Article Text

Abstract
Objective Gastric adenocarcinoma (GAC) is the 17th most common cancer in the UK with a 5-year survival rate of 22%. GastroPanel (Biohit Oyj; Helsinki, Finland) is an ELISA kit that measures pepsinogen I (PGI); pepsinogen II (PGII); gastrin-17 (G-17); and Helicobacter pylori IgG antibodies (Hp IgG). PGI and the PGI/PGII ratio correlate inversely with the severity of chronic atrophic gastritis (AG). The aim of this study was to assess GastroPanel performance in the identification of moderate to severe AG in dyspepsia.
Methods In this UK, single-centre, prospective diagnostic accuracy study, 324 patients [56.8% (n=184) female; median age 57 years (range 39–92 years)] were recruited for gastroscopy with biopsy and histology according to the updated Sydney System (USS). Blood (plasma) samples were collected for GastroPanel analysis. Paired samples were obtained from 268 patients [56.3% (n=151) female; median age=57 (range 39–92 years)]. GastroPanel results were interpreted using the GastroSoft app (Biohit).
Results Overall agreement between GastroPanel and the USS classification was 90% (95% CI=86.7 to 93.8%), with a weighted kappa (κw) of 0.828 (95% CI=0.781 to 0.865). In receiver operating characteristics (ROC) curve analysis, using moderate/severe atrophic gastritis of the corpus (AGC2+) as the endpoint, AUC=0.840 (95% CI 0.630 to 1.000) and 0.960 (95% CI 0.907 to 1.000) for PGI and the PGI/PGII ratio, respectively.
Conclusion GastroPanel is a reliable dyspepsia triage test distinguishing patients who can be safely treated conservatively from those with moderate to severe corpus atrophic gastritis at high risk of developing GAC.
- GASTRIC CARCINOMA
- GASTRIC DISEASES
- HELICOBACTER PYLORI - GASTRITIS
- DYSPEPSIA
- FUNCTIONAL DYSPEPSIA
Data availability statement
Data are available upon reasonable request. Data underlying the study will be shared with other researchers on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Gastric cancer in the UK is diagnosed at a late stage, only 22% of patients survive 5 years, and 48% 1 year. Studies have shown that some patients with atrophic gastritis (AG) at an increased risk of developing gastric adenocarcinoma (GAC) are Hp negative with low PGI. The GastroPanel test is a diagnostic kit for the biomarkers PGI, PGII, G-17 and Hp IgG. Low levels of PGI and decreased PGI/PGII ratio (with high G-17), independent of Hp IgG status (Hp+/-), indicate severe extensive corpus atrophic gastritis associated with a high risk of progression to GAC.
WHAT THIS STUDY ADDS
GastroPanel cut-off values might be affected by laboratory methodologies and population settings, and therefore, we carried out a clinical validation study in the UK. We found an all grade AG prevalence of 11.9% in patients with dyspeptic symptoms. The new generation GastroPanel ELISA was confirmed to be a precise test for the non-invasive diagnosis of moderate to severe AG of the corpus, in the UK population.
HOW THIS STUDY MIGHT AFFECT RESEARCH, CLINICAL PRACTICE OR POLICY
The new generation GastroPanel can be used for triaging patients by differentiating cases with functional dyspepsia from those with moderate to severe extensive AG who need image-enhanced endoscopy and updated Sydney System biopsies as per the 2019 British Society of Gastroenterology guidelines. The use of GastroPanel can improve the current dyspepsia pathway. Its use in clinical practice will produce a substantial financial and environmental impact by avoiding unnecessary upper GI endoscopy procedures and help keep the focus on patients with high-risk precancerous lesions.
Introduction
Gastric cancer (GC) is the sixth most common cancer worldwide, with an age-standardised incidence rate of 11.1. In the UK, it is the 17th most common cancer with 6568 cases diagnosed each year. It is estimated that 54% of cases are preventable; yet, its prognosis remains poor, with 1-year and 5-year survival rates being just 48% and 22%, respectively.1–5 The intestinal phenotype of GC—gastric adenocarcinoma (GAC) is the most common6 7 accounting for 90%–95% of all cases.
Atrophic gastritis (AG) is the most prevalent environmental precancerous condition for GAC with a pooled risk ratio of 2.91 with 95% CI of 2.58 to 3.277. Helicobacter pylori (Hp) and autoimmune AG are the two most important risk factors in the pathogenesis of GAC.8 The risk of GAC increases with the severity of AG in a linear fashion, reaching 90-fold in those with moderate to severe AG.9 10 Studies exploring the risk of progression from chronic AG to GAC report a range of between 0.1% and 10%, which is roughly comparable with other premalignant conditions of the gastrointestinal tract, such as Barrett’s oesophagus and colonic adenomatous polyps.11 12
It is agreed among experts that there is a need for an effective triage tool to select or exclude dyspeptic patients for gastroscopy at the point of referral.
Plasma PGI and the PGI/PGII ratio alone or in combination with G-17 and Hp serology can identify individuals with moderate to severe AG.13 Plasma PGI and PGII reflect the function and integrity of the corpus mucosa and entire stomach mucosa respectively.14–16 Plasma G-17 reflects antrum G-cell mass and is therefore a marker of antrum atrophic gastritis; however, because of its physiological role in acid regulation, G-17 is also a marker of acid output.
Functionally, mucosal atrophy is characterised by the impairment of acid production, lower PGI/PGII ratio and increased gastrin serological concentration. The finding of negative serum anti-Hp IgG antibody and positive PG measurements in particular, suggests moderate to severe AG.17 18
The aim of the present study was to assess GastroPanel performance in the identification of moderate to severe AG in patients with dyspepsia. As with any in vitro diagnostic test, values might be affected by laboratory methodologies and population settings, and therefore, we carried out this clinical validation study in the UK.
Methods
This single-centre, prospective diagnostic accuracy study was conducted at the Gastroenterology Department of Homerton University Hospital, London, UK. The STARD checklist was used to inform the study reporting (supplemental material, research checklist). Study recruitment was guided by an expected 8.2% prevalence of atrophic gastritis in dyspepsia19 and a point estimate of 80% sensitivity for this lesion. We planned to recruit 324 cases to achieve margins of sampling error of approximately 8 percentage points for sensitivity. The sample allowed 90% power to detect differences in sensitivity between gastric biopsies and GastroPanel of 18 percentage points or more. Consecutive patients with dyspepsia but no alarm symptoms, referred for gastroscopy, following UK dyspepsia pathway guidelines19 were recruited between February 2017 and January 2019.
All eligible patients (over 18 years old) were identified and asked to sign a written consent form before being interviewed using dyspepsia diagnosis criteria.20 Patient exclusion criteria were employed as per previous studies.13 21 Patients whose treatment required surgery, or immediate endoscopy (2-week wait pathway) for alarm symptoms were excluded (see patient flow chart online supplemental figure 1s).
Supplemental material
Suitable patients were invited to take part in the study. The study protocol followed the Declaration of Helsinki and was approved by the Ethics Committee of the NRES Committee East of England-Cambridge South (15/EE/0205). The study was registered on ClinicalTrials.gov NCT 02114411.
Patient demographic data was collected, including age, sex and clinical history, Hp infection status, medications and symptoms, using a standardised functional dyspepsia questionnaire (online supplemental table 1s).
Patients were prepared for gastroscopy following a standard protocol. They were advised not to eat, drink or smoke for at least 4 hours before blood sampling but were permitted to take prescribed, regular medication. Medications that inhibit gastric acid secretion and those that neutralise gastric acid were discontinued at least 1 week and 1 day prior to gastroscopy, respectively. If a pause in medication was not possible, a note of PPI use was recorded.
Experienced endoscopists performed gastroscopy, as per protocol. Macroscopic findings were recorded and gastric mucosal biopsies were collected from the antrum and corpus, in two separate pots, in accordance with the updated Sydney System (USS) protocol for histopathology.22 All biopsy samples were embedded in paraffin blocks, sectioned and stained [H&E, cresyl fast violet, Periodic Acid-Schiff with diastase] for routine diagnosis at the Department of Pathology, Barts Health NHS Trust, London UK. Histopathologists, who reported on the presence of Hp infection, AG, GIM and dysplasia, examined the biopsies. Gastritis was scored according to the USS classification system.22 Endoscopists and histopathologists were blinded to the GastroPanel results. 5 mL fasting venous blood was evacuated into an EDTA tube from each patient immediately prior to gastroscopy and processed according to the GastroPanel kit manufacturer’s instructions. All plasma samples were transported frozen to Biohit Oyj for analysis using the new generation GastroPanel ELISA test (quantitative analyses of PGI, PGII, PGI/PGII ratio, G-17 and Hp IgG) as per the manufacturer’s instructions.15 Results were interpreted using the GastroSoft app. The GastroPanel test and GastroSoft app correlate with the USS classification of gastritis, and use the same diagnostic categories: (a) normal mucosa, (b) Hp-gastritis (non-atrophic gastritis), (c) AG antrum (AGA), (d) AG corpus (AGC) and (e) pan-AG (AGP).16 17 Laboratory personnel were blinded to endoscopy and histopathology results.
The descriptive statistics were done using conventional tests. Sensitivity (SE), specificity (SP), positive predictive value, negative predictive value (NPV) and their 95% CIs were calculated for the GastroPanel test biomarkers using the algorithm of Seed et al (2001).23 Receiver operating characteristics (ROC) analysis was used to identify the optimal SE/SP balance for both endpoints (AGA and AGC), and AUC values were compared by the roccomp test. The agreement between the different tests was calculated separately using overall agreement (OA) and intra-class correlation coefficient (ICC) tests for weighted kappa. In addition, Fagan’s nomogram24 was constructed to evaluate the post-test probabilities for moderate to severe AGC based on the likelihood ratios of GastroPanel at a population level. All statistical analyses were performed using the SPSS 27.0.1.0 for Windows (IBM, NY, USA) and STATA/SE 17.0 software (STATA Corp., Texas, USA). All tests were deemed significant at the level of p<0.05.
Results
A total of 324 patients with dyspepsia were enrolled into the study. Patient characteristics requested in the GastroPanel referral form, including age, gender and medical history, are summarised in online supplemental table 1s. Patient flow chart is available in the supplemental material (online supplemental figure 1s). Of the 324 patients enrolled, 56.8% (n=184) were female; the median age of the patients was 57 years (range 39–92 years).
Frequency of prior Hp eradication was 4.6%; 54 patients (16.7%) reported PPI use (continuous: 14.2%; occasional: 2.5%), of whom 53 (98%) paused treatment at least 7 days prior to enrolment. Cases that had no GastroPanel result, or no histology report, were excluded from the data analysis. Paired sample sets (biopsy histology and plasma GastroPanel) were obtained from 268 patients (82.7%) [151 females (56.3%); median age=57 (range 39–92 years)] and available for analysis. One out of 268 patients had gastric ulcer in which case GastroPanel was abnormal with a PGI/PGII ratio <1. One micronodular neuroendocrine hyperplasia was identified in the gastric body on histology; however, the GastroPanel sample was haemolysed and was not suitable for analysis.
Initial analysis revealed 46 cases where histology did not match the GastroPanel result; therefore, in these cases, the GastroPanel analyses were repeated, with the original results being reproduced. Three expert histopathologists reviewed the corresponding biopsies. Expert reviewers were blinded to case number, endoscopic findings, previous histopathology reports and all GastroPanel results. Expert diagnosis was used for analysis in the case of discordance with general pathologist’s diagnosis. Expert review of histology and GastroPanel results in the 46 discrepant cases gave an overall agreement of 46%.
USS classified 178 (66.4%), 58 (21.6%), 16 (6.0%), 8 (3%) and 8 (3%) cases as normal, Hp-gastritis, AGA, AGC and AGP, respectively (table 1).
Agreement between GastroPanel classification and histology (USS classification)
The unadjusted OA between the GastroPanel diagnosis and the USS classification was 90% (95% CI=0.867 to 0.938). When adjusted for the correctly diagnosed AGC component of the AGP by the GastroPanel test in 2/8 cases, the adjusted OA was 91% (95% CI=0.876 to 0.944). The non-adjusted and adjusted weighted kappa test (two-test agreement) results were κw = 0.828 (95% CI=0.781 to 0.865) and κw = 0.824 (95% CI=0.776 to 0.861), respectively.
In ROC curve analysis using moderate to severe AGC as the endpoint, AUC for PGI/PGII ratio and PGI were AUC=0.960 (95% CI 0.907 to 1.000) (figure 1) and AUC=0.840 (95% CI 0.630 to 1.000) (online supplemental figure 2s), respectively. In roccomp analysis, the difference in AUC values was not significant (p=0.276) due to a high sensitivity in the PGI ROC curve.

ROC curve analysis of PGI/PGII ratio for detecting biopsy-confirmed moderate/severe AGC. ROC, receiver operating characteristics; AGC, atrophic gastritis corpus.
When conventional cut-offs were applied for PGI (25 µg/L and 30 µg/L) and PGI/II ratio (3.0), PGI and the PGI/PGII ratio demonstrated good performance when diagnosing moderate/severe AGC. At both cut-offs (25 and 30 µg/L), PGI gave a sensitivity and specificity of 75% and 99%, respectively. The PGI/PGII ratio gave a sensitivity and specificity of 75% and 98%, respectively, at a cut-off of 3.0 (online supplemental table 2s). Table 2 shows the precision of GastroPanel as a predictor of AGC in the biopsies.
Performance indicators of GastroSoft AGC profiles in the diagnosis of biopsy-confirmed AGC
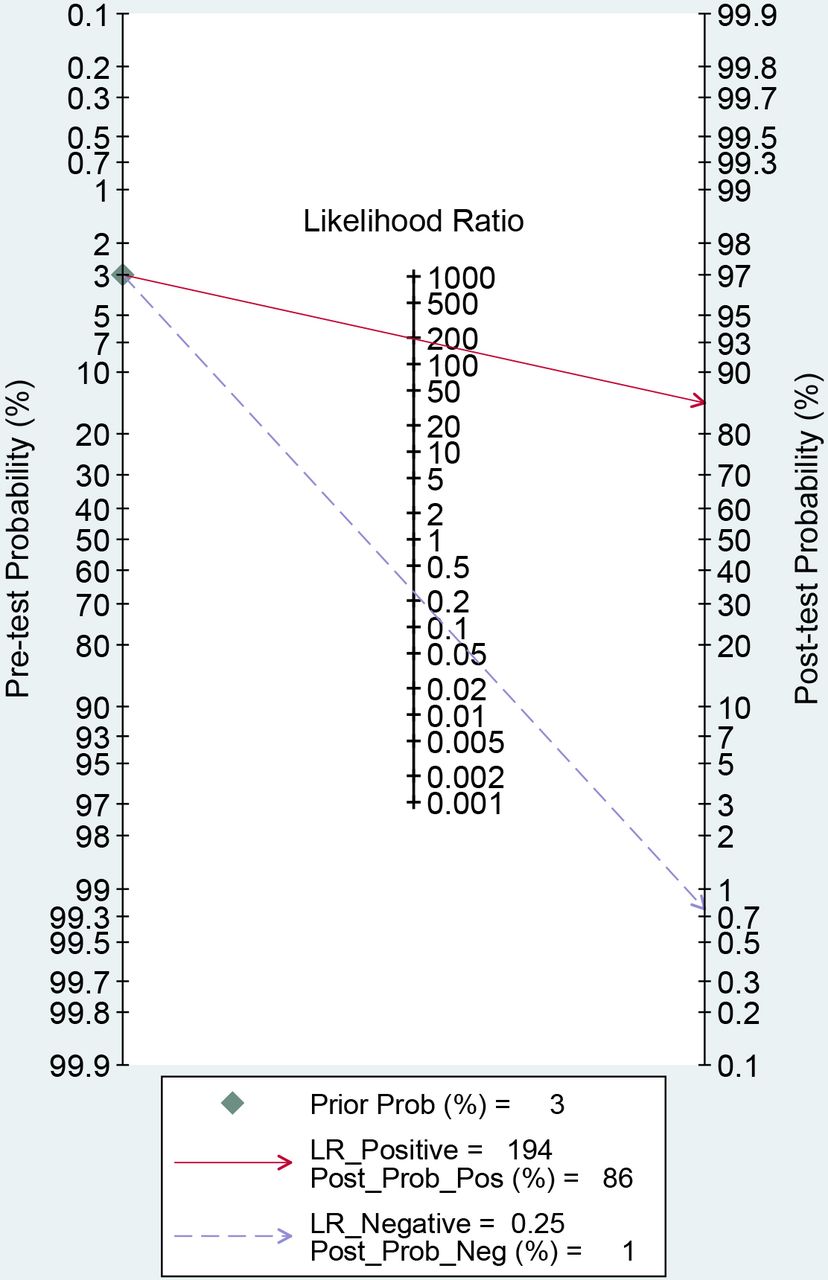
Fagan’s nomogram (figure 2) comparing GastroPanel’s PGI/PGII ratio for the identification of moderate to severe AGC true disease by USS (online supplemental table 2s) showed a positive likelihood ratio (LR+) of 194 and a negative likelihood ratio (LR-) of 0.255, based on a pre-test probability of 3%. When GastroPanel was used as a test to find AGC in a population, the post-test probabilities of identifying and ruling out moderate to severe AGC were 86%, and 1%, respectively.

{kind=link}
{kind=link}
Fagan’s nomogram: GastroPanel as predictor of AGC in a population. Data derived from the PGI/PGII ratio vs AGC2+ calculations (online supplemental table 3s). LR, likelihood ratio; AGC, atrophic gastritis corpus.
G-17 was of limited value in diagnosing AGA (data not shown). For the detection of Hp infection, GastroPanel’s Hp IgG ELISA detected biopsy-confirmed positive and negative Hp infection (any topography) in 52/64 and 174/197 cases, respectively, with AUC=0.858 (95% CI 0.796 to 0.919), as shown in online supplemental figure 3s and online supplemental table 3s. Hp data were missing from seven cases (three Hp IgG, four biopsies).
Discussion
The 2019 British Society of Gastroenterology (BSG) guidelines on the diagnosis and management of patients at risk of GAC25 state that the key to early detection of cancer and improved survival is to non-invasively identify those at risk before endoscopy, and, recommend endoscopic surveillance every 3 years for those with high-risk extensive moderate to severe AG of the corpus mucosa, as well as endoscopic mucosal resection/endoscopic sub-mucosal dissection of visible gastric dysplasia and early GC. Yet, to date, identifying patients with moderate to severe atrophic gastritis and its progressive carcinogenic lesions remains exclusively an endoscopic modality. Endoscopic diagnosis of AG is difficult and is undermined by a low inter-observer agreement at both endoscopy and histology.26
At the current time, UK endoscopy services are experiencing increased workload as predicted by recent models reporting up to a 44% increase in activity over 5 years.27
More than anything else, there is the need to triage patients with functional dyspepsia and healthy stomachs that present for endoscopy. There is also the need to avoid further endoscopy in patients already diagnosed with functional dyspepsia with recurrent symptoms over time. Therefore, an objective, targeted and non-invasive tool for the precise identification of patients with moderate/severe corpus AG who are at high risk of developing GAC or with early cancerous lesions is therefore warranted.
The Operative Link on Gastritis Assessment (OLGA) staging system was developed to deliver to clinicians simple, prognostic value information on the gastritis-associated gastric cancer risk. The OLGA staging system arranges the histological phenotypes of gastritis along a scale of progressively increasing gastric cancer risk from the lowest (stage 0) to the highest (stage IV). Correlation of PGI/PGII ratio with high-risk OLGA stages can predict increased risk of both intestinal type and diffuse type (Lauren classification) gastric carcinoma.28
In our studied cohort, GastroPanel showed excellent agreement with USS classification (90%; 242/268 cases) with a κw of 0.828 (table 1). It identified high-risk moderate/severe AGC with a sensitivity of 75% and a specificity of 99.6% (table 2). Furthermore, Fagan’s nomogram showed if GastroPanel was positive for moderate to severe AGC, it has a positive likelihood ratio of 194 with post-test probability of 86%. When GastroPanel was negative for moderate to severe AGC, the negative likelihood ratio was 0.25 with post-test probability of 1%. This was based on a prevalence of moderate/severe AG of 3%. Encouragingly, our results replicated those of Koivurora et al in a Finnish cohort published recently.29 The prevalence of atrophic gastritis in Koivurova’s study was 10.2%29 while we reported a prevalence of 11.9%, which would imply a marginally higher NPV for the test in the present study population.
In our study, we included the measurement of fasting plasma G-17. Other studies have shown that measuring stimulated (post-prandial) G-17 in addition to fasting G-17 enables the reliable differentiation of antral AG and a non-atrophic antral mucosa.30
This may represent a limitation as fasting G17 alone did not confer benefit in our study and further work is warranted on this marker of AGA.
However, our aim was to target moderate to severe AGC as this endpoint is considered the most clinically significant form of AG and indication for endoscopic surveillance by the expert consensus in the BSG guidelines.
A further limitation of our study was the low number of intermediate pre-neoplastic conditions found in the study cohort. A higher number of preneoplastic conditions would have given more conclusive results. However, our cohort represented those cases referred consecutively with dyspepsia and so represents real life disease prevalence.
Also, the sensitivity of GastroPanel in our study increased when moderate to severe corpus atrophic gastritis was considered as the targeted endpoint, which according to consensus remains the highest risk for GAC. By comparison, in the Koivurova et al study on 522 patients, the AUC for PGI and PGI/PGII was 0.952 and 0.998 respectively, when moderate to severe corpus atrophic gastritis was used as the endpoint.29
In longstanding Hp gastritis, the earliest atrophic lesions involve the mucosecreting antrum and then they steadily spread proximally involving the oxyntic mucosa in the corpus generating the open (O1–O3) patterns of Kimura and Takemoto classification of atrophic gastritis.29 Proximal open patterns (O1–O3) are associated with higher risk of developing gastric neoplasm.31 Patients with atrophic pangastritis are also thought to have an increased risk of developing gastric cancer, to a similar extent to those who have corpus predominant atrophic gastritis. It is only those patients who have antral predominant atrophic gastritis who do not need surveillance gastroscopy according to the 2019 BSG guidelines.
We reported a poor inter-observer agreement between expert pathologists regarding histological interpretation of gastric atrophy in 46 cases. However, all pathologists were blinded to the original diagnosis, and, assessment of low-grade AG can be difficult, as well-established standardised criteria are still the subject of consensus debate.32 33 Moreover, endoscopic evaluation of gastric atrophy needs improvement as has been suggested before—better guidelines and more solid criteria may be needed to appropriately diagnose and grade gastric atrophy.29 33
The use of a clinical scoring system has been proposed to predict the risk of gastric atrophy and gastric cancer in a population with high incidence of gastric cancer.34 The risk score ranged from 0 to 7 based on variables including age, family history of gastric cancer, prior disease history, and PGI and PGI/PGII ratio. This study revealed that medium-risk (score of 3–4) or high-risk (score of 5–7) categories contained a greater number of patients with atrophic gastritis and gastric cancer. These results suggest that the integrated use of GastroPanel with a gastric cancer risk score could be of additional clinical value in risk stratification for selecting patients for urgent endoscopy and form the basis for future safety-netting in a clinical pathway.
The inclusion of Hp serology in the GastroPanel provides important information regarding the role of Hp infection. Despite the risk of false positives for active infection, Hp IgG has an important clinical role in the identification and differentiation of the high-risk AGC group. Hp IgG might also help in the identification of Hp negative autoimmune cases of AG (AIG). Of note, in a recent prospective multicentre cohort study, low PGI levels resulted to be more sensitive than the autoantibodies for the detection of AIG.35
There are other specific clinical circumstances in which Hp IgG is of benefit, such as, low Hp prevalence countries where a high NPV test is of value, when patients have already been prescribed PPI therapy, or when patients are unwilling to undergo invasive tests.36–38 Moreover, antigenic tests for Hp such as faecal antigen or urea breath test can well complement GastroPanel to confirm or rule out the infection in symptomatic patients when pepsinogen I/II are normal. Importantly, in cases where the pepsinogen I/II results indicate AG, Hp would be further investigated using confirmatory histology in the referred cases for gastroscopy. In our study, 65/268 cases were Hp+ on histology (24.3%). Of the 12 cases that had moderate to severe AG (any topography), 3 were Hp+, this might be due to difficulties in the identification of Hp on histology, when gastric atrophy is particularly severe.38 This data is in line with previous studies that reported Hp negative cases with high-risk AG from positive pepsinogen results.7 19
A recent case-control study in the USA showed that subjects with PGI <70 and PGI/PGII ratio <3 had an increased risk of developing non-cardia gastric cancer.39 The cumulative 5 years incidence of gastric adenocarcinoma is 10% for severe atrophic gastritis, and therefore, taking the relatively low prevalence of high-risk AG cases into consideration, GastroPanel has the potential to impact outcomes of patients with gastric adenocarcinoma through earlier detection and diagnosis by applying targeted case selection of patients.
Conclusion
GastroPanel is a reliable triage test capable of distinguishing patients with dyspepsia who can be safely followed up and treated conservatively, from those at high risk of developing GAC, by its negative predictive value. Large-scale clinical studies are encouraged to support pragmatic clinical application of GastroPanel in the dyspepsia pathway to reduce the burden on endoscopy capacity and resources. Further studies should also assess and audit near-patient GastroPanel testing in a primary care setting, to triage dyspeptic patients without alarm symptoms, for gastroscopy.
In terms of wider applications, patients with specific alarm symptoms should be studied which may reveal additional benefits to a wider dyspeptic patient cohort, including better case selection and reducing the burden on the TWW pathway. And, in the future, it would also be of value to evaluate GastroPanel’s potential in the follow-up of patients with histologically and serologically assessed gastric atrophy at baseline, and evaluate the environmental impact potential of GastroPanel on endoscopy in a primary care referral pathway.
Supplemental material
Data availability statement
Data are available upon reasonable request. Data underlying the study will be shared with other researchers on request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committee of the NRES Committee East of England-Cambridge South (15/EE/0205). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We acknowledge the specialist nurse Joy Sadeghian for recruiting and carrying out some of the endoscopies for the study. We would also like to acknowledge NIHR research nurses that helped us with the study as well as all the patients who took part in the study. Biohit contributed only by analysing the plasma samples using the GastroPanel ELISA test, blinded to histology and endoscopy results.
References
Footnotes
Contributors CP contributed to conception of the work, data collection, investigation, statistical analysis, drafted and reviewed the original manuscript. LM, EW and RS contributed to the conception of the work, investigation, data collection and revision of the original manuscript, MN and RF contributed to the conception of the work, histology expert review and data collection. KS contributed to histology expert review, statistical analysis and revision of the original manuscript. NIHR contributed to data collection and patents’ database. Biohit contributed only analysing the plasma samples using the GastroPanel ELISA test blindly to histology and endoscopy results. Biohit was not involved in the design or the analysis of the study. CP is the guarantor.
Funding Health Services Research Programme in collaboration with Industry (Biohit) (Grant no. NA).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.