Article Text

Abstract
Objectives: To review the incidence and characteristics of preventable childhood deaths in an urban population in the UK and to determine whether the excess of preventable deaths seen previously in Asian girls still exists.
Design: A retrospective survey of childhood deaths from 1996–2002 classified in terms of preventability and compared with a previous study conducted 20 years earlier from 1976–82.
Setting: The city of Wolverhampton in the UK.
Main outcome measures: Deaths from all causes in children under the age of 5 years.
Results: There has been a reduction in the number of deaths in all age groups and from all causes. The postneonatal mortality rate fell from 6.5/1000 in 1976 to 3.1/1000 live births in 2002 largely because of the fall in the numbers of deaths caused by sudden infant death syndrome (SIDS). Preventable deaths are still associated with low birth weight (p<0.001) and poverty (unemployment and overcrowding in the earlier study (p<0.05) and with the Townsend score in this study (p<0.02)). There were fewer deaths among Asians and no female excess. There was a new category not seen in the previous study, deaths caused by homicide. The death rate for homicide in the first year of life was much higher in Wolverhampton (18.7/100 000) than in England and Wales (4.6/100 000).
Conclusions: Low birth weight and adverse socioeconomic conditions remain important factors associated with preventable deaths. There is no longer an increased risk of preventable death in Asian girls. The number of non-accidental deaths is a major cause for concern.
- CPI, Child Poverty Index
- SIDS, sudden infant death syndrome
- sudden infant death syndrome
- postneonatal mortality
- socioeconomic deprivation
Statistics from Altmetric.com
Childhood mortality is a good indicator of the health of children in the population. Wolverhampton has consistently had one of the highest childhood mortality rates in the UK. Twenty years ago, a retrospective survey of all deaths in children under the age of 5 years in the city of Wolverhampton found a significant association between adverse social factors and preventable childhood deaths and, unexpectedly, an excess of girls among the preventable deaths in children of Asian origin.1 Since then death rates for all age groups have been falling steadily in line with the national trend, suggesting that some of these deaths are indeed preventable.2
The aim of the present study was to compare the current mortality rates from preventable causes with the previous study and determine whether the sex difference among Asians still exists in Wolverhampton.
METHOD
Deaths occurring in children under the age of 5 years between 1 January 1996 and 31 December 2002 and whose parents place of residence was the city of Wolverhampton were studied and compared with a similar study of children who had died between 1 January 1976 and 31 December 1982.1 Cases were identified from the Registrar’s returns and each death was classified according to preventability.1,3,4
Only deaths in group A (deaths with a very poor prognosis) were regarded as inevitable. All the others were regarded as possibly preventable and a more detailed study of these deaths was undertaken.
Information was taken personally from community and hospital records and included sex, birth weight, ethnic origin, mother’s age, area of residence, and adverse social factors. Adverse social factors included one or more of the following: single parent or absent father (for example, in prison or working away from home), mother aged less than 20 years, financial difficulties, inadequate childcare or refusal of health advice, child in care (fostered), behavioural problems in child or sibling, learning difficulties in parent, mental health problems in parent or sibling, history of drug abuse in parents, domestic violence, repeated non-attendance for hospital or clinic appointments, maternal language difficulties, overcrowded home, or other housing problems.
The 20 electoral wards in the city were ranked according to the number of preventable deaths per 1000 live births over the seven year period. Spearman’s rank coefficient of correlation was used as a measure of the association between mortality and various indicators of deprivation taken from the 1981 census in the earlier study and the Townsend score and the Child Poverty Index (CPI) in this study.
RESULTS
There has been a steady decline in mortality for all age groups since 1976 but a much smaller decline in the birth rate. All the mortality rates showed a greater reduction in the earlier study. There was no improvement in the postneonatal mortality rate between 1996 and 2002 (table 1 and fig 1).
Childhood mortality in Wolverhampton 1976–2002

Sudden infant death syndrome as a proportion of postneonatal mortality for Wolverhampton and England and Wales (three year rolling averages).
Causes of death
Congenital abnormalities and obstetric complications, particularly prematurity accounted for more than half the deaths in both study periods (table 2). About a quarter of deaths were due to congenital abnormalities and this proportion was relatively constant and similar to the national figure.5
Childhood mortality in Wolverhampton in children aged under 5 years 1976–2002 classified according to preventability
Compared with 20 years ago, far fewer children are now dying from birth injuries, accidents, and treatable conditions (categories B and C). The number and proportion of sudden unexpected deaths fell considerably between the two studies but fewer sudden deaths had positive findings at necropsy in the present study, suggesting that fewer children die from unrecognised illness.
The most disturbing finding was the number of children who died as a result of abuse. There were no such deaths in the earlier study although it is possible that some deaths registered as sudden infant death syndrome (SIDS) may have been the result of smothering.6
Preventable deaths
There were 100 children in the earlier study and 34 children in this study whose deaths may have been preventable (table 2, groups B–F). Table 3 shows the characteristics of these two groups which both show a significantly lower birth weight compared with the population but that a higher percentage of children in the recent group lived in a deprived area of the city and had adverse social factors.
Data on children whose death may have been preventable
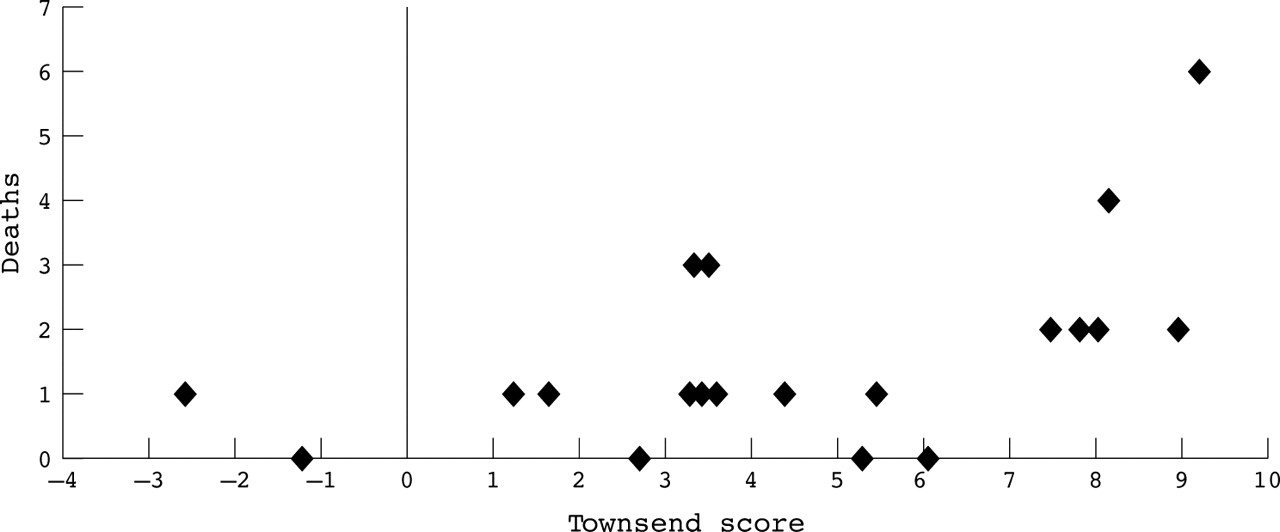
Possibly preventable deaths were significantly associated with socioeconomic deprivation in both studies. In 1976–82 a significant association was found between overcrowding at >1.5 people per room (p<0.05), lack of household amenities (p<0.01), unemployment (p<0.05), and low car ownership (p<0.01).1 In 1996–2002 preventable deaths were related to the Townsend score (Spearman’s rank coefficient of correlation: r = 0.544, p<0.02) and to the CPI (r = 0.382, p = <0.1). Over one third (36%) of deaths occurred in the three wards with highest CPI and Townsend scores (fig 2).

{kind=link}
{kind=link}
Relation between Townsend Score and preventable deaths (r = 0.544, p<0.02).
The main difference between the two groups is in ethnicity and sex. In the earlier study the incidence of possibly preventable deaths was significantly higher in Asian girls than in non-Asian girls or in Asian boys (p<0.05).1 In the present study the expected male predominance was found for all ethnic groups.
Between 1976 and 1982 the number of deaths among Asians was higher than would be expected for the population (28% compared with 23% Asian live births) whereas in the present study the number of deaths in Asians was much smaller, reflecting the reduction in live births to Asian mothers and was similar to the proportion of Asians in the population (12.1% compared with 13%) (table 3).
The seven deaths which were the result of deliberate harm were each the subject of a case review under part 8 of the Children Act. These children had all been identified in life as vulnerable and were all known to social services. They shared a number of characteristics including the very young age of the parents (median age 18.5 years; range 17–27 years), a lower than average birth weight, and adverse social factors such as a history of domestic violence in the family, drug or alcohol misuse, or intergenerational cycles of deprivation and abuse. There were concerns about parenting skills and lack of support from the families of these young parents, some of whom had learning difficulties. Six of the seven children died as a result of intracranial haemorrhage and four of these were under 4 months old.
DISCUSSION
Many changes have taken place in Wolverhampton in the 20 years between the two studies. Wolverhampton itself has become a city and the population has become materially more affluent as judged by a 60% fall in the unemployment rate. The link between material deprivation and child mortality is well known in the UK.7–9 Improvements in the general standard of living as well as improvements in healthcare and education have undoubtedly contributed to the overall reduction in childhood mortality but the deprived areas of Wolverhampton have remained largely the same despite inner city regeneration programmes. These areas continue to show high mortality rates and preventable deaths continue to be associated with poverty.
SIDS
Post neonatal mortality and deaths from SIDS were relatively stable both in Wolverhampton and in England and Wales until the late 1980s when they began to fall (fig 1). A national campaign to “reduce the risks of cot death” in 1991 resulted in a change in the usual sleeping position from prone to supine and is commonly held to be the most important factor in reducing the mortality rates,10 but figure 1 shows clearly that both SIDS and postneonatal mortality rates were already falling well before 1991. Reduction in poverty, improvements in infant healthcare, and increased awareness of the dangers of cigarette smoke to infants will all have contributed to reducing the mortality rates.
Since the early 1990s the SIDS rate has been fairly constant and the association with poverty has become more pronounced with a considerable excess of sudden infant death in families in which neither partner was employed.11
Low birth weight
The consistent finding of an association between preventable death and low birth weight accords with many other studies.4–6,9 Both preterm delivery and poor intrauterine growth are associated with the same social and economic factors that affect the risk of sudden infant death.12 The most recent national data on SIDS show a striking increase in SIDS mortality with decreasing birth weight and this is likely to be related to the increasing levels of deprivation seen in SIDS families13 Poor postnatal weight gain is also associated with an increased risk of SIDS. This seems to be independent of birth weight, prematurity, and social status and may be a useful additional tool in identifying infants at risk.14
Asian deaths
Sex discrimination in South Asia leading to a reversal of the female biological advantage with sex selective abortions, female infanticide, and neglect of girls has been reported recently.15,16 Following the earlier study, Asian baby girls were recognised as a vulnerable group in Wolverhampton and link workers were appointed to work particularly with Asian mothers. This, together with the assimilation of the Asian minority group into the local population, may have contributed to the disappearance of the Asian sex difference. Asian mothers in Wolverhampton are now mostly second generation, language is no longer a problem, and cultural differences are less obvious. In England and Wales as a whole, however, there is still a significantly higher mortality among girls whose mother was born in Pakistan.17
Mother’s place of birth rather than ethnicity may be a better indicator of language and communication difficulties preventing access to good health care. Families seeking asylum in the UK are often housed in the most deprived inner city areas. These families living in relative poverty face many of the same difficulties today as did the Asian groups 20 years ago. Recognition of these vulnerable groups in areas with high immigration may be important in reducing infant mortality rates in the future.
Deaths attributed to maltreatment
There are about 30 infant deaths per year attributed to homicide in England and Wales (4.6/100 000 live births).18 In Wolverhampton, four of the seven deaths due to maltreatment were in infants under the age of 12 months giving a summated rate for the seven year period of 18.7/100 000 live births, considerably higher than the national rate. Because the numbers are relatively small this could be a chance variation. However, since the end of the study period there have continued to be one or two deaths due to maltreatment each year in Wolverhampton suggesting that this trend is continuing.
Six of the seven deaths were the result of intracranial haemorrhage probably caused by violent shaking, but there were at least two more non-fatal cases of non-accidental head injury in Wolverhampton during the study period. In Scotland, the annual incidence of all non-accidental head injury (including survivors) was found to be 24.6/100 000 children under 1 year old.19
The relation between poverty and violence and the effect this has on the incidence of child maltreatment merits further study in similar urban populations in the UK. The risk factors for fatal child abuse found in a large North American study were similar to those found in Wolverhampton, and included young poorly educated mothers with more than half occurring before the fourth month of life.20
It is unlikely that there were no deaths from child abuse in Wolverhampton 20 years ago but they may not have been recognised. In Leeds there were major concerns about abuse or neglect in 10 of 37 unexpected deaths in infancy.21 The risk factors for SIDS and child abuse are similar and an evaluation of two prediction scores for SIDS found that these also predicted high risk for non-accidental injury.22 Failure to distinguish between deaths due to maltreatment and natural causes of sudden infant death may place other children at risk. All sudden and unexpected deaths must be subject to a thorough investigation which should include a meticulous history, detailed postmortem examination, forensic, toxicological, and metabolic investigations, and a multidisciplinary case review.23,24 The creation of a compulsory national investigation protocol as recommended in the Kennedy report will reduce the chance of misclassification of the death or miscarriage of justice.25
What is already known on this topic
-
Poverty and low birth weight are associated with preventable death in childhood.
-
Postneonatal mortality has fallen over the past 20 years largely due to the reduction in deaths from SIDS.
-
Higher infant mortality has been found among Asian girls in the UK as well as in South Asia.
-
Risk factors for SIDS and child abuse are similar.
What this study adds
-
Fewer children die from preventable causes now compared to 20 years ago.
-
Poverty continues to have a major impact on childhood mortality.
-
The birthplace of the mother may be more important than ethnicity in predicting vulnerability.
-
In Wolverhampton, deaths from child abuse have become more prominent as the SIDS rate has fallen.
CONCLUSIONS
Improvements in childhood mortality rates over the past 20 years in Wolverhampton are related to improvements in the general standard of living, while the reduction in preventable deaths may be the result of better care. The greater reduction in mortality rates in the earlier study and the increased deprivation among the preventable deaths in this study suggests that further improvements in childhood mortality may be more dependent on improvements in social circumstances than on health care. The number of deaths due to maltreatment is of concern particularly for the child protection services in the city.
The reversal of the Asian sex difference reflects assimilation of this minority group into the local population. Mother’s place of birth and degree of prosperity may be more important than ethnicity in predicting vulnerability and this may be important with regard to recent immigrant families.
Acknowledgments
The author thanks David Goda for help with the statistics.
REFERENCES
Footnotes
-
Funding: none
-
Competing interests: none
-
Ethical approval: the Chair of the local ethical committee was consulted and was of the opinion that this study was essentially an audit and so did not require formal ethical committee approval