance for prevention of CRC in people with ulcerative colitis, Crohn’s disease or adenomas’, constructed a Markov model for those at highest risk, which had an ICER of £17 557 using UK costs. Of the six other studies identified, five also reported ICERs for IBD colonoscopic surveillance that would be below the NICE £20 000 threshold across a range of countries, healthcare system costs and baseline disease states. Longer surveillance intervals and the use of chromoendoscopy with targeted biopsies were associated with increased cost-effectiveness; however, the Markov models used have considerable uncertainly related to transitioning between disease states, as the biology of the progression from low-grade dysplasia to high-grade dysplasia to cancer is much less well understood for IBD-related carcinogenesis.
Areas of future research
During the development of this guideline, the GDG identified key areas in need of further research that will facilitate future priority setting partnerships and these are shown in Box 5.
Future research questions and areas
Epidemiology
Post-colonoscopy colorectal cancer (PCCRC) rate analyses in inflammatory bowel disease (IBD) need further study, either using PCCRC 1-year rates and/or taking colorectal cancer (CRC) stage into account.
How can we digitally link to patient data in identifying, scheduling and reminding patients (and clinicians), on surveillance dates for individual patients, to aid surveillance concordance?
Risk stratification
What is the performance of single ‘top’ relative risk factor versus multivariate risk factor calculators in safely and effectively defining surveillance intervals to reduce CRC risk?
Given current but retrospective risk ratios related to sex and IBD CRC, how can we assess the current built-in assumption of less risk in women in models, which may be not correct be for current and future CRC outcomes?
How does the combination of IBD and hereditary CRC syndromes influence cancer risk cumulatively and what is the optimal surveillance interval in these patients?
Does 5-aminosalicylate have a directly chemopreventive effect against advanced colorectal neoplasia benefit independent of inflammatory control?
How can patients with IBD to be supported to optimise modifiable factors on CRC risk?
Colonoscopy
How can bowel preparation be improved for patients with IBD?
What level of bowel preparation is required to perform chromoendoscopy effectively in patients with IBD?
Large, randomised studies on IBD-specific artificial intelligence systems are required before they can be recommended clinically.
Stool-, blood- and biopsy-based biomarkers are promising tools to risk stratify patients with IBD; however, large prospective trials are required, and clinically validated laboratory tests are needed before clinical deployment.
Pathology
Is serrated epithelial change (SEC) a consequence of previous longstanding inflammatory disease or a separate risk factor for CRC in its own right?
What does a non-conventional dysplasia diagnosis in IBD mean for prognostication of future CRC risk and the role of biomarkers, and how can we to improve interobserver pathologist concordance?
Surveillance
What is safe time to de-escalate annual surveillance following dysplasia detection in IBD where we can be confident that field cancerization has not occurred?
Quality, training, sustainability and cost-effectiveness
How can we effectively train endoscopists in IBD endoscopy at scale and (re-)assess competence (digitally)?
What is the cost, waiting list impact and carbon footprint of 50%, 75%, 100% concordance with IBD colorectal surveillance guidelines?
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We are grateful for the contributions of our patient representatives, Caroline Brocklehurst and Vicky Buckley. We also thank Anshul Thakur, University of Oxford, for his assistance in developing the code for the multivariate risk prediction web calculator, and Nicholas Sutton, Crohn’s and Colitis UK for feedback on the patient-friendly summary. We thank Anouk Wijnands, Sjoerd Elias, Bas Penning de Vries and Bas Oldenburg, Universitair Medisch Centrum Utrecht, for support in developing the multivariate risk prediction web calculator. We thank Professor David Wilson, University of Edinburgh, for assistance with paediatric onset IBD special circumstances. The authors acknowledge the following funding sources: AD has received research funding from NHSE, NIHR and Innovate UK. CAL acknowledges research support from the NIHR Newcastle Biomedical Research Centre, Medical Research Council, Helmsley Charitable Trust, Crohn’s & Colitis UK, EU Innovative Medicines Initiative, Wellcome Trust, Open Targets, European Bioinformatics Institute (EMBL-EBI), Janssen, Takeda, Abbvie, AstraZeneca, Eli Lilly, Orion, Pfizer, Roche, Sanofi Aventis, UCB, Biogen, Genentech, Bristol Myers Squibb (BMS), GSK, and Merck Sharp and Dohme (MSD). GBN is supported by a National Institute for Health and Care Research (NIHR) Doctoral Research Fellowship (grant number 302607). JEE is supported by the NIHR Oxford Biomedical Research Centre. SDi acknowledges funding from NHS Lothian RD. SJL has received funding from CRUK Early Detection and Diagnosis project award (25901), CRUK Program Grant (DRCNPG-Jun22\100002) and the Wellcome Trust Senior Clinical Research Fellowship (206314/Z/17/Z).
Authors without specific funding to report have stated this explicitly. No other funding was received for the development of this manuscript. The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR or the Department of Health.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
JEE and MG are joint first authors.
NJT and AJM are joint senior authors.
X @drmorrisgordon, @ShahidaDin1, @DrChrisLamb, @anjan_dhar6, @sdolwani, @DrBuHayee, @chris@airedaledodger
Contributors JEE, MG, GBN, and VSi formed the core group responsible for coordinating the guideline development process. Section leadership was as follows: CAL led Section 1, SDi led Section 2, AW led Section 3, AB led Section 4, MK led Section 5 and MI led Section 6. JEE, MG, GBN, VSi, AB, SDi, MI, MK, CAL, AW, IAB, AD, SDo, OF, AH, BH, CH, SJL, MRN, TR, MDR, NS, VSu, MV, RW, LW, NJT and AJM contributed to the guideline development through participation in the voting process, as well as drafting, reviewing and editing the manuscript. JEE and MG served as co-chairs of the Guideline Development Group (GDG) and are guarantors for the overall content. GBN and VSi are shared second authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests All authors have completed the ICMJE uniform disclosure form. The following competing interests are reported: AH has received consulting fees, lecture fees, honoraria, or advisory board fees from AbbVie, Abivax, BMS, Celltrion, Falk, GSK, Eli Lilly, J&J, Pfizer, and Takeda. She is a governing board member of ECCO (since 2018) and a scientific board member of Crohn's and Colitis UK (since 2011). AD has received honoraria, advisory fees, consultancy fees, speaker fees and hospitality from Tillotts Pharma (UK), Dr Falk Pharma UK, Takeda, BMS, Lilly, Abbvie UK, Pharmacosmos UK, Johnson and Johnson, Celltrion, Amgen, Alfasigma and Boston Scientific Corporation Inc. CH is employed as a JAG assessor, with JAG using standards to guide the assessment of endoscopy units for accreditation.
CAL has provided consultancy for MSD, Eli Lilly, Janssen and BMS, and has received honoraria for educational activities from Takeda, Ferring, Janssen, Dr Falk and Nordic Pharma. He has also received conference attendance support from Tillotts Pharma UK, Janssen, BSG, IOIBD and ECCO. CAL is a steering committee and board member of IBD UK and was secretary of the IBD section committee of the British Society of Gastroenterology (2021–2024). AB has received lecture and advisory board fees from Dr Falk and is the secretary of the colorectal section of the BSG. AJM has received speaker honoraria from AstraZeneca and Medtronic and conference attendance support from Tillotts Pharma.
LW has served on advisory boards for Pfizer, BMS and Dr Falk and has received speaker’s honoraria from Takeda, Eli Lilly, Galapagos and BMS. She has also received conference attendance support from Ferring and Eli Lilly and receives editorial royalties for the Inflammatory Bowel Disease Nursing Manual. MI has received grants from the Helmsley Charitable Trust, Eli Lilly and Olympus, as well as payments for lectures or educational events from Pentax, Eli Lilly, and Pfizer. Additionally, she has received equipment or materials support from Pentax. MDR is the regional endoscopy advisor for NHS England (since 2021) and chair of JAG (since 2023).
MG serves as an editor for Cochrane, supporting clinical truth-unbiased synthesis (ongoing). NJT serves on the advisory board for Dr Falk UK concerning eosinophilic esophagitis and Jorveza, and his department receives research support, speaker fees and conference attendance support from Dr Falk UK. RW is an employee of Crohn's & Colitis UK (since October 2019). SDi is chair of the BSG IBD section (2024–2027) and holds roles in the Scottish Government and MHRA advisory groups, as well as being a gastroenterology specialty advisor for the Royal College of Physicians. SJL has received research grants from UCB Pharma. TR has undertaken paid consultancy for various pharmaceutical companies since 2020 and is a director of Endoread Ltd (since 2022). JEE serves on clinical advisory boards for Exact Sciences, Cosmo Pharmaceuticals and Satisfai Health, holds share options in Satisfai Health, and has received speaker fees from Falk, Janssen and Medtronic.
All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.