Article Text

Abstract
Context French interns in general practice are, like all medical students, exposed to medical errors during their training.
Objective To measure the professional and personal impact of medical errors on French general practitioner (GP) trainees.
Design, setting and participants Quantitative and qualitative study of medical errors and GP trainees enrolled at Paris Diderot University.
Method An online anonymous questionnaire was sent to all GP trainees at Paris Diderot University and recorded semi-structured interviews were conducted with 10 volunteers.
Results 70 of the 392 (18%) interns contacted replied to the questionnaire and 10 semi-structured interviews were then conducted. 97% of the participants had already made a medical error. Even with the extreme, conservative assumption that non-respondents would have reported no errors, the prevalence of self-reported medical errors in the whole sample would still have been 17%. 64% said they were at least strongly affected by their error and 74% made constructive changes to their work after the error. The interns revealed that the emotional impact of their errors were great with feelings such as guilt that could remain for more than 2 years after the event. 33% would have liked to talk more about the circumstances of their error with their superior. Most interns suggest more training on medical errors and more open-minded discussion when the error actually happens rather than formal training at the university.
Conclusion Medical errors remain a sensitive subject that is not broached enough in our university but interns need to talk about their experiences with their peers to improve risk management and prevent the recurrence of new errors.
- Medical error
- general practice trainee
- impact
- management
- general practice
- medical education
- human error
Statistics from Altmetric.com
Introduction
Since Kohn's ‘To err is human’1 was published in 2000, risk management and improvement of patient care have been at the heart of many studies in the USA and the UK. As in all countries, the French public authorities have published a series of alarming statistics on undesirable events: the ENEIS report2 showed that out of 35 000 days of hospitalisation in public hospitals in 2005, there were 450 undesirable events.
Even though Wu introduced the term ‘second victim’ more than 20 years ago,3 the notion is still relatively little known in France. The French medical journal Prescrire has set up a programme to signal and analyse medical errors called ‘Avoid the avoidable’.4 It also helps find an attentive ear in case of distress caused by the event. The few doctors who admit to having made a medical error of their own can recall their need for help from a colleague.5
There is a growing body of literature concerning doctors in training and medical errors in the USA and the UK,6–11 but few studies have evaluated the professional and emotional impact and the management of medical errors by doctors in France,12 and none have studied general practitioners (GPs) in training. We therefore decided to evaluate the impact of medical errors on GP interns, the way they deal with them, and how their formal curriculum, concerning medical errors, could be improved with a quantitative and qualitative study.
Method
Subjects
All interns (392) enrolled in the GP training programme of the Paris-Diderot University, Paris, France received an email in July 2010 inviting them to answer an anonymous questionnaire about medical errors, via the GP's department website.
Questionnaire
The anonymous questionnaire was developed after a review of the literature. No written consent was sought but it was specified that any answer on the website was considered as an inclusion in the study.
The first question ‘Have you ever had the impression of making one or more medical errors?’ enabled us to distinguish two groups according to the answer yes or no. The ‘yes’ group was then presented with 15 questions, 11 of which were multiple choice questions and four of which were open-ended questions which the interns could answer without any word limit. The multiple choice questions used categorical response formats. All the questions concerned the most recent mistake the interns could remember. The first four questions were epidemiological and then followed a series of nine questions that concerned the mistake in itself and the impact it had on their professional and personal lives and how they dealt with it.
The ‘no’ group had seven multiple choice questions which were all four-point Likert-type formats. The interns were asked how frequently they thought about medical mistakes and the following questions concerned a supposed mistake and the interns were asked on what scale they would have felt responsible for the mistake; how much they would reveal to the patient; what they would answer if the patient asked about the mistake; how they would react from a professional point of view; how they would feel; and what they would expect from their medical supervisors.
The interns were not given a definition of what the descriptive categorical terms meant (severe, medium, benign or null, and high, medium, low): they judged what these terms meant and decided in which category their mistake should be sorted.
Both groups shared the same last question which was ‘According to you, what is the definition of a medical error or what terms should figure in the definition?’ This was an open-ended question that could be answered without justification as to why the interns chose those particular terms.
Semi-structured interviews
Subjects could participate in a semi-structured interview. These interviews were conducted face to face and recorded with a digital voice recorder, between July and October 2010. Ten interns volunteered for the interviews and all of them were accepted without knowing what their mistake was and without looking for an even number in gender or level of training and without aiming for saturation of data. All interns were assured confidentiality and there was no way we could link the interviews to the surveys. Each intern was asked to talk about a mistake they believed they had made. The recordings were transcribed by one author (EV). Two authors (EV, EG) then independently analysed the transcripts.
Statistical and non-statistical analysis
Statistical analysis concerning the questionnaire and the interviews was conducted using descriptive statistics, mostly percentages for categorical variables. Categorical variables were compared using a Pearson χ2 test.
Non-statistical data found in the open-ended questions of the questionnaire and in the interviews were analysed according to methods commonly used in qualitative evaluation.
Results
Characteristics of respondents
Of the 392 interns contacted, 70 (18%) answered the questionnaire. Out of the 70, 97% said they had the impression they had already made a medical mistake and only 3% said they had never made a mistake. Even with the extreme conservative assumption that non-respondents would have reported no errors, the prevalence of self-reported errors in the whole sample would still have been 17%. The majority of the interns (71%) said they had made between two and five mistakes since starting their training as a GP. Most mistakes (55%) were made in the first year and a half (out of 3 years) of training and decreased with experience. Thirty-six per cent of the interns talked about mistakes that had happened less than 3 months before answering the questionnaire and 30% about mistakes more than a year old.
Most errors were made in accident and emergency departments (A&E) (26%), followed by internal medicine (24%) and by a mistake in a private practice with a GP (19%) (table 1).
Characteristics of respondents
Definition of medical mistake
Fifty-four per cent (n=38) of the respondents answered this question and included one to six different ideas per answer. The interns were asked to give a general definition of the notion of medical error but it seems reasonable to infer that they were also reporting, at least partially, on how they were defining their own specific events when answering the survey. The link between personal experience and a general notion is even more probable when talking about medical errors because it is a difficult and delicate subject.13 The fact that 11% of the interns specified that it was ‘unintentional’ sounds odd. It is quite probable that they needed to defend themselves and deal with their guilt while answering this question. Nevertheless, the most frequent notion was that it was an action that was ‘harmful’ for the ‘patient’ (n=15) and caused by the ‘doctor’ (n=8). Others gave answers that included the terms ‘negligence’, ‘violation’ or ‘near-miss’, ‘diagnosis’ or ‘treatment’. These interns were probably referring to their own specific experience. table 2 shows the different notions that appeared in order of frequency.
Definition of medical error or the terms that should figure in the definition
Ten semi-structured interviews were conducted with the 10 interns who volunteered. Ninety per cent of the interviewees talked about mistakes that had happened either in their first or second year of internship rather than their last year. The mistakes they discussed happened in an A&E department for 50%, internal medicine for 30%, geriatrics for 10% and paediatrics for 10%. table 3 summarises the 10 interviews.
Summary of the 10 interviews
Outcomes of the mistakes on the patients
This analysis of outcomes was solely in the form of a self-assessment of what had happened. In the questionnaires, 33% of the interns estimated that the mistake they had made had severe consequences for the patient. Ninety per cent of the interviewed interns said their mistake had severe consequences for the patients.
A χ2 test showed that, for interns, the more severe the estimated consequences of their mistake for the patient, the stronger the personal impact on them (Q=23.06>K=16.92 with degree of liberty 9, tolerance α=0.05).
Ninety-one per cent of the interns thought they were at least half responsible for the error. No intern thought of their mistake as being inevitable. These results were confirmed in the interviews (table 4).
Estimates by the interns of the outcomes of mistakes on patient (n=55)
A Pearson χ2 test showed that the more the interns thought they could have avoided their mistake, the more they felt responsible for their mistake (Q=6.7>K=5.99 with degree of liberty 2, tolerance α=0.05).
Professional and emotional impact
Sixty-four per cent of the interns said they felt at least a strong impact after the error. To analyse its professional impact, it was decided to categorise the changes made as a consequence of the error as constructive or defensive, as did Wu.13 Seventy-four per cent of the interns made constructive changes which were mainly additional checks of the clinical exam, prescriptions, biological and radiology exams “I make sure that I have double-checked all the biological exams I prescribed”, making sure the patient perfectly understood what he had been told, taking more time to make crucial decisions and asking more frequently for advice from senior doctors or specialists. Some interns said they did not hesitate to brush up on what they had learnt rather than relying on their sometimes faulty memory.
The most common defensive change was the excessive fear of a group of symptoms or diagnosis that made the interns order extra tests: “as soon as someone has painful legs they get a Doppler ultrasound”.
One aspect that was only revealed in the interviews was how the interns suddenly felt incompetent and generated a highly negative image of themselves: “it was something I could have avoided and that was just not the sort of doctor I wanted to be”, “I thought I should just give up, change career and open up a B&B”.
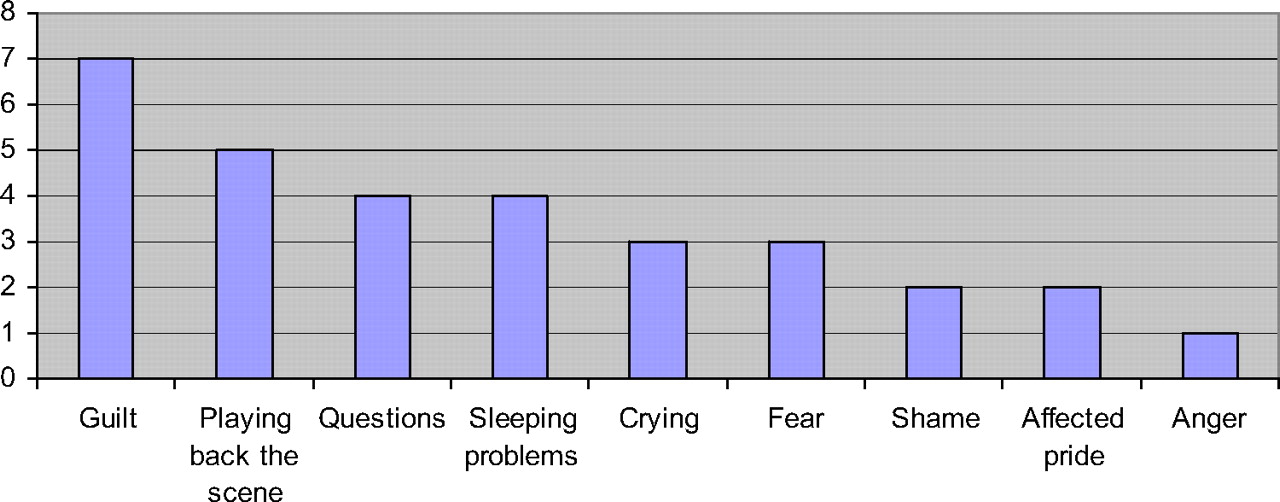
The emotional impact of the mistake was only analysed in the interviews: a wide variety of feelings were described by the interns, the most frequent one being guilt (figure 1).

{kind=link}
Emotions felt by the interns in the interviews. There was more than one emotion felt by each interviewed intern.
Five interviewees thought about their mistake for a long time and replayed the scenario in their minds. This was especially true for two interns who could not place their finger on their mistake, but who felt they had not done enough to save their patient and therefore tried to figure out what had gone wrong over and over again: “every time I saw someone, I had to speak about what had happened … I replay the scene to see what I could have done differently”.
How the interns dealt with the mistake
The most difficult aspect to deal with was the consequences of the mistake on the patient's health. Most interns felt they would have been better able to deal with this had the department they were placed in already had procedures in place, to include a more thorough discussion about what had led to the error, and more group discussions about the way they actually felt (table 5).
What could have helped interns prevent and deal with their mistake
One intern said in his interview that he would have liked “just to sit around a coffee and for someone to ask me ‘so, how are you feeling?’”.
Another issue the interns had to deal with was the reaction of some of the physicians after the mistake. In seven interviews, an intensive care unit (ICU) doctor intervened because the clinical situation was severe, but a third were described to have had a negative reaction to the situation and criticised what the intern had done. One intern said “I came back the next day and the ICU doctor just screamed at me ‘what the hell happened?’ without trying to understand the situation I had been in”. These negative reactions were unfortunately also quite frequent with the A&E doctors: half of the interns said they were criticised without analysing the situation, by the person who was supposed to be teaching them: “you got everything completely wrong, you've got to learn how to examine a patient”, “that women with abdominal pain you saw the other day … she nearly died and it's all your fault”.
Disclosure
Only 57% of the interns disclosed their error to a medical supervisor. These interns estimated its consequences as severe or average. In the interviews, the interns detailed who they had talked to about their mistake: 80% had told their supervisor, 80% had also told a friend or family member. When asked if they received the support they expected, the interns only talked about the support from the senior doctor they had disclosed the error to. More than one intern specified that their family, even if they were doctors themselves just “couldn't understand unless they were there at the time, no-one could”. Overall, 29% of the interns estimated the support from their superior was perfect and 27% said they received no support whatsoever.
Only two interns disclosed their mistake to the patient. We did not ask the interns why they chose for or against disclosure to their patients but the interviewees said that they were “too ashamed” or “too scared of what the patient might think”. Sixty per cent of the interviewees admitted having brief thoughts about possible litigation following their error. However, this does not seem to be the reason why they chose not to talk about it: “it swept very quickly over my mind but it wasn't the problem: the main problem was that I'd destroyed a family. If they had wanted to sue I would even have found it normal”.
Trainees' perception of medical error taken at face value
No evaluation was made by the author as to whether the trainee had actually made a medical error, or that medical error had actually caused a patient harm. However, the vast majority of respondents thought they had already made a mistake which shows that like all doctors in training worldwide, we are concerned by this problem. Because this was a self-assessment of mistakes, with personal estimates of how responsible the interns each felt for the error and how severe they judged the consequences, there is possibly a larger number of mistakes reported than if the senior doctors were asked for their opinion: some of the doctors who reviewed the study thought the reported errors were more of an unlucky turn of events despite the best possible care given by the intern, rather than a real error. This reinforces the importance of disclosing our mistakes to our superiors: it may be that we remain with a very strong sense of guilt for something that they wouldn't even judge to be a mistake, like West showed could be the case.14
Discussion and recommendations
Our study received responses from 18% of those enrolled in the GP training programme of our university. The most probable explanation for the relatively low number of participants is that medical errors are still a subject that we hesitate to talk about in the French medical community. The relative lack of literature on the subject in French confirms this. However, supposing that all the interns who decided not to participate had made no mistakes, there still remains one out of five that admits to having made one or more medical error since they started their training: it is a subject that should therefore be broached systematically in our training programme, rather than in optional courses.
Medical errors are a sensitive subject and the general definition given by the interns in the survey was probably influenced by the different situations the interns met and by their own professional identity.13 The main purpose was to measure the professional and emotional impact of mistakes on GP trainees. On the professional side, like Wu's interns,15 the constructive changes made by the interns were very encouraging and illustrate that most are capable of learning from their mistakes, even if they doubted their own competence.
The interviews explored the emotional impact of the errors, the main limitation being that the interns who volunteered for them were probably the most affected. Guilt, as in Newman's study,16 was the most frequent feeling evoked, even after several years, as Christensen et al17 said could be the case.
Concerning the support they received from the supervising physicians, the interns mostly reported the lack of analysis of the error. They would have preferred to have had a form of debrief of the whole event, just to understand what had led to the error so as not to repeat it. They also insisted that even if they felt guilty, they did not want their superiors to minimise their error. Kroll et al9 suggested that it closes down the discussion if the interns cannot freely express what went wrong and how strongly they feel. Most interns said that they would also have liked their superior to acknowledge the fact that they themselves had made an error at least once in their career, but they had not stopped practising medicine.
Some interns had to face another problem, that Galam has called ‘double victim’: not only did they already feel very badly about having made a mistake but they were overly criticised and condemned by some physicians who were supposed to teach them. How can interns be expected to disclose medical errors to their superiors if they fear they will be criticised without any sort of analysis of the mistake?
Disclosure to patients is something that we have to work on: only two interns told their patient what had happened. As we do not have any form of formal teaching about medical mistakes in our university, there is no teaching about disclosure either.
Most interns, however, were not keen for any formal teaching about errors while at university but preferred to have group discussions. In our opinion if our training programme included just a few hours about medical errors, their possible professional consequences and the emotions they can induce, then maybe interns would find it easier to talk about them to their superiors, their colleagues and their patients.
The lack of knowledge about medical errors was also underlined by the many definitions of medical error suggested by the interns. As GP trainees they had received no formal teaching about medical responsibility. Even though the interns are not too preoccupied as yet by the growing sense of intrusion of law suits into the French medical system, there will come a time when they will need to have a more precise idea about the potential legal consequences of their possible errors.
This study helped us to show that there are several gaps in our training as future GPs that could be easily filled: first of all, the creation of forums for group discussion around mistakes, to help each other understand that we are never alone and to help prevent the same mistake happening twice. It seems that a few hours spent on medico-legal issues could help us understand how the legal system can impinge on the medical world and to whom we should turn should we ever need legal advice. It should be suggested to our medical supervisors that medical mistakes are clearly something that interns think about before and after having made them, and that it would be easier for all if it were clear who to turn to and what to do if a mistake should occur during our courses in hospital or in a private practice.
Additional studies concerning French medical interns and the impact of medical mistakes need to be conducted. It is clear that such studies are too few in number to force changes in our training and in understanding how French students deal with medical errors. If we can talk more freely about our mistakes, we will always try to work towards improving patient care by minimising risks and developing a healthy work environment for all physicians.
Acknowledgments
We thank all the interns who answered the survey and the 10 interns who volunteered for the interviews. We also thank Mr Guillotin for his help on the statistics.