Article Text

Abstract
Objective To investigate the predictive value of the Diverticular Inflammation and Complication Assessment (DICA) classification and to develop and validate a combined endoscopic-clinical score predicting clinical outcomes of diverticulosis, named Combined Overview on Diverticular Assessment (CODA).
Design A multicentre, prospective, international cohort study.
Setting 43 gastroenterology and endoscopy centres located in Europe and South America.
Participants 2215 patients (2198 completing the study) at the first diagnosis of diverticulosis/diverticular disease were enrolled. Patients were scored according to DICA classifications.
Interventions A 3-year follow-up was performed.
Main outcome measures To predict the acute diverticulitis and the surgery according to DICA classification. Survival methods for censored observation were used to develop and validate a novel combined endoscopic-clinical score for predicting diverticulitis and surgery (CODA score).
Results The 3-year cumulative probability of diverticulitis and surgery was of 3.3% (95% CI 2.5% to 4.5%) in DICA 1, 11.6% (95% CI 9.2% to 14.5%) in DICA 2 and 22.0% (95% CI 17.2% to 28.0%) in DICA 3 (p<0.001), and 0.15% (95% CI 0.04% to 0.59%) in DICA 1, 3.0% (95% CI 1.9% to 4.7%) in DICA 2 and 11.0% (95% CI 7.5% to 16.0%) in DICA 3 (p<0.001), respectively. The 3-year cumulative probability of diverticulitis and surgery was ≤4%, and ≤0.7% in CODA A; <10% and <2.5% in CODA B; >10% and >2.5% in CODA C, respectively. The CODA score showed optimal discrimination capacity in predicting the risk of surgery in the development (c-statistic: 0.829; 95% CI 0.811 to 0.846) and validation cohort (c-statistic: 0.943; 95% CI 0.905 to 0.981).
Conclusions DICA classification has a significant role in predicting the risk of diverticulitis and surgery in patients with diverticulosis, which is significantly enhanced by the CODA score.
Trial registration number NCT02758860.
- diverticular disease
- endoscopy
Data availability statement
Data are available upon reasonable request.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Diverticulosis, the most frequent anatomical alteration of the colon, is increasing worldwide.
The first endoscopic classification of the diverticulosis/diverticular disease, named Diverticular Inflammation and Complication Assessment (DICA) classification was recently developed.
A first retrospective study found this classification predictive on the risk of developing acute diverticulitis and undergo surgery.
What are the new findings?
This large (2215 patients), prospective, cohort study collected patients in 43 centres located in Europe and South America, who were prospectively followed-up for 3 years.
The DICA endoscopic classification is as clear predictor of the outcomes of diverticulosis/diverticular disease. It is enhanced by the Combined Overview on Diverticular Assessment (CODA) score, which combined clinical and endoscopic finding.
Significance of this study
How might it impact on clinical practice in the foreseeable future?
The CODA score, combining DICA and few clinical parameters, may reliably predict the occurrence of acute diverticulitis and surgery due to complications, thus providing a new risk stratification tool useful for daily clinical practice.
For the first time, we have a reliable tool to predict the temporal evolution of the disease.
Introduction
Diverticulosis is an anatomical alteration of the colon, characterised by the detection of pockets generally involving mucosa and submucosa.1 Its prevalence is high but stable in the Western world,2 while it is increasing in developing world as well as Asia.3–6 Diverticulosis is the most frequent structural alteration of the colon diagnosed at colonoscopy.7 Just 20% of people having diverticulosis may have symptoms’ occurrence linked to the diverticula, developing the so-called ‘diverticular disease’.
Until 2015, diverticulosis and diverticular disease did not have any endoscopic classification, and the available classifications were based on imaging8–10 or on clinical features of the diverticular disease.11–13 The absence of an endoscopic classification was quite surprising, considering the frequency of the finding,1 the high number of colonoscopies performed worldwide and the chance to find endoscopic signs of diverticular inflammation in up to about 2% of patients undergoing colonoscopy.14–16
In 2015, the first endoscopic classification of diverticulosis/diverticular disease of the colon was presented.17 The Diverticular Inflammation and Complication Assessment (DICA) classification takes into account few endoscopic findings of the colon with diverticula,17 and was developed in order to have an objective method to describe the colon with diverticulosis and its characteristics. It was validated by two studies,18 19 and a first retrospective study found this classification predictive on the risk of developing acute diverticulitis and undergo surgery.20
Thus, we aimed to perform a larger prospective, international cohort study in order to confirm the predictive value of the DICA classification and to develop and validate a novel clinical score (named Combined Overview on Diverticular Assessment, CODA) predicting diverticulitis and surgery, including DICA classification as the main item.
Methods
Study design and population
This multicentre, prospective cohort study aimed to (i) evaluate the prognostic performance of the DICA endoscopic classification in predicting clinical outcomes (diverticulitis, and surgery due to complications), (ii) develop a novel endoscopic-clinical score for predicting diverticulitis (CODA score) in a derivation cohort comprising 35 centres located in Italy and England and (iii) externally validate the CODA score in 8 centres located in Poland, Romania, Lithuania, Brazil and Venezuela (validation cohort). Development and validation of the CODA score were performed and reported in agreement with the Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) guideline.21 The study has been conducted according to the World Medical Association Declaration of Helsinki of the 1975. All study participants provided informed written consent prior to endoscopic investigation and to take part in this study. The study was recorded at www.ClinicalTrials.gov.
Endoscopic classification of diverticulosis was made according to DICA classification.17 18 The DICA classification consists of four main endoscopic items and some subitems, each of which has a specific numerical score: adding up the scores of each main item and of each subitem, DICA score can be built. Therefore, we can have three scores: DICA 1 (up to 3 points); DICA 2 (4–7 points); DICA 3 (more than 7 points) (online supplemental table S1).
Supplemental material
Further details concerning study design, eligibility criteria and the DICA classification can be found in the online supplemental appendix.
Outcomes of the study/statistical analysis
Prognostic performance of the DICA endoscopic classification
We evaluated the prognostic performance of the DICA classification in predicting diverticulitis (primary outcome) and surgery due to complications of diverticulitis (secondary outcome) by means of time-to-event (survival) methods for censored observations. Time to event was defined as the time from baseline visit until the date of event or censoring. Kaplan-Meier estimates were used to draw cumulative incidence curves, compared by log-rank tests, as well as by univariable Cox proportional hazards (PH) analysis.
An additional outcome was the development and validation of a CODA score model.
CODA score model development
The outcome considered for model development was diverticulitis. Candidate predictors included the following variables at baseline visit: age, gender, body mass index (BMI), DICA classification, smoking (current, former or never), appendectomy, Charlson score, cumulative symptomatic score and its component scores for abdominal pain, bloating, diarrhoea and constipation. Considering the rather small number of candidate predictors, the size of the derivation cohort (n=1732) and the number of observed events (n=130) were considered adequate to achieve sufficient accuracy and precision of model estimates.21 22 No data were missing for outcome measures and candidate predictors.
We conducted explorative univariable Cox PH analysis to assess associations between each candidate predictor and diverticulitis. We inspected pairwise correlations among continuous variables (correlation matrix: online supplemental table S2). We used a backward selection procedure starting from the saturated model and eliminating candidate predictors not significant in the multivariable framework. The best fitting model was selected according to the lowest Akaike information criterion.1 The PH assumption was examined on the basis of Schoenfeld residuals. As this assumption was violated by the continuous variable ‘age’ due to a non-linear response over time, we have dichotomised this predictor at 65 years. Other variables were treated as continuous.
We assessed model discrimination using the Harrell’s c-statistic, which quantifies the ability of the model to identify patients who will experience diverticulitis.21 The Brier score for right-censored data (which equals 0 for a perfectly accurate model) was calculated as a measure of predictive accuracy, and the Nagelkerke’s R2 for PH models for censored survival data were employed as a measure of overall performance.1 Additional information about these performance indexes can be found in the online supplemental appendix (pp. 2‒4).
We built the CODA score by converting the multivariable model’s beta coefficients to integer values, while preserving monotonicity and simplicity.1 Tables and nomogram plots were produced to transform all possible total point scores into 1-year, 2-year and 3-year absolute risk of event. Though the CODA score was developed to predict diverticulitis, its overall performance in predicting surgery due to complications was also tested.
CODA score model validation
We carried out the internal model validation in the derivation cohort using a bootstrap resampling process to provide an unbiased estimate of its performance.21 We performed 100 bootstrap runs with replacement and, on each run, assessed the ‘apparent’ performance (ie, c-statistic, Brier score, Nagelkerke’s R2) and the ‘test’ performance. The difference between ‘assessed’ and ‘test’ performance was averaged across all bootstrap samples, providing an estimate of model optimism. The entire model selection process was repeated at each bootstrap run. Optimism-corrected performance measures were calculated as the original ‘apparent’ estimates minus the optimism.
Model fitness was checked by using the Grønnesby and Borgan test.23 Calibration was evaluated by plotting the observed proportion versus predicted risk of diverticulitis and reporting the calibration slope (which should equal 1 for a perfectly calibrated model).21 We accompanied the calibration slope with a test for calibration intercept equals 0 and slope equals 1, as appropriate.21 Further information about our methodology can be found in the online supplemental appendix (pp. 2‒4).
To assess external validity, we applied the CODA score to each patient included in the validation cohort based on his/her respective predictor values and used it to calculate the 3-year risk for each individual. The CODA score model fitness was checked in the validation cohort by means of Grønnesby and Borgan test.23 Calibration was investigated by plotting the observed proportion versus predicted risk and calculating a calibration slope with intercept. The external performance of the c-DICA score in predicting the primary and secondary study outcomes was assessed using the Harrell’s c-statistic, Brier score and Nagelkerke’s R2.
To explore non-linear associations, we also carried out an alternative model selection and validation process using fractional polynomial terms.24 25 In comparison, however, the model assuming a linear association between predictors and outcome performed similarly, while retaining interpretability and ease of use.
Stata software was used for statistical modelling and analysis (StataCorp). P values <0·05 were considered statistically significant. All tests were two-sided.
The corresponding author had full access to the study data and had the final responsibility for the decision to submit for publication.
Results
This multicentre, prospective, international cohort study recruited 2215 patients with diverticulosis; however 17 patients attended exclusively the baseline visit and were therefore excluded from the study. The remaining 2198 patients were followed for an average of 2.8 years.
Recruitment occurred in 43 centres located in Italy (77.2%; n=1696), Poland (12.5%; n=275), Brazil (4.0%; n=87), Lithuania (2.3%; n=50), Venezuela (1.6%; n=37), UK (1.6%; n=36) and Romania (0.8%; n=17). Baseline demographic and patients’ characteristics are reported in table 1. Patients were predominantly women (51.7%) with a median age of 66 years (IQR, 58‒74). DICA classification was associated with cumulative symptoms, abdominal pain, meteorism, constipation and diarrhoea scores (table 1).
Baseline demographic and clinical characteristics of the overall cohort and stratified by DICA groups
A total of 162 diverticulitis events, and 43 surgeries due to complications, occurred during follow-up. The cumulative incidence of diverticulitis was 26.3 per 1000 person-years corresponding to an estimated 3-year risk of 7.5% (95% CI 6.5% to 8.7%). The cumulative incidence of surgery due to complications was 7.0 per 1000 person-years corresponding to an estimated 3-year risk of 2.0% (95% CI 1.5% to 2.7%).
Development and validation cohorts
The development cohort (35 centres in Italy and England) included 1732 patients, while the validation cohort included 466 patients (8 centres in Poland, Romania, Lithuania, Brazil and Venezuela). Baseline demographic and patients’ characteristics of the two cohorts are reported in table 2.
Baseline demographic and clinical characteristics of the derivation and validation cohorts
One hundred and thirty diverticulitis and 37 surgeries occurred in the development cohort. The 3-year risk of diverticulitis and of surgery were 7.66% (95% CI 6.49% to 9.03%) and 2.19% (95% CI 1.59% to 3.02%), respectively. In the validation cohort, the 3-year risk of diverticulitis and of surgery were 6.97% (95% CI 4.98% to 9.71)% and 1.32% (95% CI 0.60% to 2.92%), respectively. Although the patients’ characteristics significantly differed between the two cohorts, the cumulative incidence of diverticulitis and surgery were not significantly different (log-rank: p=0.61 and p=0.24, respectively).
DICA endoscopic classification as a predictor of clinical outcomes
As DICA is an existing endoscopic classification, we did not apply the development and validation steps for prognostic scores. Instead, we evaluated its performance measures in predicting clinical outcomes in the overall data set, and, as sensitivity analyses, we reported the same measures for the derivation and validation cohorts.
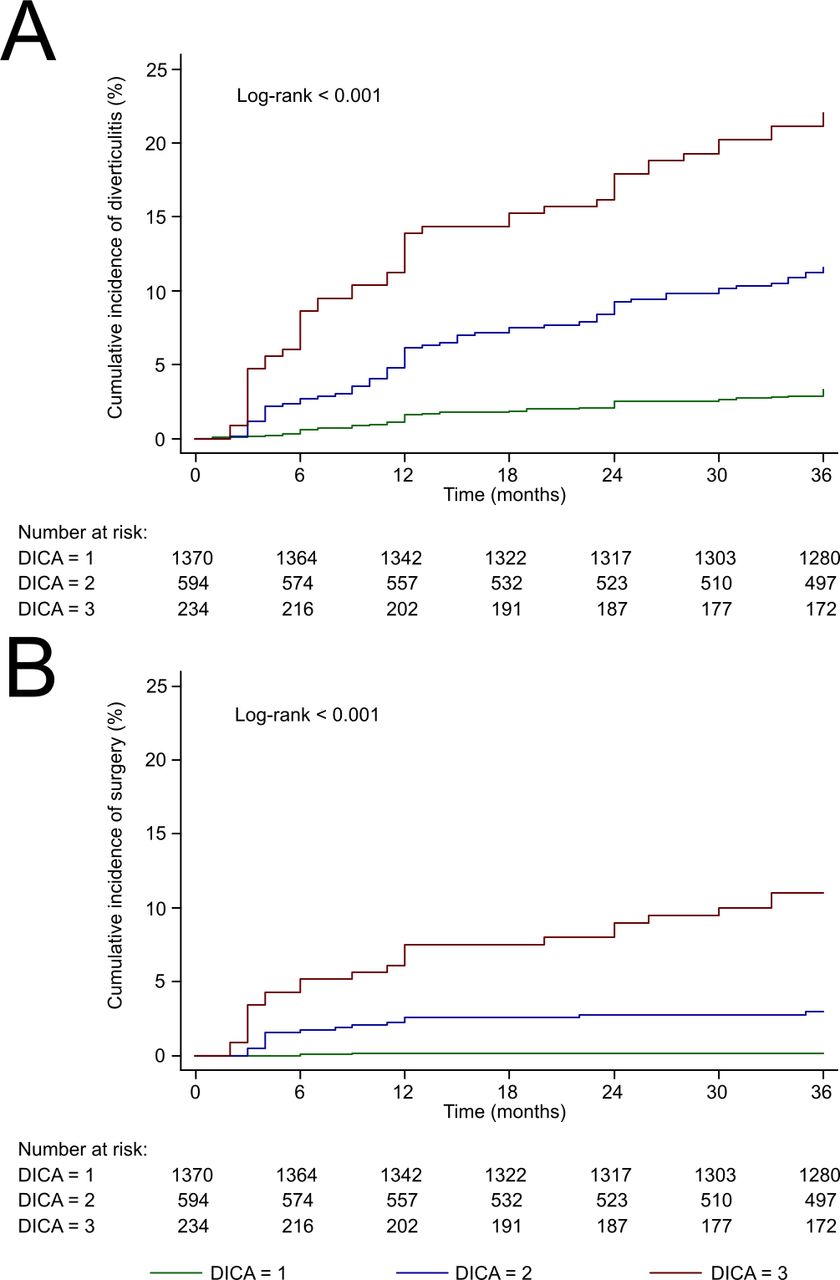
In the overall study population, the Kaplan-Meier curves stratified by DICA showed an estimated 3-year cumulative probability of diverticulitis of 3.3% (95% CI 2.5% to 4.5%) in patients with DICA equal 1, 11.6% (95% CI 9.2% to 14.5%) in patients with DICA equal 2 and 22.0% (95% CI 17.2% to 28.0%) in those with DICA equal 3, which significantly differed across strata (figure 1A, log-rank test, p<0.001). Univariable Cox analysis showed an increasing hazard of developing diverticulitis at increasing DICA classification (DICA 2 vs 1, HR 3.63; 2.49‒5.30; and DICA 3 vs 1, HR 7.45; 4.98‒11.1). The hazard of event was double in patients showing DICA equal 3 versus 2 (HR 2.05; 1.42‒2.96).

Kaplan-Meier curves of cumulative incidence of diverticulitis (A), and surgery due to complications (B), from patients categorised into DICA endoscopic classification levels (1–3). DICA, Diverticular Inflammation and Complication Assessment.
Similarly, the 3-year cumulative probability of surgery due to complications significantly increased with higher DICA classification (DICA 1: 0.15%, 0.04%‒0.59%; DICA 2: 3.0%, 1.9%‒4.7%; and DICA 3: 11.0%, 7.5%‒16.0%; figure 1B, log-rank test, p<0.001), as well as the corresponding HRs (DICA 2 vs 1, HR 20.3; 4.70‒88.1; DICA 3 vs 1, HR 77.3; 18.3‒327).
The DICA endoscopic classification showed fair discrimination in predicting the 3-year risk of diverticulitis (Harrell’s c-statistic: 0.705; 0.668‒0.742) and very good discrimination concerning risk of surgery (Harrell’s c-statistic: 0.849; 0.801‒0.896). Performance and predictive accuracy measures, including separate analyses in the development and validation cohorts, are reported in online supplemental table S3.
Development and validation of the CODA score
We sought to identify prognostic factors of diverticulitis in patients with diverticulosis and develop and validate a clinical prognostic score with broad clinical applicability. Three variables were included in the CODA score: DICA classification (1–3), abdominal pain (0–10) as continuous variables and age as dichotomous variable (cut-off at 65 years). Model specifications are reported in table 3. The CODA score ranges from 3 to 31 (only integers), and its scoring system is reported in table 4.
Predictors of acute diverticulitis: results of univariable and multivariable Cox PH analysis (derivation cohort)
Combined Overview on Diverticular Assessment score: scoring system
The Grønnesby and Borgan test showed reasonable model fit in the derivation cohort (score test p=0.2009, likelihood-ratio test p=0.2229) and in the validation cohort (score test p=0.3206, likelihood-ratio test p=0.2731). The calibration slope was 0.86 (95% CI 0.65 to 1.07) in the derivation and 1.27 (95% CI 0.86 to 1.69) in the validation cohort. Both intercepts were not significantly different than zero (pderivation=0.7813; pvalidation=0.8547).
The apparent c-statistic in the development cohort was 0.767 (95% CI 0.727 to 0.806). After adjustment for optimism, the final score showed a c-statistic of 0.757 (0.716‒0.798). The external validation confirmed fair discrimination capacity (c-statistic: 0.708; 0.605‒0.812) very good predictive accuracy (Brier score: 0.052; 0.038‒0.065) and fair overall performance (Nagelkerke’s R2: 0.40; 0.11‒0.70).
Although the CODA score was developed to predict diverticulitis, it showed excellent performance in predicting the 3-year risk of surgery due to complications (secondary outcome). The score showed high discrimination capacity in the development cohort (optimism-corrected c-statistic: 0.829; 95% CI 0.811 to 0.846), online supplemental figure S1, and in the validation cohort (c-statistic: 0.943; 95% CI 0.905 to 0.981), online supplemental figure S2. Apparent and optimism-corrected performance measures in the development and validation cohorts (external validation) for diverticulitis and surgery due to complications are reported in table 5.

Kaplan-Meier curves of cumulative incidence of diverticulitis (A), and surgery due to complications (B), from patients classified into Combined Overview on Diverticular Assessment score categories.
Performance measures of the Combined Overview on Diverticular Assessment score
On the basis of the 3-year risk of diverticulitis (primary endpoint) and surgery (secondary endpoint), the CODA score can be classified into three categories, figure 2. Category A includes patients scoring from 3 to 9 points (3-year risk of diverticulitis ≤4%, 3-year risk of surgery ≤0.7%), category B includes patients scoring from 10 to 16 points (4% <risk of diverticulitis <10%; 0.7% <risk of surgery <2.5%) and category C includes patients scoring over 16 points (risk of diverticulitis >10%; risk of surgery >2.5%). Graphical nomograms showing the risk of primary and secondary study outcomes corresponding to each possible CODA score are plotted in figure 3 (3-year risk) and online supplemental figure S3 (1-year and 2-year risks). The conversion of all possible scores into 1-year, 2-year and 3-year absolute risks of diverticulitis and surgery, respectively, is reported in online supplemental tables S4 and S5.

{kind=link}
{kind=link}
{kind=link}
Nomogram of the CODA score: 3-year predicted risk of diverticulitis (in blue colour), and surgery due to complications (in red colour) corresponding to each possible CODA score. CODA, Combined Overview on Diverticular Assessment; DICA, Diverticular Inflammation and Complication Assessment.
During the model derivation phase, we identified an alternative candidate model including variables comprised in the c-DICA score with the addition of BMI. The alternative model showed a slightly higher apparent discrimination capacity (c-statistic=0.783), but there was evidence of poor fit (Grønnesby and Borgan p=0.0345). In the validation cohort, this model showed a suboptimal discrimination capacity (c-statistic=0.662). Refitting all candidate predictors in the validation cohort revealed that BMI was not associated with the outcome both in the univariable and multivariable analysis. Poor fit in external validation was also observed after using fractional polynomial terms to account for non-linear associations. As suggested by the TRIPOD guideline,1 we selected to not include BMI in the CODA score and sacrifice internal predictive performance to allow for a broader clinical applicability of our score thanks to improved external validity and simplicity.
Discussion
Diverticulosis of the colon is being increasingly diagnosed worldwide.26 Due this large number of examinations, it is quite frequent not only to find diverticulosis but also to find signs of endoscopic inflammation without any clinical suspect of acute diverticulitis.14 15
In 2015, the first endoscopic classification of diverticular disease, called DICA, was presented.17 This classification overcame the flaws of previous definitions describing too vaguely the colon with diverticulosis during colonoscopy, leading to an easy-to-use three-step score.18 19 In this prospective multicentre study, the DICA classification was confirmed to have a significant predictive value in term of acute diverticulitis occurrence/recurrence and risk of surgery during a 3 years follow-up. Since no blinded assessments were undertaken in the present study, a central endoscopical reading will be performed in a further study to assess the reproducibility of each parameters of the DICA classification (diverticulosis extension, number of diverticula in each district, inflammation and complications).
We developed and validated a new clinical score based on DICA: the CODA score. This score had improved characteristics in terms of discrimination capacity and overall performance over DICA. The score was developed in 35 centres in Italy and England and externally validated in 8 centres in other countries belonging to different geographical and healthcare levels, thus ensuring its robustness. The CODA score was built by combining the DICA classification with the level of abdominal pain and age of each patient. This very simple score can be used to predict the individual 3 years risk of acute diverticulitis occurrence/recurrence or surgery occurrence. We know that some clinical parameters have been recognised as risk factor for acute diverticulitis and surgery.16 27–31 However, these factors were just identified as generic risk factors, and their impact on complications during the follow-up was not well-defined. At multivariate analysis, older age and the level of abdominal pain confirmed their role as predictive factor, while the two major risk factors for diverticulitis and surgery previously identified, namely young age and the use of non-steroidal anti-inflammatory drugs, were not. These findings highlight the importance of an international and multicentric patient recruitment who may have different phenotypic characteristics.
This study has several strengths. First, this is the first clinical score ever developed and validated for predicting complications of DD. Indeed, the CODA score is an important step forward in the management of DD and could potentially aid patients and clinicians by enabling selection of the best management strategies based on the predicted risk. Second, this is a, real life, prospective, international cohort study with 3 years of follow-up. The length of the follow-up was determined by the majority of complications, namely acute diverticulitis, occurring or recurring within 2 years after diagnosis of symptomatic uncomplicated diverticular disease (SUDD)32 or acute diverticulitis.16 Third, we enrolled only patients at the first diagnosis of diverticulosis/diverticular disease, naïve to any treatment and early disease, thus avoiding biases that could influence clinical outcome.8 Our results are therefore a real picture of the follow-up of diverticulosis/diverticular disease when diagnosed during colonoscopy. Finally, from a methodological point of view, the candidate predictors considered for model development had no missing values. This allowed an unbiased complete case analysis. Our findings have important consequences for clinical practice. First, by stratifying patients with the CODA scores, physicians may be able to distinguish those patients who need close monitoring during the follow-up from those who will not. The use of the DICA classification, and in particular the use of the CODA score, could revolutionise diverticular disease. The current clinical/radiological classifications do not consider neither the endoscopic appearance nor the patient clinical characteristics. Let us consider the case of an older patient with endoscopic diagnosis of extensive diverticulosis with erosions, and experiencing abdominal pain. Is he/she suffering from SUDD or acute diverticulitis? The results of this study totally change and overcome the current (and probably obsolete) definitions. The patient in the example has a DICA 3 endoscopic score and a C severity of CODA score. This means he/she has a significant risk to have diverticulitis occurrence and surgery occurrence in the next 3 years, and nothing else is needed to define the disease outcome in that patient.
As a consequent point, the potential treatment of these patients has to be reconsidered. At present, we have adequate treatments for SUDD and acute diverticulitis, while no treatment has been found effective in preventing acute diverticulitis recurrence.33 The debate on this last point is still open, and the frustrating results are probably due to a lack of understanding about how to correctly select patients for prophylactic treatment.1 This study opens the door to a new understanding of diverticular disease and its treatment. Since the risk of complications seems associated to disease severity (ie, DICA and CODA), new therapeutic trials should be designed according to these classifications in order to select patients that really need a prophylactic treatment.
In conclusion, this large, prospective, international, real life study, showed that the DICA endoscopic classification is a predictor of outcomes of diverticular disease. The CODA score combines DICA and few clinical parameters, and may reliably predict the occurrence of acute diverticulitis and surgery due to complications, thus providing a new risk stratification tool useful for daily clinical practice.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Ethic Committee of the coordinator centre and of all participating centres.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it published Online First. The author, Enio Chavez de Oliveira, and affiliation 41 and the collaborator group have been added.
Collaborators DICA International Group: Marco Astegiano, Division of Gastroenterology, “Molinette” University Hospital, Torino – Italy. Gianluca Baldassarre, Digestive Endoscopy Unit, ULSS7 Alto Vicentino, Santorso (VI) - Italy. Fabio Baldi†, Digestive Endoscopy Unit, Civil Hospital, Tarquinia (VT) – Italy. † deceased. Edoardo Borsotti, Division of Gastroenterology, “San Donato” Hospital, San Donato Milanese (MI) – Italy. Claudio Cassieri, Division of Internal Medicine and Gastroenterology, “Cristo Re” Hospital, Roma – Italy. Alessia Cazzato, Division of Gastroenterology, “Santa Caterina Novella” Hospital, Galatina (LE) - Italy. Stefania Chiri, Division of Gastroenterology, “Santa Caterina Novella” Hospital, Galatina (LE) - Italy. Antonio Ciccone,Department of Life, Health & Environmental Sciences, Division of Gastroenterology, Hepatology and Nutrition, San Salvatore Hospital, University of L'Aquila, L’Aquila. Debora Compare, Department of Clinical Medicine and Surgery, Division of Gastroenterology and Hepatology, Federico II” University Hospital, Naples - Italy. Alberto Damiani, Service of Digestive Endoscopy, “Villa dei Pini” Home Care, Civitanova Marche (MC) – Italy. Patrizia De Colibus, Division of Gastroenterology, “T. Maresca” Hospital, Torre del Greco (NA) - Italy. Roberto Faggiani, Division of Gastroenterology, “S. Camillo” Hospital, Roma - Italy. Fabio Finocchiaro, Division of Gastroenterology, “Molinette” University Hospital, Torino – Italy. Serafina Fiorella, Division of Gastroenterology, “San Pio da Pietrelcina” Hospital, Vasto (CH) - ItalyA. Francesca Foschia, Territorial Gastroenterology Service, ASL Roma 2, Roma – Italy. Federica Furfaro, IBD Unit, “Humanitas” University Hospital, Rozzano (MI) – Italy. Sara Gallina, Division of Gastroenterology, “Belcolle” Hospital, Viterbo – Italy. Gian Marco Giorgetti, Digestive Endoscopy and Nutritional Unit, “S. Eugenio” Hospital, Roma – Italy. Simona Grad, 2nd Medical Department, “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca – Romania. Giuseppe Grande, Digestive Endoscopy Unit, “Sant’Agostino Estense” Hospital, Baggiovara (MO) – Italy. Antonio Grandolfo, Division of Gastroenterology, “S. Paolo” Hospital, Bari - Italy. Maria Antonia Lai, Division of Gastroenterology – “Monserrato” University Hospital, University of Cagliari, Cagliari - Italy. Piera Giuseppina Lecca, Division of Internal Medicine and Gastroenterology, “Cristo Re” Hospital, Rome - Italy. Daniele Lisi, Digestive Endoscopy and Nutritional Unit, “S. Eugenio” Hospital, Rome - Italy; Territorial Gastroenterology Service, ASL Roma 2, Rome - Italy. Loris Riccardo Lopetuso, Division of Internal Medicine and Gastroenterology, IRCCS “A. Gemelli” Hospital, Fondazione Policlinico Gemelli, Catholic University, Roma – Italy. Antonio Penna, Division of Gastroenterology, “S. Paolo” Hospital, Bari - Italy. Piero Portincasa, Internal Medicine Unit, “A. Murri” Medical Clinic, Policlinico University Hospital, Bari - Italy. Giannenrico Rizzatti, Division of Internal Medicine and Gastroenterology, IRCCS “A. Gemelli” Hospital, Fondazione Policlinico Gemelli, Catholic University, Roma – Italy. Giovanni Luca Rizzo, Division of Gastroenterology, “Perrino” Hospital, Brindisi – Italy. Stefania Scanni, Territorial Gastroenterology Service, ASL Roma 2, Roma – Italy. Luigi Schiffino, Division of Gastroenterology and Surgical Endoscopy, “Grassi” Hospital, Ostia, Roma – Italy. Erasmo Spaziani, Department of Surgery, “Sapienza” University of Rome-Polo Pontino, Terracina (LT) – Italy. Ieva Stundiene, Institute of Clinical Medicine, Vilnius University Hospital, Vilnius - Lithuania. Antonino Tesoriere, Digestive Endoscopy Unit, Civil Hospital, Tarquinia (VT) - Italy. Gabriele Torti, Department of Medicine and Surgery, Gastroenterology and Hepatology Unit, “Santa Maria della Misericordia” University Hospital, University of Perugia, Perugia - Italy. Riccardo Urgesi, Division of Gastroenterology and Digestive Endoscopy “S. Giovanni-Addolorata” Hospital, Roma - Italy. Paolo Usai, Division of Gastroenterology – “Monserrato” University Hospital, University of Cagliari, Cagliari – Italy.
Contributors Guarantor of the Article: AT; Authorship Conception and design: AT; FDM, GB, E.S.; Acquisition and collection of data: AT, GB, WE, LA, MLA, MA, MB, F, B†, GB, MAB, RC, RC, DD, RE, RF, LF, SF, GF, MF, GM, SG, MGG, MAL, FL, GL, DL, GM, GN, LCCO, ECO, AP, SP, AP, AP, SP, PP, TP, GP, MCR, GLR, SR, JR, GS, FS, LS, IS, RV, CZ, AZ, SD, GB, EB, CC, AC, SC, AC, DC, AD, PDC, FF, FF, FF, SG, GG, AG, PGL, LRL, FP, GR, SS, AT, GT, RU,PU; Analysis and interpretation of data: AT, WE, MP, DP, SB, SD; Final approval of the version to be published: AT, GB, WE, LA, MLA, MA, MB, F, B†, GB, MAB, RC, RC, DD, RE, RF, LF, SF, GF, MF, GM, SG, MGG, MAL, FL, GL, DL, GM, GN, LCCO, ECO, AP, SP, AP, AP, SP, PP, TP, GP, MCR, GLR, SR, JR, GS, FS, LS, IS, RV, CZ, AZ, SD, GB, EB, CC, AC, SC, AC, DC, AD, PDC, FF, FF, FF, SG, GG, AG, PGL, LRL, FP, GR, SS, AT, GT, RU, PU.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SD served as speaker, consultant and/or advisory board member for AbbVie, Allergan, Alfa Wassermann, Biogen, Boehringer Ingelheim, Celgene, Celltrion, Ferring, Gilead, Hospira, Johnson and Johnson, Merck, MSD, Mundipharma, Pfizer, Sandoz, Takeda, Tigenix, UCB Pharma, Vifor. GM served as speaker and/or advisory board fees for AlfaSigma, Arena, Janssen, Gilead, Roche. GN received funding for target projects from Apharm and Sofar. APserved as lecturer for AlfaSigma and Polpharma. JR served as lecturer for AlfaSigma, Takeda, Ipsen and Servier. FS served as lecturer for Sanofi.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Commentary