Article Text

Abstract
Objective In 2019, a BMJ Rapid Recommendation advised against colorectal cancer (CRC) screening for adults with a predicted 15-year CRC risk below 3%. Using Switzerland as a case study, we estimated the population-level impact of this recommendation.
Design We predicted the CRC risk of all respondents to the population-based Swiss Health Survey. We derived the distribution of risk-based screening start age, assuming predicted risk was calculated every 5 years between ages 25 and 70 and screening started when this risk exceeded 3%. Next, the MISCAN-Colon microsimulation model evaluated biennial faecal immunochemical test (FIT) screening with this risk-based start age. As a comparison, we simulated screening initiation based on age and sex.
Results Starting screening only when predicted risk exceeded 3% meant 82% of women and 90% of men would not start screening before age 65 and 60, respectively. This would require 43%–57% fewer tests, result in 8%–16% fewer CRC deaths prevented and yield 19%–33% fewer lifeyears gained compared with screening from age 50. Screening women from age 65 and men from age 60 had a similar impact as screening only when predicted risk exceeded 3%.
Conclusion With the recommended risk prediction tool, the population impact of the BMJ Rapid Recommendation would be similar to screening initiation based on age and sex only. It would delay screening initiation by 10–15 years. Although halving the screening burdens, screening benefits would be reduced substantially compared with screening initiation at age 50. This suggests that the 3% risk threshold to start CRC screening might be too high.
- COLORECTAL CANCER SCREENING
- CANCER PREVENTION
- DECISION ANALYSIS
- SCREENING
Data availability statement
Data from the Swiss Health Survey are not publicly available and can be obtained from the Swiss Federal Statistics Office upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
A BMJ Rapid Recommendation advised against colorectal cancer (CRC) screening for individuals with a predicted 15-year CRC risk <3%.
The distribution of predicted risk in the population is unknown, therefore the population-level impact of this recommendation is uncertain.
WHAT THIS STUDY ADDS
Under the Rapid Recommendation, the vast majority of men and women would not start screening before age 60 and 65, respectively.
Compared with screening from age 50, the number of screening tests would be halved but also approximately 10% of prevented CRC deaths and 19%–33% of lifeyears gained by screening would be lost.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We showed that the recommended comprehensive risk prediction tool does not outperform risk prediction solely based on age and sex, and a 3% risk threshold for screening initiation could be too high.
Introduction
Colorectal cancer (CRC) is the third most common cancer in the world.1 Studies have shown that population-based screening for CRC and its precursors can effectively reduce CRC mortality.2 However, the average lifetime risk of developing CRC is 4%–5%.3 This implies that 95% of individuals will never develop CRC and thus not benefit from screening while they are exposed to its burdens and potential harms. Therefore, individuals ideally make an informed choice to be screened or not, weighing these expected harms and benefits.
Currently, individuals are recommended to start CRC screening between ages 45 and 60 in most Western countries.4–6 In 2019, a BMJ Rapid Recommendation guideline panel proposed screening initiation based on CRC risk instead. This panel summarised and balanced harms, burdens and benefits of CRC screening such as incidence and mortality reduction, required number of screening tests and the risk of complications, given an individual’s predicted 15-year risk of CRC. The panel recommended in favour of CRC screening if this risk exceeds 3% and against CRC screening if the risk is below 3% (weak recommendation), effectively suggesting to start screening when an individual’s risk exceeds 3%.7 For risk estimation, the panel used the QCancer-colorectal risk prediction tool, which uses risk factors such as age, sex, smoking status, alcohol status and prior cancer diagnoses.8 Its discriminative power ranks among the highest of all ‘comprehensive’ tools: those that use variables that are routinely available in the UK biobank or are easily obtained through questionnaires.9
However, the analysis forming the basis of this recommendation did not incorporate the distribution of QCancer-predicted risk in the population.10 Therefore, the population-level impact of the recommendation is unclear. For example, women without any risk factors would be recommended against screening until age 67 because their QCancer-predicted risk does not exceed 3% before that age.11 As a consequence, this recommendation could result in the so-called Geoffrey Rose’s Prevention Paradox12: if a majority of the population is not screened because it is at low risk, while most CRC cases occur in this majority, the Rapid Recommendation will prevent only a minority of these cases.13
Recently, the PREcision ScreENing randomised controlled Trial (PRESENT) in the canton of Vaud, Switzerland, experimented with personalised CRC screening recommendations based on QCancer-predicted risk.14 Using data obtained from and for this trial, our study modelled the long-term impact of the BMJ Rapid Recommendation using Switzerland as a case study. We compared this to age-based screening initiation, as currently practised, to assess whether it will be a case of Geoffrey Rose’s Prevention Paradox.
Methods
First, we estimated the distribution of QCancer-predicted risk in the Swiss screen-eligible population. Second, we incorporated this distribution in the well-established Microsimulation Screening Analysis-Colon (MISCAN-Colon) model to simulate risk prediction with QCancer. Third, using this model, we simulated the population-level impact of risk-based CRC screening initiation as suggested by the BMJ Rapid Recommendation, compared with the current practice of age-based screening initiation. In Switzerland, individuals are currently reimbursed for biennial faecal immunochemical test (FIT) (cut-off 10 or 15 µg/g, depending on the canton) or 10-yearly colonoscopy screening between ages 50 and 69.
Distribution of QCancer risk
To estimate the distribution of QCancer-predicted risk in Switzerland, we used individual-level data from the Swiss Health Survey (SHS).15 This population-based, cross-sectional health interview is conducted every 5 years. Individuals over 15 years old are randomly selected for an interview to answer questions about lifestyle, health status and use of health services. Afterwards, the results are weighted by age, sex, canton, nationality and household size to represent the Swiss population.
At the time of our study, the most recently available SHS was from 2017. However, we used the written questionnaire of SHS 2012 as it included more questions on prior cancer diagnoses, required to calculate QCancer-predicted risk. We calculated QCancer-predicted risk of all respondents to SHS that were old enough to apply QCancer (≥25 years old) and not too old for screening (<75 years). Individuals were weighted by their SHS weight. Online supplemental table S1.2 shows the baseline characteristics of these 14 414 weighted individuals.
Supplemental material
Most questions in the QCancer calculator could simply be matched with SHS variables. All individuals were assumed not to have ulcerative colitis or diagnosed colonic polyps because these are exclusion criteria for routine CRC screening.16 Previous cancer diagnoses and family history of gastro-intestinal (GI) cancer were not available in SHS and were imputed (see the two Imputation sections). Missing entries of other variables were also imputed. We generated 50 data sets using multiple imputation17 to assess the variance of the QCancer risk distribution due to the imputations. More details on matching SHS and QCancer, and the imputations are found in online supplemental appendix 1.1.
Imputation of previous cancer diagnoses
The QCancer calculator considers previous diagnoses of certain cancer types as a risk factor for CRC. However, SHS only captured cancer diagnoses from the past year, and without specifying the cancer type. To address this, individual previous cancer diagnoses were imputed in two steps. First, we assumed that the SHS variables ‘Have you ever been treated for cancer?’ and ‘Have you been diagnosed with cancer in the past year?’ indicated whether someone ever had cancer. Thus, we assumed that individuals with a cancer diagnosis made over a year ago had been treated. Second, we imputed a cancer type for all cancer diagnoses based on the age-specific and sex-specific 10-year prevalence of all cancers in Switzerland in 2012.18 We assumed that everyone had been diagnosed with only one cancer type.
Imputation of family history of GI cancer
SHS neither registers family history of GI cancer nor a suitable alternative. We randomly imputed GI cancer family history using the age-specific and sex-specific prevalence of CRC family history.19 In the base case, we assumed an average prevalence of 7.3%.
MISCAN-Colon microsimulation model
MISCAN-Colon is a well-established microsimulation model that has informed CRC screening guidelines in various countries.20–22 It simulates individuals from birth to death and some develop adenomas and/or CRC. By simulating various CRC screening strategies for these individuals, the model evaluates the impact of screening. An extensive model description has been published previously.20 23 For our case study, we developed separate models for Swiss men and women by adjusting the Dutch version of MISCAN-Colon. In short, we used data from Swiss cancer registries to recalibrate the sex-specific model parameters for risk of adenoma onset by age, speed of CRC diagnosis and CRC survival, in line with the successfully validated approach of Gini et al.24 More details are found in online supplemental appendix 2.
Risk prediction in MISCAN-Colon
In MISCAN-Colon, each individual is assigned an underlying ‘true’ lifetime risk of developing adenomas. The distribution of this underlying risk in the population was previously calibrated to match international adenoma prevalence and CRC incidence estimates.20 In reality, the underlying risk is unobservable: we can only observe predicted risk as calculated by QCancer. Therefore, in the simulation, every individual was also assigned a QCancer-predicted risk whenever they completed the QCancer tool.
QCancer is not a perfect risk predictor, thus an individual’s predicted and underlying risk typically do not align perfectly. Nevertheless, there is a correlation between predicted and underlying risk and the strength of this correlation depends on the predictive accuracy of QCancer. We calibrated this correlation using an elliptical copula approach (online supplemental appendix 3).25–27 Ultimately, an individual’s QCancer-predicted risk depended on this calibrated correlation, and the individual’s sex, age and underlying risk in the simulation.
Analysis
Screening strategies
We simulated two types of CRC screening strategies: risk-based and age-based. Risk-based screening started when an individual’s QCancer-predicted risk exceeded a specified threshold, similar to the Rapid Recommendation. Besides the suggested threshold of 3%, we also simulated thresholds of 1%, 2% and 4% to study the effect of alternative risk-based screening start criteria. We assumed that predicted risk was calculated every 5 years, thus individuals that exceeded a 3% risk by age 62 would actually start screening at age 65. Age-based screening started at a fixed age for all individuals. We simulated four screening start ages (50, 55, 60 and 65), which were most comparable to the chosen risk-based strategies. This includes the current Swiss recommendation to start screening at age 50.28
We evaluated these eight screening strategies by simulating a birth cohort of men and women separately. We used biennial FIT (cut-off 15 µg/g) for screening. Screening stopped after age 75 because the screening stop age in Switzerland will be extended in the near future. After a positive FIT, individuals were referred for a follow-up colonoscopy. When adenomas were detected during colonoscopy, individuals would undergo colonoscopy surveillance according to Swiss guidelines.29 We assumed full adherence to screening tests, follow-up colonoscopies and surveillance. Other assumptions such as test performance and colonoscopy complication rates can be found in online supplemental appendix 4.
As a reference, we also simulated a scenario without screening, whereby patients would only undergo colonoscopy when they presented symptoms of CRC.
Outcomes
First, we reported the estimated distribution of QCancer-predicted risk for 20 age and sex groups (25–29, 30–34, …, 70–74 for both sexes). Second, given that simulated individuals calculated their QCancer risk every 5 years, we calculated the distribution of the starting age of screening for both sexes (online supplemental appendix 3.1).
Third, we simulated the sex-specific population-level benefits, burdens and harms of the eight screening strategies. Benefits included prevented CRC cases and deaths and lifeyears gained (LYG) by screening. For screening burdens, we used the number of screening tests (FITs or screening colonoscopies) and number of individuals who had at least one or two colonoscopies (all colonoscopies). Screening harms were defined as the number of hospitalisations due to complications from any colonoscopy. All outcomes were reported per 1000 40-year-old men or women without CRC because 40 was the earliest age individuals would start risk-based screening. Additionally, we reported two burden-benefit ratios: the number of screening tests per CRC death prevented by screening (Number Needed to Screen, NNScreen), and the number of individuals who had at least one colonoscopy per CRC death prevented (Number Needed to Scope, NNScope). All outcomes were lifetime outcomes, which contrasts the analyses for the Rapid Recommendation, which reported them for a 15-year time window.7 10
Sensitivity analyses
In sensitivity analyses, we first repeated our analyses with annual FIT and, second, with 10-yearly colonoscopy screening instead of biennial FIT. Third, we assumed a higher prevalence of GI cancer family history (on average 10% instead of 7.3%) because it is likely underestimated by the prevalence of CRC family history used for the imputations. Fourth, we assumed a lower prevalence of GI cancer family history (4.87%) because we used UK CRC family history prevalence for imputations. This may have overestimated the family history prevalence in Switzerland because CRC incidence in the UK is approximately 50% higher than in Switzerland (online supplemental appendix 1.1).30 Fifth, we estimated the distribution of QCancer risk from the results of the PRESENT study, which required other assumptions than SHS (online supplemental appendices 1.2 and 3.4). The study participants gave informed consent for their data being processed.14 Sixth, we used the Dutch version of MISCAN-Colon to evaluate the impact of the Rapid Recommendation in a country at higher risk of CRC. We assumed the same distribution of QCancer risk factors as in Switzerland but a different natural history of disease. Seventh and eighth, we estimated the impact of the BMJ Rapid Recommendation when using a hypothetical, more discriminative risk prediction tool in Switzerland and The Netherlands, respectively. This tool had an area under the curve (AUC) of 0.84, independent of age and sex, and was perfectly calibrated to the Swiss or Dutch population (online supplemental appendix 3.5), rather than the estimated AUC of 0.66–0.70 for QCancer which includes age and sex.9
Patient and public involvement
Although patients have not been directly involved in this modelling study, they have been involved in the overall design and implementation of the overarching PRESENT study.14
Results
Distribution of QCancer risk
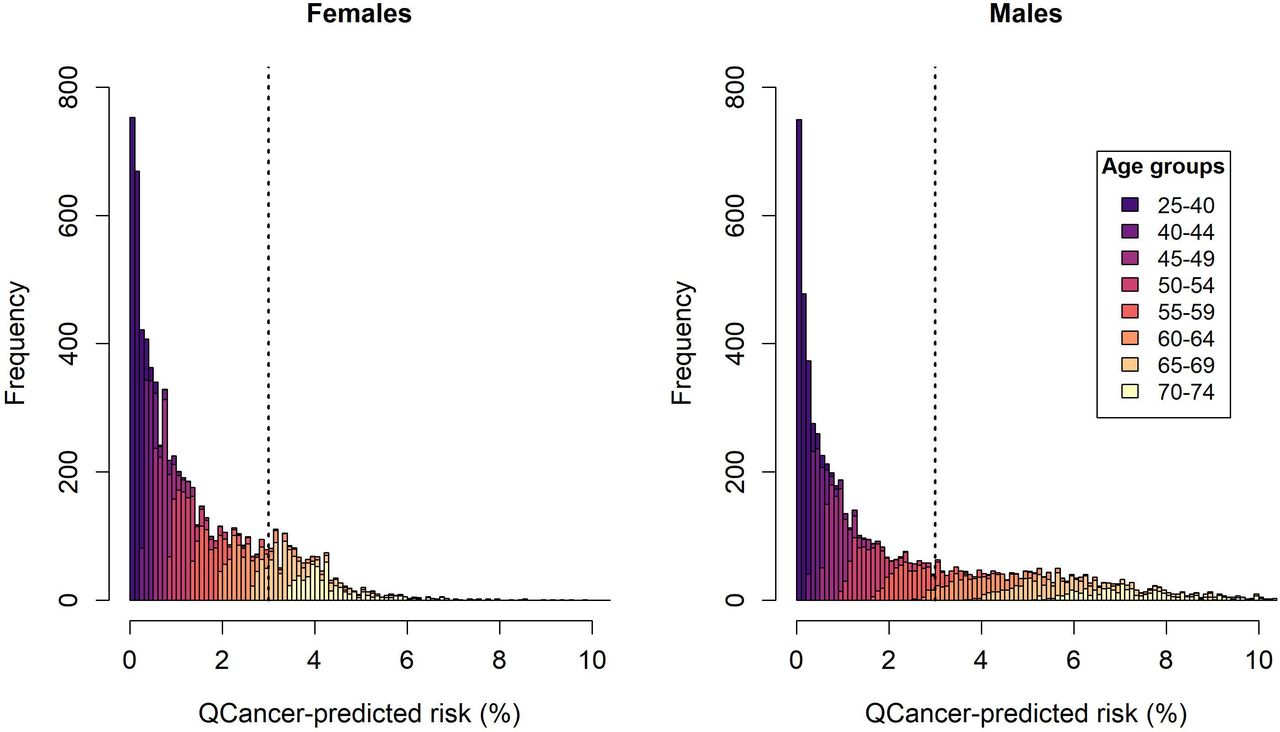
Figure 1 shows the median of the 50 imputed QCancer risk distributions by sex. The variance of the 50 imputations was negligible (online supplemental appendix 1.1.3), so we proceeded with the median distributions of both sexes. Overall, QCancer assigned a wide range of risk scores to the population, from 0 to above 10%. However, the risk distributions of separate age groups were relatively narrow, especially in age groups below 60 years, and their overlap was remarkably limited. For example, only 3.1% of women in age group 50–54 had a higher risk than the women with the lowest risk in age group 60–64. For men, this was only 4.6%. This shows that age is a very important risk factor in QCancer. Similarly, QCancer-predicted risk exceeded 3% for all men and women in age group 70–74, but for only 1.6% of men and 0.3% of women aged 50–54.

Distribution of QCancer-predicted risk in the full Swiss Health Survey cohort, stratified by sex. The colours represent the distributions of 5-year age groups. The vertical, dotted line indicates the 3% risk threshold for screening as suggested by the BMJ Rapid Recommendation.
Distribution of screening start age
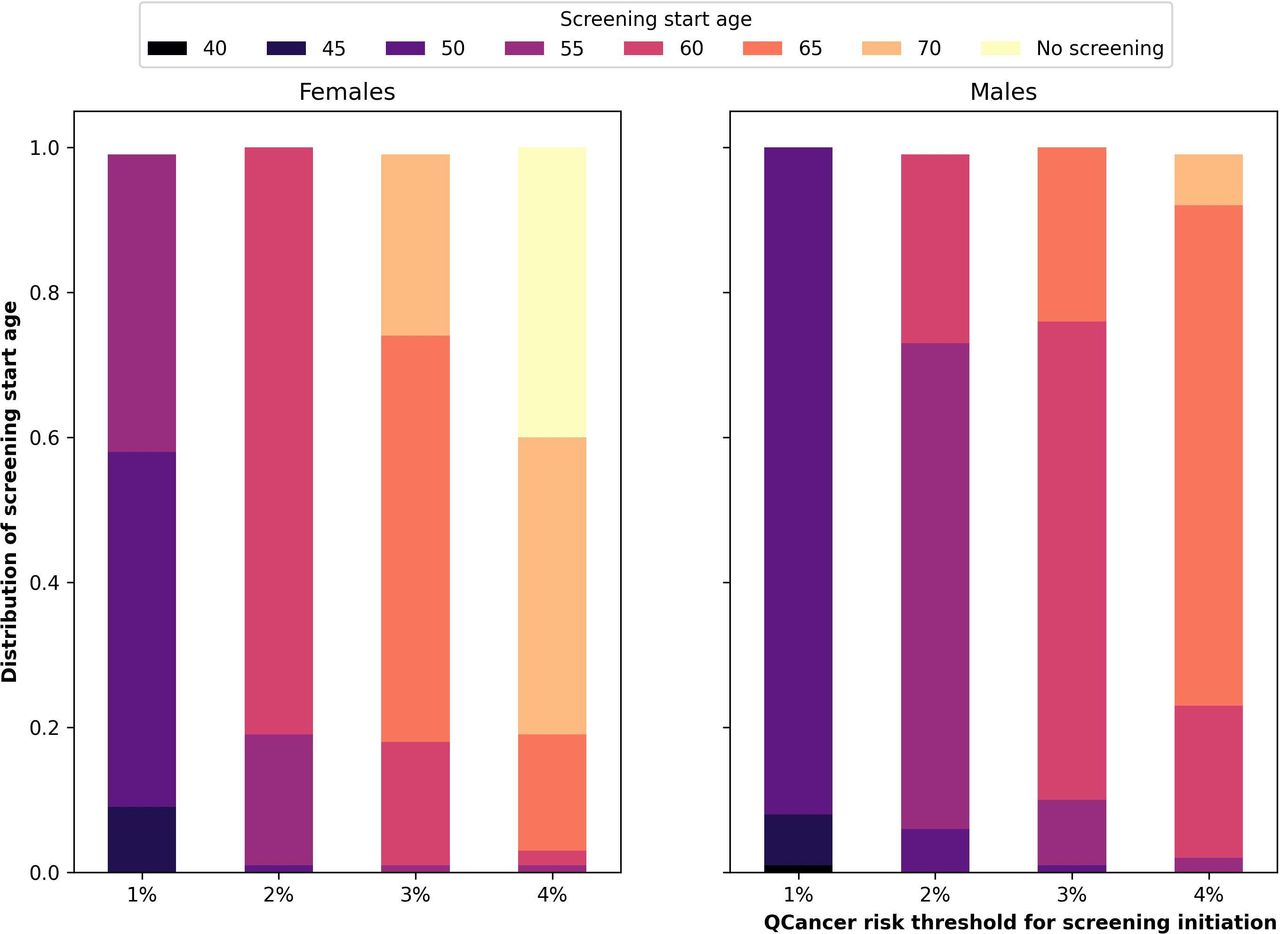
For all four risk thresholds (1%, 2%, 3% and 4%), most individuals of the same sex would start screening at the same age (figure 2 and online supplemental appendix 5.1). For instance, at a threshold of 3%, 56% of women started screening at age 65, and 66% of men started at age 60. In fact, 82% of women would not start screening before age 65, and 90% of men would not start screening before age 60.

Proportion of women and men that would start screening at a certain age given the used risk threshold for CRC screening initiation. We assumed individuals would complete the QCancer risk tool every 5 years. CRC, colorectal cancer.
When increasing the risk threshold for screening initiation, the screening start age increased as well. For example, with a risk threshold of 1%, 49% of women and 92% of men would start screening at age 50. With a risk threshold of 4%, 40% of women would never be screened because their risk only exceeded this threshold after the age of 70.
MISCAN-Colon simulations
Screening initiation at 3% risk
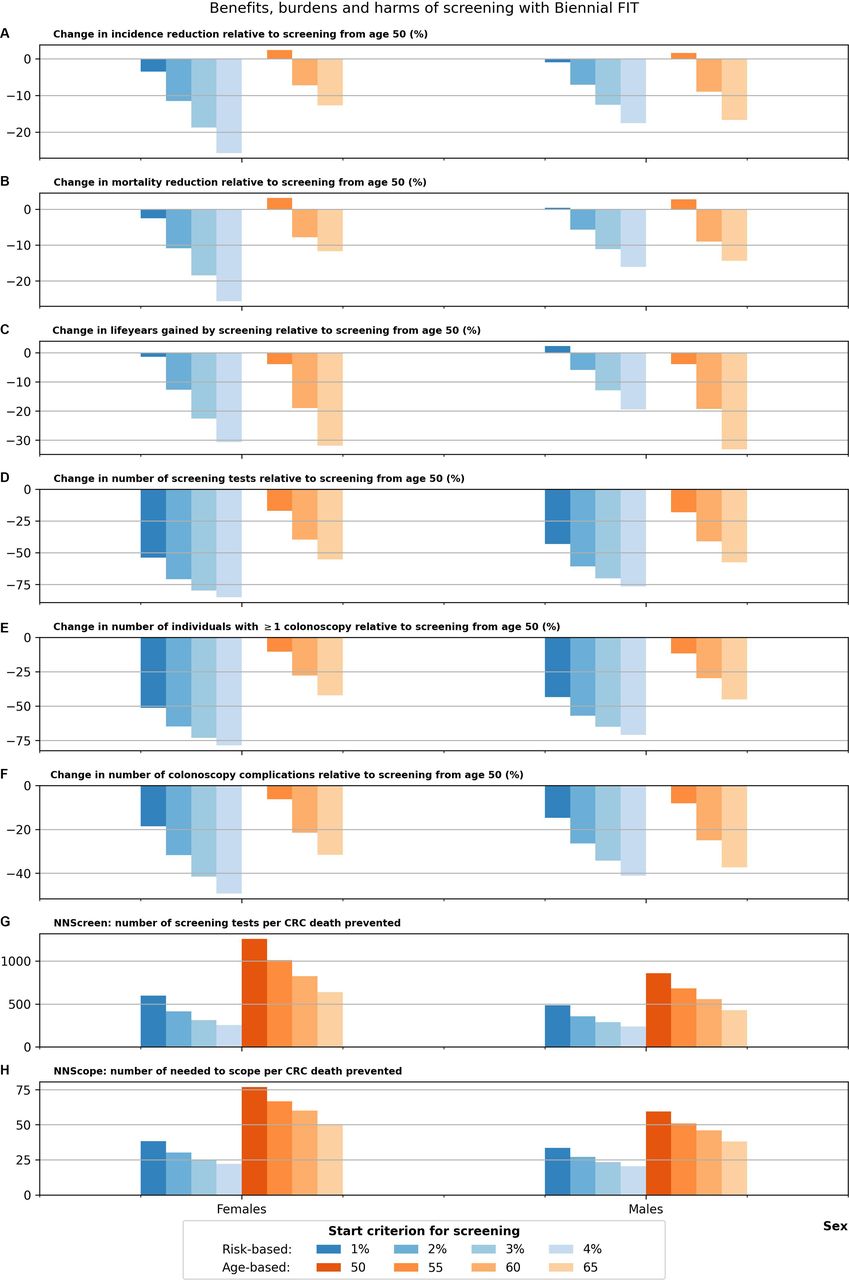
MISCAN-Colon predicted that risk-based screening, starting when an individual’s QCancer-predicted CRC risk exceeds 3%, would lead to a reduction in all screening outcomes compared with age-based screening from age 50. Prevented CRC deaths would decrease by 15.6% for women (from 7.7 to 6.5 CRC deaths per 1000 CRC-free 40-year olds, see figure 3 and table 1). For men, prevented CRC deaths would decrease by 7.8% (from 10.3 to 9.5 CRC deaths prevented). The 3% threshold would result in a 32.9% loss in LYG for women (from 103.8 to 69.7) and a 19.1% loss for men (from 125.7 to 101.7). However, it would also require 57.2% fewer FITs (9655 to 4130) for women and 42.6% fewer FITs (8852 to 5083) for men. Other screening burdens and harms would also be reduced by 25%–61%. The predicted NNScreen would decrease from 1258 to 638 for women and from 858 to 537 for men.

Relative change in model-predicted screening outcomes of risk-based and age-based screening compared with screening from age 50. (A) Incidence reduction. (B) Mortality reduction. (C) Lifeyears gained by screening. (D) Number of screening tests. (E) Number of individuals with ≥1 colonoscopy. (F) Number of colonoscopy complications. (G) NNScreen: number of screening tests per CRC death prevented. (H) NNScope: number of individuals needed to scope per CRC death prevented. CRC, colorectal cancer; FIT, faecal immunochemical test.
Outcomes of the base case and sensitivity analyses with biennial FIT
Age-based screening and risk-based screening yielded similar outcomes. For example, compared to screening from age 50, a screening start age of 65 would lead to a reduction in prevented CRC deaths (11.7% loss to 6.8 CRC deaths prevented) and LYG (31.8% loss to 70.8 LYG) similar to the 3% risk threshold. Moreover, the decrease in required FITs would be similar (55.2% to 4322), and it would yield an equal NNScreen (637 per death prevented). For men, a screening start age of 60 yielded a similar reduction in outcomes as the 3% risk threshold: compared with screening from age 50, CRC deaths prevented, LYG and number of FITs would be reduced by 8.7%, 19.3% and 41.1%, to 9.4 cases, 101.4 LYG and 5211 FITs, respectively. The NNScreen would be 555.
Other screening start criteria
A 2% risk threshold for screening initiation would lead to a decrease in all outcomes compared with screening from age 50 for females, and similar number of cases and deaths prevented at slightly increased LYG, harms and burdens (figure 3 and online supplemental appendix 6.1). In general, a 2% threshold yielded outcomes very similar to screening from age 60 for women and age 55 for men. A 1% threshold would lead to negligible changes in screening outcomes, thus be very comparable to screening all men and women from age 50.
Of note, figure 3 shows that delaying screening initiation from age 50 to 55 would lead to slightly more cases and deaths prevented while all other outcomes, including LYG, decreased. This is because the age to stop screening is also delayed from age 74 to 75 due to the 2-year FIT interval.
Sensitivity analyses
With annual FIT screening, a 3% risk threshold remained comparable to screening women and men from age 65 and 60, respectively, and lead to a similar reduction in screening outcomes as for biennial FIT. Colonoscopy screening had a smaller reduction in screening impact although it would not outperform age-based screening (online supplemental appendices 6.2 and 6.3). Variations in the prevalence of GI cancer family history, using PRESENT data or using the Dutch natural history of disease, neither lead to risk-based screening outperforming age-based screening (table 1 and online supplemental appendices 6.4–6.7).
When using substantially improved risk prediction tools in Switzerland, a 3% risk threshold still resulted in an 11%–23% loss in screening benefits compared with screening from age 50 (figure 4 and online supplemental appendix 6.8). This is because the majority of the population never reaches a 3% risk (online supplemental appendix 5.2). Screening harms and burdens, however, would be reduced by as much as 34%–80% when using a 3% threshold. Notably, a 1% threshold would yield increased mortality reduction (0.4%) and LYG for men (2.3%) and a small loss in other benefits (0.9–3.5%) at a substantial reduction in harms and burdens (15%–54%). In The Netherlands, a 3% risk threshold combined with the hypothetical risk prediction tool would lead to a 3.6%–8.9% reduction in benefits and a 20%–67% reduction in harms and burdens (table 1 and online supplemental appendix 6.9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative change in screening outcomes of risk-based and age-based screening compared with screening from age 50 for sensitivity analysis 7 assuming a hypothetical, better risk prediction tool for risk stratification. (A) Incidence reduction. (B) Mortality reduction. (C) Lifeyears gained by screening. (D) Number of screening tests. (E) Number of individuals with ≥1 colonoscopy. (F) Number of colonoscopy complications. (G) NNScreen: number of screening tests per CRC death prevented. (H) NNScope: number of individuals needed to scope per CRC death prevented. CRC, colorectal cancer; FIT, faecal immunochemical test.
Discussion
This study modelled the population-level impact of a 3% risk threshold for CRC screening initiation as suggested by the 2019 BMJ Rapid Recommendation. When using QCancer for risk prediction, the burdens and harms of screening would be halved compared with the current Swiss recommendations to start screening from age 50. At the same time, however, it would decrease CRC cases and deaths prevented by up to 16%, and LYG by up to 33%. Its impact would be similar to using age and sex as risk factors alone: screening all women from age 65 and men from age 60. Our final two sensitivity analyses predicted that with a better, yet hypothetical risk prediction tool, a 3% threshold for screening initiation would still yield a substantial loss in screening benefits of up to 23% and 9% in Switzerland and The Netherlands, respectively. However, a lower risk threshold for screening initiation could yield similar screening benefits at significantly reduced burdens compared with screening based on age and sex.
The poor performance of risk-based as compared with age-based and sex-based screening initiation is because age and sex substantially impact QCancer-predicted risk. Our study showed that QCancer mainly uses age to discriminate between high-risk and low-risk individuals of the same sex. This aligns with external validation studies: while QCancer had an impressive discrimination in a cohort of 25 to 84-year olds (AUC±0.85),8 this reduced significantly in a cohort aged 40 to 69 (AUC 0.66–0.70).9 Similarly, in the same cohort, the AUC of the risk prediction tools without age as a risk factor did not exceed 0.56.9
Our distribution of QCancer-predicted risk is in line with previous estimates. 15-year risk of CRC was estimated at typically 1%–2% at age 50 in Europe and North America,7 and 1%–7% at ages 40–69 in the UK.10 In our study, 78% of SHS responders aged 50–54 had a 1%–2% risk, and 60% of SHS responders aged 40–69 had a risk of 1%–7%. The majority of the remaining 40% had a risk below 1%, which concurs with the known higher baseline risk of CRC in the UK compared with Switzerland.30
Other modelling studies also predicted that risk-based screening does not necessarily improve the balance between screening burdens and benefits in realistic scenarios. Frampton et al31 modelled risk-based screening initiation, similar to the BMJ Rapid Recommendation, based on polygenic risk (AUC=0.63) and age. Although this would lead to 16%–17% fewer screen-eligibles, it would yield 8%–10% fewer screen-detected CRC cases. It is debatable whether such a reduction in benefits outweighs the reduction in burdens. Ladabaum et al32 defined three risk groups and assigned each a different screening intensity (10-yearly, 5-yearly or once-only colonoscopy). They predicted that this approach would only be cost-effective in the extreme case of perfect risk prediction. Naber et al26 predicted polygenic-risk-based screening strategies to be cost-effective for an AUC ≥0.65 and costs of polygenic testing of up to US $100. However, they identified 12 risk groups, each requiring a different screening strategy, which might be challenging to implement in practice. Notably, when their model was extended by van den Puttelaar et al27 to incorporate risk prediction of other-cause mortality, an AUC of 0.65 for CRC risk prediction was found insufficient to be cost-effective.
Our study is the first to assess the long-term population-level impact of the Rapid Recommendation. An important strength of this study is it using the most reliable data sources available for Switzerland. Nevertheless, there are several limitations to note. First, as with many population health surveys, the SHS is prone to healthy population and social desirability biases.33 34 The true distribution of QCancer risk might be higher on average and more heterogeneous than reported if unhealthy lifestyle is under-reported and unhealthy subjects are under-represented. Second, QCancer was developed for the UK population and would ideally be recalibrated to the Swiss or Dutch population. However, it is unlikely that a recalibrated QCancer tool for these countries, nor the original tool applied to the UK population, is more independent from age and sex. Third, we only modelled FIT and colonoscopy separately. In reality, most Swiss programmes have the benefits, harms and burdens of offering the choice between both screening tests. Finally, we calibrated MISCAN-Colon to historical CRC incidence rates and stage distributions from a period before (opportunistic) CRC screening to more accurately model the likely effects of screening. As a consequence, we were limited to reliable CRC stage distribution data from the urban canton of Geneva, which might not be representative for Switzerland.
Notwithstanding these limitations, our results have important implications for clinical practice. First, they suggest that screening based on QCancer-predicted risk should not be considered for population-based screening programmes because it does not outperform screening simply based on age and sex at population level. Instead, the QCancer questionnaire could even negatively impact screening effectiveness as it may be a potential barrier to screening participation. Our study predicts that improved risk prediction tools do have potential to outperform age-based screening initiation. For example, risk prediction tools using prior negative FIT results achieve higher AUCs35 36 and do not require individuals to complete a questionnaire. Second, the recommended 3% threshold for screening initiation should be reconsidered. Using QCancer for risk prediction, it would result in considerably delayed screening initiation for the vast majority of the Swiss population, which is in sharp contrast with recent changes in some CRC screening recommendations,5 and in substantial losses in screening benefits, especially for women. This likely holds for other Western countries as well because it is unlikely that the difference in CRC risk between countries is fully explained by differences in risk factors included in the QCancer tool. Yet, even with the substantially improved risk prediction tool from our sensitivity analyses, a 3% risk threshold would yield losses in screening benefits compared with screening from age 50, although they were small for Dutch men. Since Switzerland and The Netherlands have one of the lowest and highest age-standardised CRC incidence rates in Europe, respectively, the 3% threshold will likely yield losses in nearly all European countries.30
To summarise, the BMJ Rapid Recommendation to not screen individuals whose 15-year risk of CRC is below 3% would likely halve screening burdens and harms in Switzerland. Unfortunately, it would also substantially reduce screening benefits, especially for women. This could be considered an example of Geoffrey Rose’s Prevention Paradox, whereby screening mostly high-risk individuals would miss a large portion of CRC cases that occur in low/moderate risk groups. Furthermore, risk-based screening using QCancer does not outperform screening based on age and sex alone. Given these results, we should reopen the discussion on the appropriateness of discouraging individuals to be screened if their 15-year risk of CRC is below 3%.
Data availability statement
Data from the Swiss Health Survey are not publicly available and can be obtained from the Swiss Federal Statistics Office upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This modelling study used individual-level data from the PRESENT trial. The study protocol of this trial (project ID 2021-02431) was approved by the ethics committee of the canton of Vaud on 2 March 2022 (Plys et al, Colorectal Cancer Screening Decision Based on Predicted Risk: Protocol for a Pilot Randomized Controlled Trial14). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to acknowledge the National Agency for Cancer Registration (NACR) for providing CRC mortality and stage-specific incidence and survival rates for Switzerland, and Prof. Elisabetta Rapiti, Geneva Cancer Registry, for validating the Geneva stage-specific data. Moreover, they acknowledge the other members of the PRESENT Trial Steering Committee, Prof. Reto Auer, Dr. Marie-Anne Durand and Aziz Chaouch, for their valuable inputs to the PRESENT trial which served as a basis for this paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LAvD: conceptualisation, investigation, formal analysis, validation, interpretation of results, writing—original draft. LAvD acts as a guarantor for the paper and its contents. J-LB: conceptualisation, interpretation of results, supervision, writing—review and editing. EM: investigation, formal analysis, interpretation of results, writing—review and editing. RvdP: validation, interpretation of results, writing—review and editing. EP: investigation, validation, interpretation of results, writing—review and editing. KB, DC, FF, KS: conceptualisation, interpretation of results, writing—review and editing. ILV: conceptualisation, interpretation of results, supervision, writing—review and editing.
Funding This study was funded by the Swiss Cancer Research Foundation (KLS-5111-08-2020). KS receives salary support from the Leenaards Foundation. ILV is funded in part by a Vidi grant (09150171910047) from the Dutch Research Council (NWO). RvdP and ILV were (partially) supported by grant U01-CA253913 from the National Cancer Institute (NCI) as part of the Cancer Intervention and Surveillance Modeling Network (CISNET). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders did not have any role in the design of this modelling study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.