Article Text

Abstract
Objective Metabolic dysfunction-associated steatotic liver disease (MASLD) is a growing global health concern, with increasing mortality rates driven by the obesity pandemic. Weight loss has been shown to improve MASLD outcomes, yet the effectiveness of eHealth interventions in MASLD management remains uncertain. We aimed to evaluate the effectiveness of eHealth interventions compared with standard care in improving health outcomes among patients with MASLD.
Design A systematic review and meta-analysis were conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Data sources Relevant studies were retrieved from PubMed, Cochrane Central and Embase databases from inception to 26 April 2024.
Eligibility criteria Only double-arm clinical trials involving human participants diagnosed with MASLD were included. Eligible studies were limited to those published in English.
Data extraction and synthesis eHealth interventions—including internet-based platforms, smartwatches, telephone follow-ups and mobile applications for dietary and exercise modifications—were compared against traditional intervention methods. The primary outcomes assessed were changes in body weight, abdominal/waist circumference, aspartate aminotransferase (AST) and alanine transaminase (ALT). Secondary outcomes were changes in body mass index (BMI), diastolic blood pressure, systolic blood pressure, MASLD fibrosis score, high-density lipoprotein, gamma-glutamyl transferase and triglycerides.
Results 11 studies met the inclusion criteria, of which 10 provided relevant outcomes and were included. The mean age of participants across the studies ranged from 39.3 to 57.9 years, with intervention durations spanning 3 to 24 months. Our results indicate significant improvements with eHealth interventions compared with control comparators, including reductions in AST (standardised mean difference (SMD): −0.35 (95% CI –0.61, –0.10); p<0.05), ALT (SMD: −0.38 (95% CI –0.65, –0.11); p<0.05), weight loss (SMD: −0.38 (95% CI –0.60, –0.17); p<0.05) and BMI (SMD: −0.37 (95% CI –0.54, –0.21); p<0.05).
Conclusions The utilisation of eHealth interventions showed significant improvements in outcomes related to AST, ALT, abdominal circumference, weight loss and BMI. However, future studies with larger sample sizes and longer follow-ups are warranted to assess the sustainability of these outcomes.
- OBESITY
- Non-alcoholic Fatty Liver Disease
- Mobile Applications
- META-ANALYSIS
- NONALCOHOLIC STEATOHEPATITIS
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- OBESITY
- Non-alcoholic Fatty Liver Disease
- Mobile Applications
- META-ANALYSIS
- NONALCOHOLIC STEATOHEPATITIS
WHAT IS ALREADY KNOWN ON THIS TOPIC
eHealth interventions are effective at body mass index (BMI) reduction and cause significant decreases in liver enzyme levels (aspartate aminotransferase and alanine transaminase) in patients with metabolic dysfunction-associated steatotic liver disease (MASLD).
WHAT THIS STUDY ADDS
Our meta-analysis establishes that eHealth interventions significantly enhance weight loss and improve BMI and liver enzyme levels in patients with MASLD. Interventions with daily reminders were significantly more effective in promoting weight loss than those with less frequent contact.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
eHealth interventions, in particular those with daily reminders, can enhance weight loss and reduce liver enzymes in patients with MASLD. Future studies with larger sample sizes and longer follow-ups are warranted to assess the sustainability of these outcomes.
Introduction
Metabolic-associated steatotic liver disease (MASLD) is a prevalent metabolic disorder characterised by hepatic lipid accumulation, commonly associated with obesity and diabetes.1 Despite its often asymptomatic nature, MASLD can progress to metabolic-associated steatohepatitis (MASH), a more severe form of the disease, ultimately leading to liver fibrosis, cirrhosis, hepatocellular carcinoma and the potential necessity for liver transplantation.2 3 MASLD is a serious health hazard as the mortality rates continue to rise along with the obesity pandemic.4 5 Given its widespread prevalence, affecting nearly 33% of the global population, MASLD represents a significant burden on healthcare systems, necessitating effective management strategies.6
Weight loss is pivotal in treating MASLD, with greater weight loss correlating with more significant histological improvements in liver health.7 8 Despite advancements in pharmacological treatments, non-pharmacological approaches, such as dietary modifications and weight loss regimens, remain the cornerstone of MASLD management.9–12 However, a significant challenge lies in the high prevalence of physical inactivity among MASLD patients, with over 80% reported as being sedentary.13 This sedentary lifestyle contributes to disease progression in many cases. Although structured lifestyle programmes, focusing on nutrition and exercise, have demonstrated success in promoting weight loss, they are not without limitations.14 Traditional in-person programmes face obstacles such as cost, geographical accessibility and time constraints, often resulting in inconsistent patient adherence. In recent years, the integration of digital interventions such as mobile phone apps and web-based exercise programmes has been deemed to be useful for weight loss.15–17 By eliminating the need for physical attendance, these interventions mitigate barriers associated with travel and decrease time commitments, thus enhancing patient engagement. Additionally, digital platforms provide opportunities for real-time feedback, allowing for personalised and immediate guidance.
Despite the promising potential of eHealth interventions for MASLD management, existing clinical trials comparing them to standard care remain limited and often constrained by small sample sizes. Prior meta-analyses have also been constrained by narrow outcome measures and heterogeneous study designs, making it difficult to draw robust conclusions.18 19 To address these limitations, we conducted a systematic review and meta-analysis to comprehensively assess the efficacy of eHealth interventions compared with standard care in improving clinical outcomes in patients with MASLD.
Methods
This systematic review and meta-analysis adhered to the methodological standards outlined in the Cochrane Handbook for Systematic Reviews of Interventions. The reporting of findings followed the guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).20–22
Eligibility criteria and outcomes
Eligible studies were restricted to peer-reviewed articles published in English and involving human participants. Inclusion criteria required the following: (1) Only participants with MASLD as the primary diagnosis; (2) only double-arm studies be considered and (3) interventions using eHealth platforms such as internet-based approaches, smartwatches, telephone follow-ups or mobile phone applications for diet or exercise modifications were compared against traditional intervention methods in a control group. Exclusion criteria encompassed the following: (1) studies lacking MASLD as the primary diagnosis; (2) single-arm designs; (3) non-human studies and (4) publications categorised as case reports, reviews or observational studies.
The primary outcomes were changes in body weight, abdominal/waist circumference, aspartate aminotransferase (AST) and alanine transaminase (ALT). The secondary outcomes were changes in body mass index (BMI), diastolic blood pressure (DBP), systolic blood pressure (SBP), MASLD fibrosis score, high-density lipoprotein (HDL), gamma-glutamyl transferase (GGT) and triglycerides. The components of lifestyle modification interventions for MASLD are categorised into seven key areas: initial assessments, education, dietary counselling, physical activity monitoring, feedback, interactive communication and motivation strategies. Comprehensive lifestyle interventions (CLIs) are defined as interventions that incorporate all seven components. In contrast, partial lifestyle interventions (PLIs) are interventions that lack one or more of these essential components.
Data sources and search
To identify eligible clinical trials, an electronic search of PubMed, Scopus and the Cochrane Central Register of Controlled Trials was conducted from inception to 26 April 2024. The detailed search strategy is provided in online supplemental table 1. Articles identified through the systematic search were then imported into rayyan.ai, where duplicates were removed.23 Subsequently, a two-stage screening process was employed: (1) initial screening based on title and abstract, followed by (2) full-text screening for inclusion according to the predefined eligibility criteria. Both stages of screening were performed independently by two reviewers (MS and SZA), with any discrepancies resolved through consultation with a third reviewer (MUS) and subsequent discussion.
Supplemental material
Data extraction and quality assessment
Two independent reviewers, MS and SZA, conducted data extraction and quality assessment from the included studies. Any disparities in data extraction or quality assessment were addressed through thorough discussion between the reviewers. The extracted data encompassed baseline characteristics, trial demographics and outcome measures, all of which were documented in an Excel spreadsheet. Quality assessment of the included studies was conducted in accordance with the Cochrane risk of bias tool.24 To ensure accuracy and reliability, all authors collectively reviewed the extracted data.
Statistical analysis
In our analysis, we used the mean change from baseline to determine effect sizes. In instances where only baseline and endpoint measurements were accessible, we calculated the mean change (and its SD) as follows: ΔMean=mean endpoint−mean baseline and ΔSD= where r represents the correlation coefficient. To ensure minimal estimation bias in determining ΔSD, we adopted a conservative correlation coefficient value of r=0.7.25 When the original study only supplied the total follow-up sample size without specifying counts for control and intervention groups, we contacted the authors for additional information. If they were not able to provide the data, we split the total number of participants in a 1:1 ratio in intervention and control groups. In our study, effect sizes were aggregated using a random-effects model to compute standardised mean differences (SMDs) alongside their corresponding 95% CIs. Visual representations of the analysis were constructed through forest plots, while funnel plots were employed to scrutinise potential publication bias. To gauge heterogeneity across trials, we used τ² and Higgins I² statistic, with an I² value of ≤50% deemed acceptable. Statistical significance was determined by a p<0.05. Review Manager (V.5.4, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020) served as the primary tool for conducting all statistical analyses.
where r represents the correlation coefficient. To ensure minimal estimation bias in determining ΔSD, we adopted a conservative correlation coefficient value of r=0.7.25 When the original study only supplied the total follow-up sample size without specifying counts for control and intervention groups, we contacted the authors for additional information. If they were not able to provide the data, we split the total number of participants in a 1:1 ratio in intervention and control groups. In our study, effect sizes were aggregated using a random-effects model to compute standardised mean differences (SMDs) alongside their corresponding 95% CIs. Visual representations of the analysis were constructed through forest plots, while funnel plots were employed to scrutinise potential publication bias. To gauge heterogeneity across trials, we used τ² and Higgins I² statistic, with an I² value of ≤50% deemed acceptable. Statistical significance was determined by a p<0.05. Review Manager (V.5.4, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020) served as the primary tool for conducting all statistical analyses.
Results
Search results
Our search string identified 295 studies from relevant databases. After title and abstract screening, we were left with 16 studies that covered the use of eHealth interventions in treating health outcomes among patients with MASLD. After full-text screening, five single-arm studies were excluded. A total of 11 clinical trials17 26–35 met the inclusion criteria, and 10 were included in the meta-analysis as one of the studies did not report any relevant outcomes.35 This process is summarised in the PRISMA flow chart (online supplemental figure1).
Characteristics of included studies
The characteristics of the included studies are summarised in table 1. The studies span from 2016 to 2024 and cover various geographical regions, including China, Iran, Italy, Singapore, Portugal, Korea and the USA. The review encompassed a total of 1521 participants, with individual study sample sizes ranging from 24 to 716 participants. The participants’ average age varied from 39.3 to 57.9 years, with a majority being male in most studies. Dong et al exclusively recruited male participants.27 The duration of interventions spanned from 3 to 24 months. The interventions primarily focused on combining dietary and physical activity counselling with different modes of delivery, such as telephone visits, text messages, web-based programmes, and mobile phone applications. Standard care was used as the control in all studies. The BMI of participants ranged from 25.5 to 36.0 kg/m², with body weight spanning from 75.9 kg to 104.3 kg where reported.
Characteristics of included studies
Intervention delivery and frequency
The components of lifestyle modification interventions for MASLD are categorised into seven key areas: initial assessments, education, dietary counselling, physical activity monitoring, feedback, interactive communication and motivation strategies (table 2). Initial assessments of participants’ physical conditions were consistently conducted across all studies.17 26–35 The majority of studies provided education related to disease management or healthy behaviours,17 26 28–35 dietary counselling,17 26 27 29–35 and motivation,17 26–34 with only one study omitting each of these components. Interactive communication17 26 29–35 and feedback mechanisms26–34 were also prominently featured in nine studies. Monitoring of participants’ physical activity was less common, implemented in approximately half of the studies.26 29–31 33 34 Among the technological modalities used, mobile phone applications were the most common,29–31 33 34 followed by telephone interventions.26 27 35 Other technologies included video or phone,32 short message service (SMS) text messaging,28 web platforms17 and mobile-technology approaches.34 The frequency of these interventions varied widely among the studies, ranging from daily interactions28–31 to a few times a week,26 35 once a week,17 34 once a month33 and once every 3 months27 ,32 with daily interventions being the most prevalent.
Components of eHealth strategies
Risk of bias
The risk of bias for the studies included is summarised in online supplemental figure 2 and online supplemental figure 3. Most of the studies were assessed as having a low risk of bias across primary measures, supported by strong randomisation, allocation concealment and outcome assessment procedures. Performance bias was generally low, although two specific studies displayed a high risk due to inadequate blinding.31 32 Attrition bias and reporting bias were predominantly minimal, with one study having attrition28 bias and one study having reporting bias.17 The assessment of other biases showed mixed results, with six of the eleven studies classified as having an unclear risk.27–30 34 35
Results of the meta-analyses
Forest plots displaying the effects of eHealth interventions on outcomes based on MASLD are presented in figures 1–3.

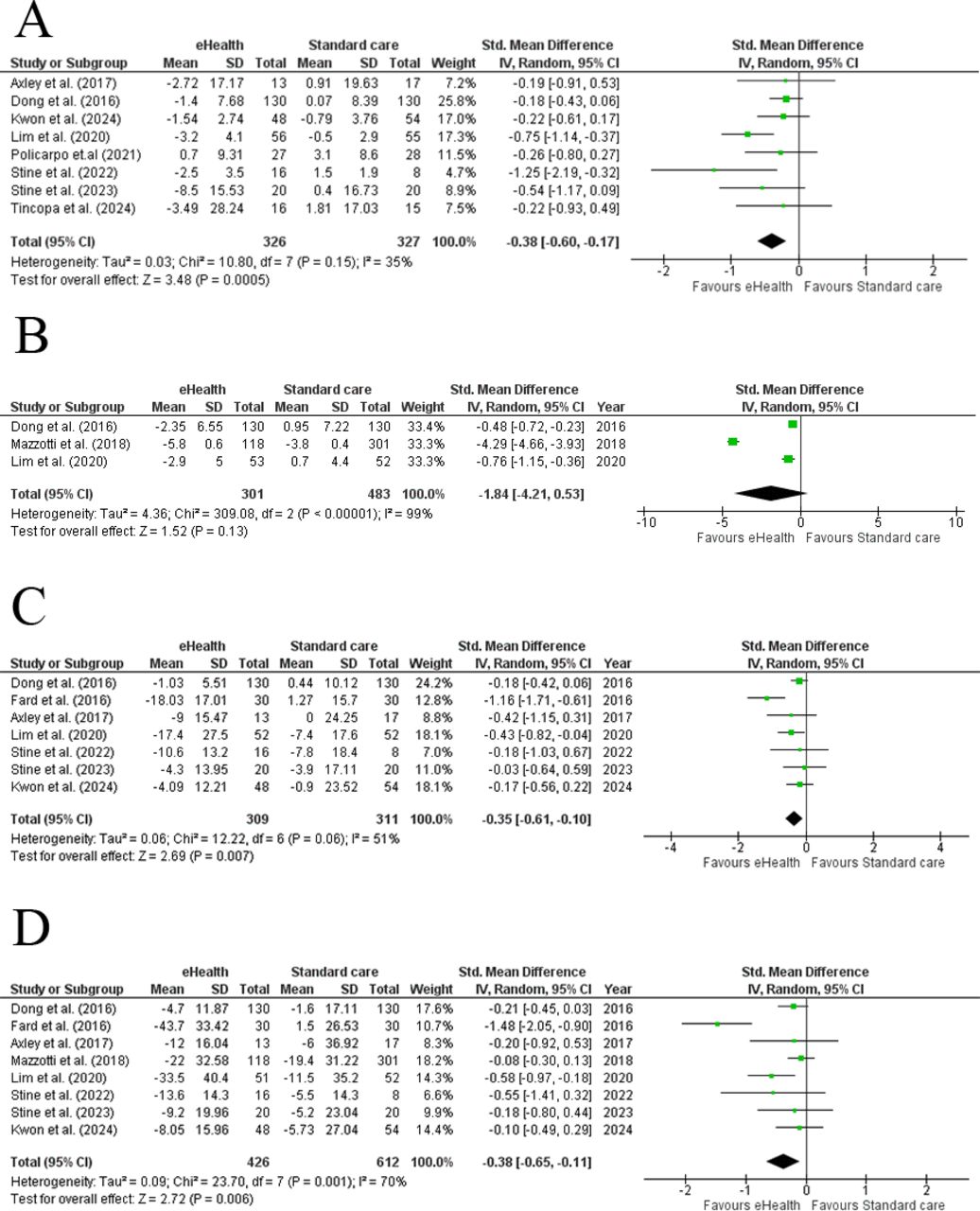
Forest plot assessing the effect of eHealth interventions versus standard care on (A) weight loss, (B) abdominal/waist circumference, (C) aspartate aminotransferase levels and (D) alanine aminotransferase levels in patients with MASLD. MASLD, metabolic dysfunction-associated steatotic liver disease.

Forest plot assessing the effect of eHealth interventions versus standard care on (A) body mass index, (B) diastolic blood pressure, (C) systolic blood pressure, (D) MASLD fibrosis score (E) high-density lipoprotein levels, (F) gamma-glutamyl transferase levels, and (G) triglyceride levels in patients with MASLD. MASLD, metabolic dysfunction-associated steatotic liver disease.

{kind=link}
{kind=link}
{kind=link}
Forest plot for subgroup analyses of eHealth interventions on weight loss, including (A) comprehensive lifestyle interventions (CLI) versus partial lifestyle interventions (PLI), (B) eHealth interventions at 3-month vs 6-month follow-up, (C) frequency of contact (daily vs monthly) and (D) mobile phone applications versus other eHealth interventions in patients with MASLD. MASLD, metabolic dysfunction-associated steatotic liver disease.
Primary outcomes
Weight
Eight studies reported the effect of eHealth intervention on weight. Meta-analysis showed that the effect of eHealth intervention caused a significant decrease in weight of patients with MASLD (SMD: −0.38 (95% CI –0.60, –0.17); p<0.05; I2=35%; τ²=0.03, figure 1A).
Abdominal/waist circumference
Three studies reported data for abdominal/waist circumference. Meta-analysis of these studies showed that eHealth interventions did not significantly decrease the abdominal/waist circumferences of patients with MASLD (SMD: −1.84 (95% CI –4.21, –0.53); p=0.13; I2=99%; τ²=4.36, figure 1B).
Aspartate aminotransferase
Seven studies reported data for AST. Meta-analysis of these studies showed that eHealth interventions significantly reduced the AST levels of patients with MASLD (SMD: −0.35 (95% CI −0.61, –0.10); p<0.05; I2=51%; τ²=0.06, figure 1C).
Alanine transaminase
Eight studies reported data for ALT. Meta-analysis of these studies showed that eHealth interventions significantly reduced the ALT levels of patients with MASLD (SMD: −0.38 (95% CI −0.65, –0.11); p<0.05; I2=70%; τ²=0.09, figure 1D).
Secondary outcomes
Body mass index
Six studies reported data for BMI. Meta-analysis of these studies showed that eHealth interventions significantly decreased the BMI of patients with MASLD (SMD: −0.37 (95% CI −0.54, –0.21); p<0.05; I2=1%; τ²=0.00, figure 2A).
Diastolic blood pressure
Two studies reported DBP. Meta-analysis of these studies showed that eHealth interventions did not significantly reduce DBP in patients with MASLD (SMD: −0.49 (95% CI −1.02, 0.04); p=0.07; I2=75%; τ²=3.96, figure 2B).
Systolic blood pressure
Two studies reported SBP. Meta-analysis of these studies showed that eHealth interventions did not significantly reduce SBP in patients with MASLD (SMD: −0.43 (95% CI −0.91, 0.05); p=0.08; I2=70%; τ²=0.09, figure 2C).
MASLD fibrosis score
The MASLD fibrosis score was reported in two studies. Meta-analysis of these studies showed that eHealth intervention did not significantly affect the MASLD fibrosis score within patients with MASLD (SMD: −0.46 (95% CI −1.84, 0.92); p=0.51; I2=93%; τ²=0.93, figure 2D).
High-density lipoprotein
Three studies reported HDL levels. Meta-analysis of these studies showed that eHealth interventions had no significant impact on the HDL levels in patients with MASLD (SMD: −1.38 (95% CI −4.32, 1.56); p=0.36; I2=96%; τ²=4.52, figure 2E).
Gamma-glutamyl transferase
Two studies reported GGT levels. Meta-analysis of these studies showed that eHealth interventions did not significantly reduce the levels of GGT in patients with MASLD (SMD: −1.04 (95% CI −2.54, 0.45); p=0.17; I2=98%; τ²=1.14, figure 2F).
Triglycerides
Four studies reported triglyceride levels. Meta-analysis of these studies showed that eHealth interventions did not have a significant effect on the triglyceride levels of patients with MASLD (SMD: −0.14 (95% CI −0.44, 0.16); p=0.37; I2=59%; τ²=0.051, figure 2G).
Subgroup analysis of CLI versus PLI for weight loss
CLI was defined as studies that used eHealth to provide all the following components: education, feedback, counselling for diet, physical activity monitoring, interactive communication and motivation. PLI was defined as interventions missing at least one of these components. We conducted this subgroup analysis to assess the effectiveness of CLI versus PLI for weight loss. CLI resulted in a significantly greater reduction in weight (SMD: −0.53 (95% CI −0.85, –0.21); p<0.05; I2=40%; τ²=0.05, figure 3A) compared with PLI (SMD: −0.20 (95% CI −0.41, 0.02); p=0.07; I2=0%; τ²=0.00, figure 3A). No statistically significant difference was observed between the subgroups (p=0.09).
Subgroup analysis of eHealth interventions at 3 months and 6 months follow-up for weight loss
A subgroup analysis was conducted to assess the effectiveness of eHealth interventions on weight loss at 3 and 6 months of follow-up. Significant reductions in body weight were observed at both 3 months (SMD: −0.57 (95% CI −1.07, –0.08); p<0.05; I²=39%; τ²=0.07 figure 3B) and 6 months (SMD: −0.40 (95% CI −0.72, –0.09); p<0.05; I²=34%; 0.03, figure 3B), with the effect size being more pronounced at the 3-month follow-up. However, no statistically significant difference was found between the subgroups (p=0.57).
Subgroup analysis of frequency of contact for weight loss
A subgroup analysis was conducted to evaluate the effectiveness of different contact frequencies for weight loss. Significant reductions in body weight were observed with daily (SMD: −0.66 (95% CI −0.99, –0.34); p<0.05; I2=15%; τ²=0.02, figure 3C) and monthly contacts (SMD: −0.20 (95% CI −0.40, –0.01); p<0.05; I2=0%; τ²=0.00, figure 3C), with a greater magnitude attributed to daily contacts. A statistically significant difference was observed between the subgroups (p=0.02).
Subgroup analysis of mobile phone applications versus other eHealth interventions for weight loss
A subgroup analysis was conducted to evaluate the effectiveness of different types of eHealth interventions for weight loss. Mobile phone applications resulted in a significant reduction in body weight (SMD: −0.59 (95% CI −0.96, –0.22); p<0.05; I2=49%; τ²=0.07, figure 3D), compared with other eHealth interventions such as text messages, web-based programmes, smartwatches and telephone follow-ups (SMD: −0.20 (95% CI −0.40, 0.00); p=0.06; I2=0%; τ²=0.00, figure 3D). No statistically significant difference was observed between the subgroups (p=0.07).
Discussion
Our meta-analysis establishes that eHealth interventions significantly enhance weight loss, improve BMI and liver enzyme levels in patients with MASLD. Interventions with daily reminders were significantly more effective in promoting weight loss than those with less frequent contact. The clinical trials we analysed, conducted between 2016 and 2024, underscore the nascent stage of eHealth adoption in treating MASLD. Our results support the use of eHealth interventions in treating patients with MASLD to improve clinical outcomes.
Although existing meta-analyses have suggested the superiority of eHealth interventions over standard care, these studies have notable limitations that may have affected their conclusions.18 19 For instance, Kwon et al demonstrated only a borderline significant result for weight loss, with a limited range of outcomes reported, potentially restricting the scope of their findings. Similarly, the meta-analysis by Albhaisi et al combined single-arm and double-arm studies, a methodological choice that may have introduced confounding variables and statistical noise, thereby compromising the reliability of their results. Our meta-analysis addressed these limitations by including high-quality double-arm clinical trials, a larger sample size and a greater number of reported outcomes to fully assess the effectiveness of eHealth on patient outcomes.
Current treatment guidelines advocate for weight loss as the primary intervention for MASLD, noting that reduction in both subcutaneous and visceral fat can improve liver health markers like AST and ALT.36–38 Consistent with previous research, our results demonstrate greater benefits of eHealth interventions over traditional weight loss methods, owing to their ease and accessibility.39 This is crucial because patients often hesitate to adhere to strict in-person treatment routines due to costs, geographical barriers and time constraints. These factors particularly affect MASLD patients, who may be reluctant to follow a strict weight loss regimen since MASLD typically remains asymptomatic until severe stages, such as MASH cirrhosis.40
eHealth interventions, including mobile applications, telephonic follow-ups, web-based programmes and smartwatches, demonstrate varying levels of effectiveness in managing MASLD, with all showing superiority over standard care in promoting weight loss. While subgroup analysis did not show mobile phone apps to be significantly better than other eHealth interventions, the difference was borderline non-significant and could become significant with the inclusion of more studies. This is likely due to the multifunctionality and user-friendly features of mobile phones, such as AI-driven caloric tracking via uploaded food images.33 This technology significantly reduces the burden of manual entry, enhancing the accuracy and consistency of dietary monitoring. By simplifying the tracking process, these apps improve patient adherence to dietary goals, ultimately leading to more successful weight management and better clinical outcomes.
The variation in contact frequency—from daily to several months—reveals a significant result indicating that daily reminders are more effective in maintaining patient motivation, adherence, and consequently, weight loss. However, it is to be noted that the optimal frequency of contact may vary among individuals. Excessive reminders, especially multiple times a day, could lead to patient fatigue or irritation, diminishing the intervention’s effectiveness. This balance underscores the need for personalised intervention schedules that optimise engagement without overwhelming patients. Consequently, further research is essential to determine the ideal frequency and intensity of interventions that can most effectively engage patients and promote long-term adherence to lifestyle changes. Exploring how patient characteristics influence responsiveness to different intervention frequencies could lead to more tailored and effective treatment strategies for MASLD.
Most of our secondary outcomes showed non-significant results and high heterogeneity, largely due to the frequent omission of important measures in these trials. For example, despite the critical role of the MASLD fibrosis score in predicting liver cancer, cirrhosis and liver failure, its frequent omission has led to significant variability in our results.41 Future studies should consistently report a broader set of outcomes to better assess the improvements that eHealth interventions can achieve.
Decentralised clinical trials (DCTs) present a valuable opportunity to enhance both the effectiveness and accessibility of eHealth interventions for MASLD. The flexible and remote nature of DCTs enables comprehensive and consistent data collection across diverse populations and settings.42 This allows for continuous monitoring and the inclusion of a wider array of health indicators often overlooked in traditional trials. Data reporting becomes more accurate, such as adverse events being recorded in real-time, rather than retrospectively. This lowers the risk of inaccurate data collection due to factors such as patient forgetfulness, which often results in non-reporting of data. It also provides a more reliable time frame for the onset of such adverse events.43
The FDA’s recent approval of Rezdiffra as the first drug for MASH introduces a significant advancement in the treatment landscape.44 While promising, Rezdiffra is still new and should be considered a complementary therapy to conventional lifestyle modifications, highlighting the continued importance of weight loss in improving MASLD prognosis. Future trials that use a combination therapy of eHealth-based weight loss interventions with Rezdiffra, compared with traditional weight loss methods, could provide new insights and potentially reduce the global burden of MASLD.
While eHealth interventions offer significant potential in managing MASLD, their implementation comes with challenges. First, digital health access is not universal, and disparities in internet availability, socioeconomic status, and digital literacy may limit its effectiveness, particularly among older patients or those in low-resource settings. Second, reliance on digital platforms could impact patient–physician trust, as some patients may feel less connected to their healthcare provider in a remote setting. Future studies should explore strategies to improve accessibility, provide digital literacy training and develop hybrid care models that combine digital and in-person interactions to optimise patient engagement and outcomes.45
Strengths and limitations
Our study presents many strengths. It assesses the effectiveness of eHealth interventions against standard care comprehensively, incorporating a larger sample size and more clinical trials than the previous meta-analyses.18 19 Our analysis is unique as it not only explores a broader range of outcomes but also provides subgroup analyses to determine the impact of different types of digital interventions, contact frequency and CLI versus PLIs on weight loss.
Our meta-analysis has several limitations. First, we observed high heterogeneity in many outcomes, particularly in secondary outcomes, due to the limited number of available studies. Notably, results for outcomes such as DBP, SBP, MASLD fibrosis score, and GGT should be interpreted with caution, as they were reported in only two studies. Given this small sample size, these findings may not accurately reflect the true effects of eHealth interventions in MASLD patients. Future studies with larger sample sizes and standardised outcome reporting are needed to strengthen the evidence base. Second, the short follow-up duration in most studies restricts our understanding of the long-term benefits of eHealth interventions. Third, the potential for recall bias exists, where participants might not accurately recall their diet and exercise behaviours, leading to misreporting. Fourth, social desirability bias could influence participants to report behaviours they believe are expected or socially acceptable rather than their actual behaviours, potentially resulting in the overreporting of positive actions and under-reporting of negative ones. Lastly, funnel plots were not generated for any outcomes, as the recommended minimum threshold for conducting such analyses is at least 10 studies per outcome. Given that none of the outcomes in our meta-analysis met this criterion, the generation of funnel plots was not feasible.
Conclusions
Our meta-analysis confirms that eHealth interventions significantly improve various health markers for MASLD patients, including reductions in weight, AST, ALT and BMI. These results highlight the potential for healthcare professionals to further enhance the effectiveness of eHealth technologies by understanding their nuances, ultimately aiding MASLD patients in improving their self-management skills.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors YZ acted as guarantor; YZ: conceptualisation, writing–review and editing, supervision; US: methodology, writing–original draft, formal analysis, writing–review and editing, project administration; MS: writing–original draft, writing–review and editing, data curation, visualisation; SZA: data curation, writing–original draft, writing–review and editing; OS: supervision, data curation; JZ: supervision; SL: supervision; AS: supervision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.