Article Text

Abstract
Objective To examine trends in diagnosis of gender dysphoria and related conditions in children and young people attending primary care practices in England.
Design Longitudinal analysis of electronic primary care records from the Clinical Practice Research Datalink (CPRD) Aurum database linked to hospital and Index of Multiple Deprivation data.
Setting Primary care practices in England between 2011 and 2021.
Participants 3782 patients aged 0–18 years with a recorded history of gender dysphoria/incongruence and matched comparators with autism spectrum conditions or eating disorder.
Main outcome measures Incidence rates and prevalence of gender dysphoria/incongruence; prescribing rates for medical treatments; co-occurrence of anxiety, depression and self-harm.
Results Between 2011 and 2021, incidence rates of recorded gender dysphoria/incongruence increased from 0.14 (95% CI 0.08 to 0.20) to 4.4 (95% CI 4.1 to 4.7) per 10 000 person years, and from 2014 the rate increased more rapidly in recorded females than males. There was no significant association between gender dysphoria/incongruence and area level deprivation. Of the 3782 children and young people with a record of gender dysphoria/incongruence, 176 (4.7%) were prescribed puberty suppressing hormones; 302 (8.0%) were prescribed masculinising/feminising hormones; and 1994 (52.7%) had a record of anxiety, depression or self-harm. Compared with matched comparators, those experiencing gender dysphoria/incongruence had similar recorded rates of anxiety and higher rates of depression and self-harm.
Conclusions Recorded prevalence of gender dysphoria/incongruence increased substantially in children and young people between 2011 and 2021, particularly in recorded females. Levels of anxiety, depression and self-harm were high, indicating an urgent need for better prevention and treatment of mental health difficulties in these patients.
- Child Health
- Epidemiology
- Primary Health Care
Data availability statement
Data may be obtained from a third party and are not publicly available. Data were derived from the Clinical Practice Research Datalink (CPRD) Aurum primary care dataset (https://www.cprd.com/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Historically, gender dysphoria/incongruence was rarely recorded in children and young people, but incidence has recently increased sharply in several countries, particularly for females.
Mental health and neurodevelopmental conditions appear to be common in children and young people experiencing gender dysphoria/incongruence, but prevalence estimates vary widely.
Most previous studies have assessed small populations attending specialist services, with few studies based in primary care, the usual place of first contact for patients.
WHAT THIS STUDY ADDS
There was a 50-fold increase in recorded prevalence of gender dysphoria/incongruence in children and young people in primary care in England between 2011 and 2021.
Despite this increase, gender dysphoria/incongruence remains uncommon in these age groups, affecting fewer than 1 in 200 young people aged 17–18.
Recorded rates of anxiety, depression and self-harm were high for children and young people experiencing gender dysphoria/incongruence, particularly for those with multiple conditions.
There was no consistent relationship between gender dysphoria/incongruence and area deprivation in this age group.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
There is an urgent need to tackle vulnerability to mental health difficulties and improve mental health support for children and young people experiencing gender dysphoria/incongruence.
Primary care services require support and guidance to ensure effective coordination of care for children and young people with multiple complex needs.
Introduction
Over the last decade, rapid rises in the numbers of children and young people presenting with gender dysphoria/incongruence or identifying as transgender have been reported in several countries.1–3 In England and Wales, referrals to the Tavistock and Portman’s Gender Identity Development Service (GIDS)—until its closure in 2024, the only NHS funded specialist service for under 18s with gender dysphoria/incongruence—rose markedly during the 2010s4 resulting in lengthy waiting times, uncertainty for patients and families, and increased pressure on primary care. Interventions offered by GIDS ranged from psychosocial support to medical intervention overseen by specialist paediatric endocrinologists, the latter treatments beginning with puberty suppressing hormones (typically gonadotropin-releasing hormone analogues, GnRH-a) and progressing to feminising or masculinising hormones in most cases.5 There is, however, a lack of robust evidence for the long-term effects of these interventions, particularly medical treatments.6–11
The rise in gender dysphoria/incongruence has been more rapid for birth-registered females4 12 and mental health concerns and neurodevelopmental conditions, including autism spectrum conditions, are more common than in the general population,13 although estimates of co-occurrence vary widely.14 Research in this area has proved challenging, in part due to low numbers of children who are generally managed by specialist providers, and there have been few population-based studies based in primary care, the usual place of first contact with health services. McKechnie et al explored trends in transgender presentation in general practices in the UK, finding incidence increased in the 2010s, with the greatest increases in adolescent and young adult age groups.15 Their analysis focused on rates of diagnosis across all age groups, however, and did not report on co-occurring conditions or treatments.
In this study, we used electronic patient records to (1) describe trends in incidence and prevalence of gender dysphoria and/or incongruence in people aged 0–18 presenting to primary care practices in England; (2) estimate the frequency of treatment with puberty suppressing hormones and masculinising/feminising hormones; and (3) describe recorded rates of anxiety, depression and self-harm compared with children and young people with other complex conditions. Children with a record of autism spectrum condition or eating disorder were selected for comparison as these conditions can have similar clinical aspects of need and concern, for example, elevated rates of anxiety, depression, social isolation, self-harm and body-related distress and discomfort.16 Children with these conditions can also have long waiting times in accessing specialist NHS services.17 18
Methods
Data
Data were derived from the Clinical Practice Research Datalink (CPRD) Aurum primary care dataset, which contains anonymised electronic medical records—including diagnoses, prescriptions and referrals—for over 13 million active patients (19.8% of the population) registered with general practices in the UK.19 Clinical data for children with a record of experiencing gender dysphoria and/or incongruence before age 19 years were extracted from 1 January 2009 (or patient first registration date if later) until 31 December 2021 (or patient end of registration date or last practice data collection date if earlier). Data were also extracted for two comparator groups: children with a recorded history of autism spectrum condition or eating disorder. Comparators were matched on year of birth and geographical region, with a target ratio of 5:1 (without replacement), and patients with a history of gender dysphoria/incongruence were excluded from matching. Further details on matching and its limitations are given in online supplemental appendix A.
Supplemental material
Codes used for study conditions included diagnostic, treatment, symptom and referral codes (see online supplemental appendix A). Patient records were linked by CPRD to Office for National Statistics death registration data; Hospital Episodes Statistics admitted patient care, outpatient and Accident and Emergency data; and Index of Multiple Deprivation (IMD) 2019 categories.
The final study population consisted of 3782 children and young people with a record of experiencing gender dysphoria/incongruence, 18 740 matched comparators with autism spectrum conditions, and 13 951 matched comparators with an eating disorder (for whom low numbers restricted matching to 3.7:1). Descriptive statistics for the study population are provided in table 1. Our main analysis covers the period from 2011 to 2021 because very low numbers for gender dysphoria/incongruence before 2011 make sub-analysis underpowered. Summary results for all years are provided in online supplemental appendix D.
Descriptive characteristics of study population. For co-occurring conditions, figures indicate any history of the condition
Demographics
For each child in each year, age was estimated by subtracting year of birth from the index year due to lack of more detailed date of birth data (ie, someone born in 2000 was deemed to be 18 for the whole of 2018). Deprivation, grouped into five categories, was assigned to individuals based on postcode of last known residence and measured using the Index of Multiple Deprivation (IMD—2019 version).20 Gender is recorded by practices as ‘male’, ‘female’ or ‘other’; only the most recently recorded gender is available in the dataset. In general, ‘other’ is very rarely used (see table 1), but for patients with a record of gender dysphoria, 2.4% had their gender recorded as ‘other’ and were excluded from sub-analyses by gender due to low numbers.
Analyses
Incidence and prevalence
Incidence rates of gender dysphoria/incongruence were estimated by dividing numbers of first recording of gender dysphoria/incongruence in each year by the person-time at risk (calculated as time present in each year for all persons without a known prior gender dysphoria/incongruence diagnosis). Prevalence was estimated on 1 July in each year as the number of people present with a first diagnosis of gender dysphoria/incongruence on or before 1 July in that year divided by the number of people present on 1 July in that year. Non-parametric tests for trend were also conducted (see online supplemental appendix B).
Co-occurrence of conditions
For 1 July each year, the number of children and young people experiencing gender dysphoria/incongruence with a recorded diagnosis, prescription, symptom or hospital admission indicative of anxiety, depression or self-harm before 1 July in that year or in a preceding year was divided by the mid-year estimate of the total number experiencing gender dysphoria/incongruence. Co-occurrence in matched comparators was similarly estimated.
Prescribing of puberty suppressing hormones and masculinising/feminising hormones
For 1 July each year, the number of children and young people experiencing gender dysphoria/incongruence with a recorded prescription for puberty suppressing, masculinising (androgens/antiestrogens) or feminising (oestrogens/antiandrogens) hormones starting on or after the date of the first record of gender dysphoria/incongruence was divided by the mid-year estimate of the total number experiencing gender dysphoria/incongruence.
Sensitivity analyses
Variations to the definitions set out above were explored (online supplemental appendix C):
For prevalence of gender dysphoria/incongruence, analyses were restricted to first recorded activity within the preceding (a) 3 years and (b) 1 year.
For co-occurring anxiety, depression and self-harm, analyses were (a) restricted to recording within the preceding year; (b) restricted to first recording from 90 days before to any time after the first recording of the index condition; and (c) estimated separately for those with co-occurring autism spectrum conditions and/or eating disorders (for those experiencing gender dysphoria/incongruence).
For medical treatments, analyses were (a) expanded to include prescriptions issued at any time, including prior to first record of gender dysphoria/incongruence; (b) restricted to prescriptions received within the preceding year.
Ethical approval
Permission for data usage was obtained from the CPRD Independent Scientific Advisory Committee (protocol number 22_001967). Linked pseudonymised data were provided by CPRD.
Results
Incidence and prevalence of gender dysphoria/incongruence
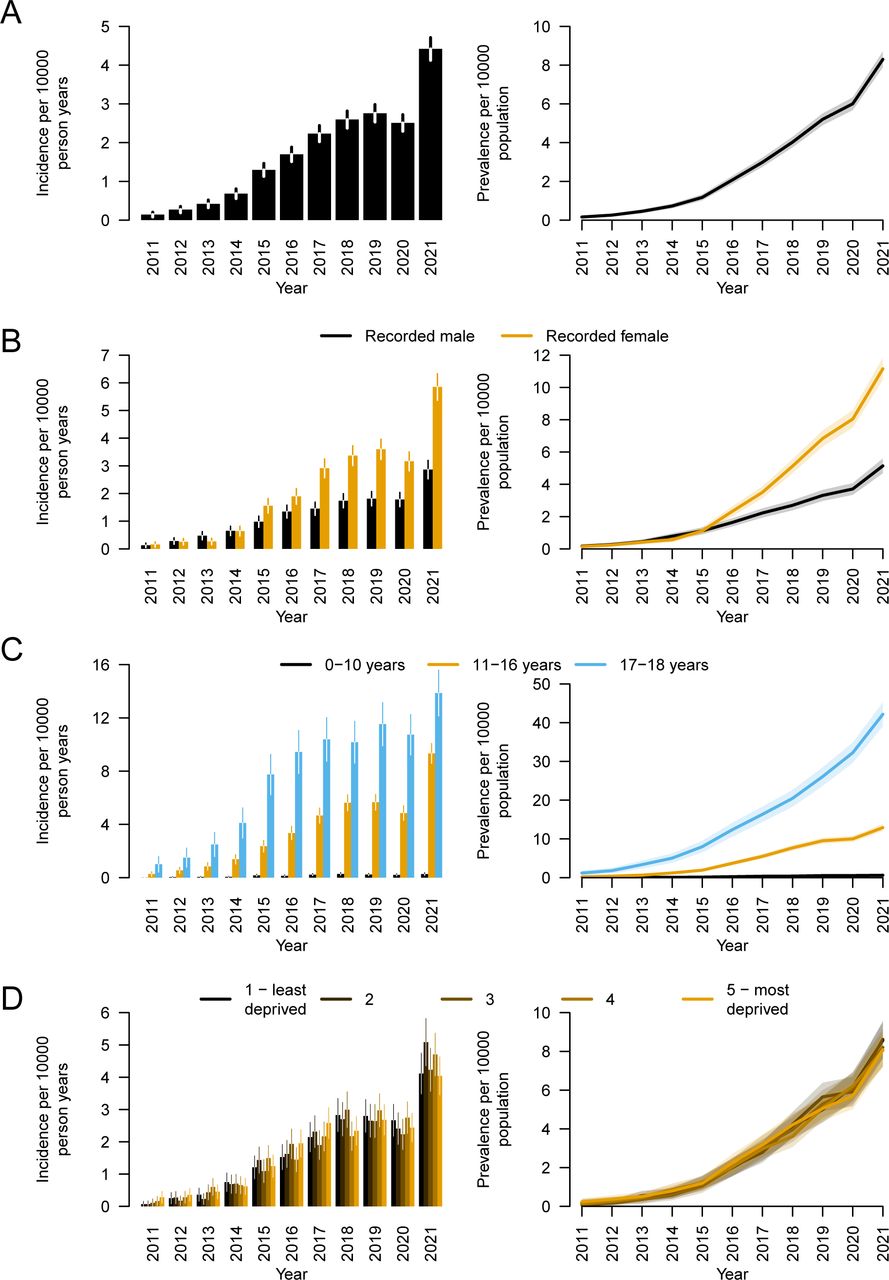
Incidence rates of recorded gender dysphoria for children and young people (age 0–18) increased from 0.14 (95% CI 0.08 to 0.20) per 10 000 person years in 2011 to 4.4 (95% CI 4.1 to 4.7) per 10 000 in 2021. Rates increased significantly every year with the exception of 2020, the first year of the COVID-19 pandemic (online supplemental appendix B). Overall prevalence for children and young people with any recorded history of gender dysphoria/incongruence increased from 0.16 (95% CI 0.10 to 0.23) per 10 000 persons in 2011 to 8.3 (95% CI 7.9 to 8.7) per 10 000 in 2021. In sensitivity analyses, prevalence in 2021 ranged from 3.4 (95% CI 3.1 to 3.6) per 10 000 for those with a record within the last year to 6.6 (95% CI 6.3 to 7.0) per 10 000 for those with a record within the last 3 years (see online supplemental appendix C).
Prevalence of gender dysphoria/incongruence was similar in recorded males and females up to 2015, after which prevalence increased more quickly in recorded females, and was approximately twice as high as in recorded males by 2021 (figure 1B). Incidence of gender dysphoria/incongruence increased with age, being rarely recorded in those under the age of 11 (figure 1C); recorded prevalence was therefore highest in the 17–18 age group (42 (95% CI 39 to 45) per 10 000 in 2021). There was no significant linear association between recorded prevalence and area deprivation at any time (figure 1D; online supplemental appendix D figure A16).

Incidence (left) and mid-year prevalence (right) for gender dysphoria/incongruence in children and young people aged up to 18 years: (A) overall; (B) by most recent gender recorded at primary care practice; (C) by age group; (D) by deprivation category. Vertical lines on incidence rate bars and shaded areas around prevalence lines represent 95% CIs.
Co-occurrence of conditions
Over the whole study period, 1994 of the 3782 children and young people with a record of gender dysphoria/incongruence (52.7%) had a record of anxiety, depression and/or self-harm at some time before reaching the age of 19.
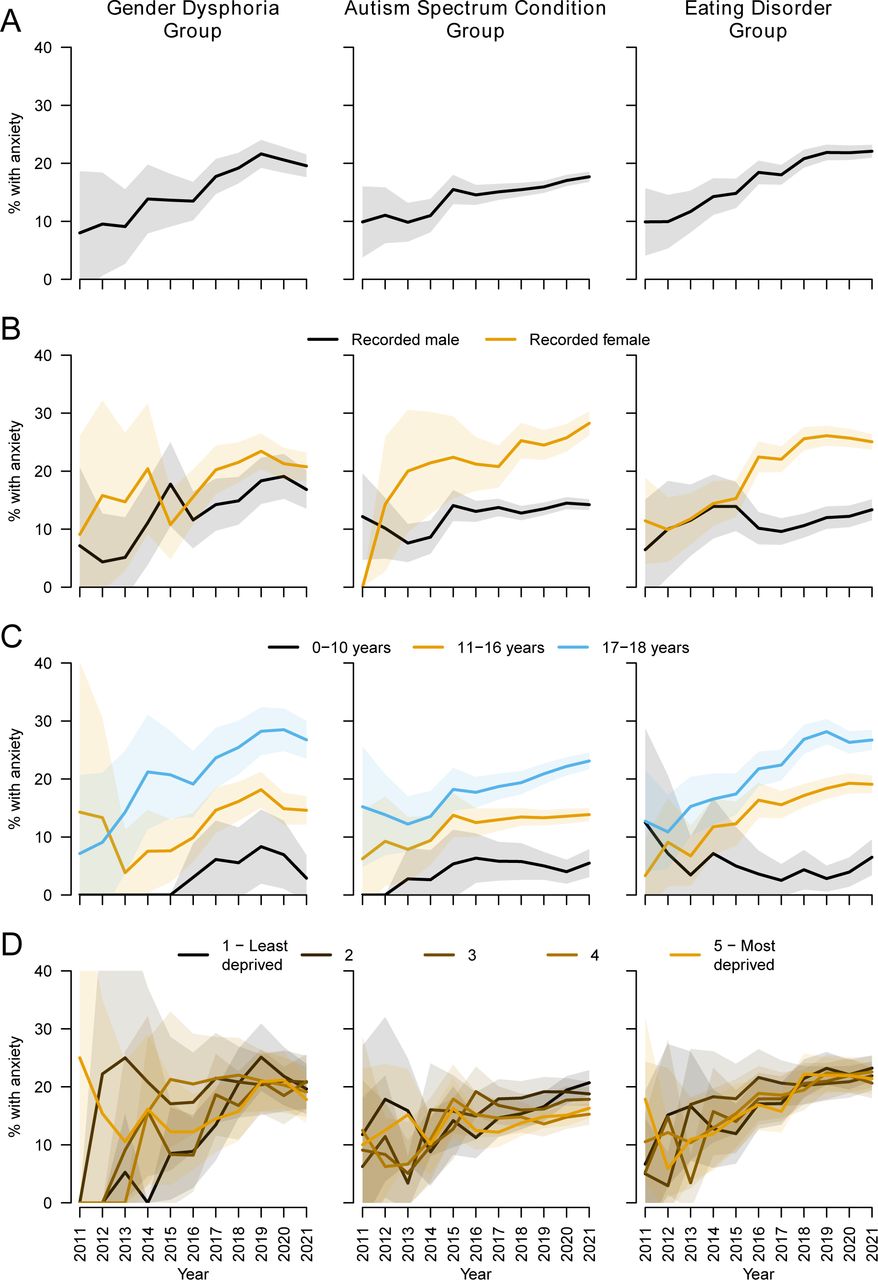
Estimates of rates of co-occurring conditions by year are imprecise before 2015 due to low numbers. Between 2015 and 2021, the proportion of patients with a history of anxiety increased from 13.6% (95% CI 9.1% to 18.2%) to 19.6% (95% CI 17.6% to 21.5%) for patients experiencing gender dysphoria/incongruence compared with 15.5% (95% CI 13.0% to 18.0%) to 17.7% (95% CI 16.8% to 18.6%) for matched comparators with autism spectrum condition and 14.8% (95% CI 12.3% to 17.3%) to 22.1% (95% CI 21.0% to 23.2%) for comparators with eating disorder (figure 2A). Confidence intervals are relatively wide for all three conditions, particularly in earlier years, and increases over time were only statistically significant for eating disorder. For all groups, co-occurring anxiety tended to be more common in recorded females than recorded males (although not significantly so for patients experiencing gender dysphoria/incongruence, figure 2B) and increased in frequency with age (figure 2C). There was no clear association with area deprivation for any group (figure 2D).

Co-occurrence of anxiety among children and young people with (left) gender dysphoria/incongruence; (centre) autism spectrum conditions; (right) eating disorders: (A) overall; (B) by most recent gender recorded at primary care practice; (C) by age group; (D) by deprivation category. Shaded areas represent 95% CIs.
The proportion of children and young people in the gender dysphoria/incongruence group with a history of depression changed little after 2015, reaching 33.7% (95% CI 31.4% to 36.0%) in 2021. In contrast, there were clear increases in the other groups between 2015 and 2021: from 15.0% (95% CI 12.5% to 17.5%) to 18.9% (95% CI 18.0% to 19.7%) for autism spectrum conditions and from 22.6% (95% CI 19.6% to 25.6%) to 29.8% (95% CI 28.6% to 31.0%) for eating disorder (figure 3A). Depression was recorded significantly more frequently in the gender dysphoria/incongruence group in all years, particularly for recorded males. For all groups, depression was more common in recorded females than recorded males (figure 3B), increased in frequency with age (figure 3C), and was not associated with area deprivation (figure 3D).

Co-occurrence of depression among children and young people with (left) gender dysphoria/incongruence; (centre) autism spectrum conditions; (right) eating disorders: (A) overall; (B) by most recent gender recorded at primary care practice; (C) by age group; (D) by deprivation category. Shaded areas represent 95% CIs.
The proportion of children and young people with a history of self-harm did not increase significantly for any group after 2015, reaching 18.5% (95% CI 16.6% to 20.4%) in 2021 for gender dysphoria/incongruence compared with 5.8% (95% CI 5.2% to 6.3%) for autism spectrum conditions and 14.0% (95% CI 13.0% to 14.9%) for eating disorder (figure 4A). Self-harm was recorded significantly more frequently in the gender dysphoria/incongruence group in all years, particularly for recorded males. In all groups, self-harm was more common in recorded females (figure 4B) and increased in frequency with age (figure 4C). There were no consistent deprivation-related patterns (figure 4D).

History of self-harm among children and young people with (left) gender dysphoria/incongruence; (centre) autism spectrum conditions; (right) eating disorders: (A) overall; (B) by most recent gender recorded at primary care practice; (C) by age group; (D) by deprivation category. Shaded areas represent 95% CIs.
The gender dysphoria/incongruence group includes patients who also have autism spectrum conditions and/or eating disorder, hence high rates of anxiety, depression and self-harm may reflect the existence of multiple conditions. For patients experiencing gender dysphoria only, the proportions with a history of anxiety, depression or self-harm in 2021 were 15.9% (95% CI 13.9% to 17.9%, 28.5% (95% CI 26.0% to 31.0%) and 16.5% (95% CI 14.55 to 18.6%), respectively (online supplemental appendix C figure A12).
Prescribing of medical treatments
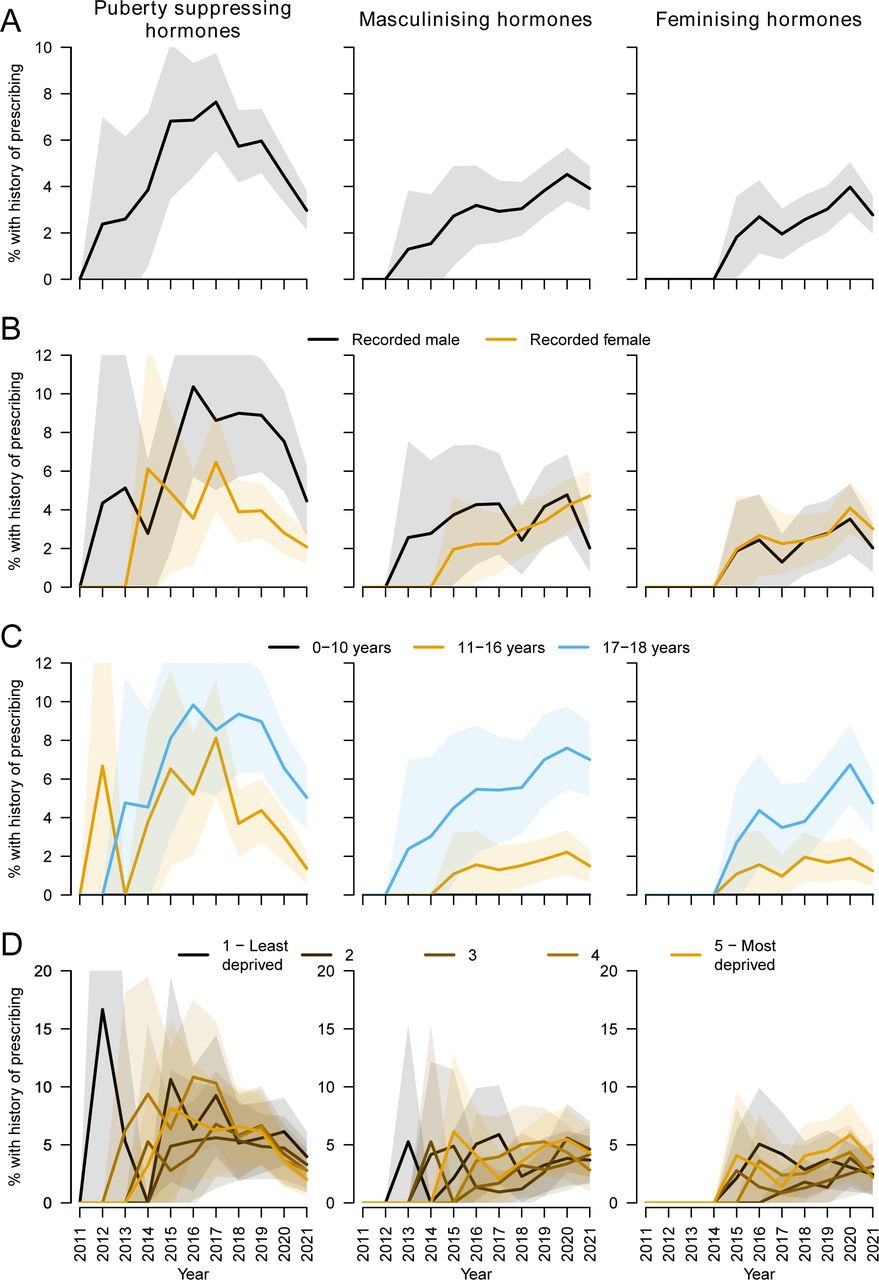
The proportion of children and young people with a record of gender dysphoria/incongruence with a record of a prescription for puberty suppressing hormones increased from 0% in 2011 to 7.6% in 2017 before declining again, reaching 3.0% in 2021 (figure 5A). Prescribing of masculinising hormones increased from 2012, reaching 3.9% in 2021; prescribing of feminising hormones increased from 2014, reaching 2.9% in 2021. Over the whole study period, 176 (4.7%) children and young people with a record of gender dysphoria/incongruence also had a record of a prescription for puberty suppressing hormones and 302 (8.0%) had a record of a prescription for masculinising/feminising hormones. Of those with a record of a prescription for puberty suppressing hormones and at least 2 years of follow-up, 71 (62%) had a record of a prescription for a masculinising or feminising hormone within 5 years (online supplemental appendix C figure A15).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of children and young people with gender dysphoria/incongruence prescribed (left) puberty suppressing hormones; (centre) masculinising hormones; (right) feminising hormones: (A) overall; (B) by most recent gender recorded at primary care practice; (C) by age group; (D) by deprivation category. Shaded areas represent 95% CIs.
Prescribing of puberty suppressing hormones was marginally more frequent for recorded males than recorded females (figure 5B), but patients in receipt of puberty suppressing hormones may be more likely to have changed their recorded gender, making comparisons difficult to interpret, and potentially explaining why recorded males received masculinising hormones and recorded females received feminising hormones. Prescribing of puberty suppressing and masculinising/feminising hormones increased with age (figure 5C). There was no clear association with area deprivation (figure 5D).
Discussion
Between 2011 and 2021, there was a substantial increase in recording of gender dysphoria and/or incongruence among children and young people by general practices contributing to the CPRD Aurum database in England. Recorded incidence rates increased every year with the exception of 2020, when access to primary and secondary care was restricted during the COVID-19 pandemic. The increase was most marked among those recorded as female and for 17 and 18 year olds, and occurred at a similar rate for all levels of area deprivation. By 2021, 8.3 (95% CI 7.9 to 8.7) per 10 000 people aged 18 and under had a history of gender dysphoria/incongruence; if this pattern were repeated nationally, it would equate to 10 291 (95% CI 9795 to 10 787) people aged 18 and under, compared with 192 (95% CI 120 to 276) in 2011—an over 50-fold increase. Levels of anxiety, depression and self-harm were high, particularly for recorded females.
Strengths and weaknesses
We used electronic medical records drawn from a nationally representative sample of general practices carrying complete primary care histories of thousands of people with a record of gender dysphoria/incongruence linked to other health-related datasets. Primary care databases facilitate investigation of rare events and conditions, such as gender dysphoria/incongruence, and minimise selection and information bias as almost all residents in England are registered with a general practitioner and practices collect data prospectively. However, these datasets are reliant on accurate and up-to-date recording of symptoms, diagnoses and clinical activity by practice staff who may be unfamiliar with the conditions and treatments of interest, and who may not have had symptoms or diagnoses—which can be stigmatising—disclosed to them by patients. We therefore conducted several alternative analyses, making different assumptions about the relative timing of conditions.
Our study risks classification errors in relation to patient sex and gender, as practices’ clinical computing systems had one reporting option (gender, reported as male, female or other) and CPRD reports the latest recorded gender category only. This will refer to sex as recorded at birth in most cases, particularly for children and young people, but patients experiencing gender dysphoria/incongruence can ask practices to change their recorded gender without supporting evidence,21 although practices sometimes request this (for example, a change to NHS number following gender reassignment). For prescribing, both puberty suppressors and masculinising/feminising hormones have a range of alternative indications and therefore might not have been prescribed primarily as a treatment for gender dysphoria in every case. The main analysis was restricted to prescriptions issued on or after the first recording of gender dysphoria/incongruence to reduce the risk of including alternative indications for treatment in the analysis. Although practices can document prescriptions issued in secondary care or by private providers in the primary care record, it is possible that treatments will not have been recorded if they were issued elsewhere.22 This, and the inclusion of an unknown number of ineligible patients (who are pre-puberty or post-puberty) in the denominator for our rate calculations, means our prescribing figures are likely to be underestimates.
Key findings and comparison with existing literature
The incidence of gender dysphoria/incongruence in primary care described in this study is consistent with levels and patterns of referrals reported by GIDS, the national centre for gender dysphoria in children and adolescents, over the same period. Referrals to GIDS increased from around 100 annually in 2010 to over 2500 in 2019, after which referrals fell during the COVID-19 pandemic.23 24 An audit of attenders at GIDS between 2018 to 2022 found that most had been referred by Child and Adolescent Mental Health Services (CAMHS), with 41% directly referred by general practices.25 Our results suggest that practices are likely to be aware of cases referred by other services, and general practices commonly referred to GIDS via CAMHS during the 2010s.
Recent increases in incidence of gender dysphoria/incongruence have a range of potential explanations, including social factors (for example, changes in public attitudes towards gender differences, greater awareness and acceptance of gender dysphoria/incongruence, increasing use of social media and networking); increasing rates of emotional distress and poor mental health in this age group, particularly for females26 ; and changes in supply and delivery of healthcare (for example, changes to clinical guidelines and practices, and increased availability of advice and treatments both in person and online).27 As we did not directly explore these factors, we cannot comment on their explanatory power but heightened public awareness may have affected presentations to primary care and case finding by practices. Recording behaviour by practices may also have changed in response to updates to clinical coding systems and guidelines, although we used a broad range of diagnostic terms and related clinical presentations in our analysis to account for changes in diagnostic behaviour (see online supplemental appendix A).
International studies report high levels of anxiety (31–46%), depression (31–45%) and self-harm (8–41%) in children with gender dysphoria/incongruence attending paediatric specialist services.14 In our study, overall recorded levels in primary care were at the lower end of these estimates, with rates of anxiety similar to, and rates of depression and self-harm higher than, matched comparators with autism spectrum conditions or eating disorder in most years (these higher rates are partly explained by elevated risk in children with multiple conditions—see online supplemental appendix C). Note that the overall rates of mental health conditions in the three study groups are affected by the respective ratios of males to females, which vary substantially (table 1). The greatest differences between the groups were for recorded males; rates of depression and self-harm were substantially higher for male children and young people experiencing gender dysphoria compared with males in the other two groups. The Mental Health and Young People Survey in England, which relies on self and parental report, found that 17.4% of 17–19 year olds had a ‘probable’ mental health disorder—including problems with emotions, behaviours or relationships—at the time of the survey in 2021.28 In 2021 in our study, 55% of 17–18 year olds experiencing gender dysphoria/incongruence and 73% experiencing both gender dysphoria/incongruence and an autism spectrum condition had a documented history of anxiety, depression or self-harm (see online supplemental appendix C).
Our finding of a lack of an association between gender dysphoria/incongruence and area deprivation contrasts with McKechnie et al, who reported rates for patients living in the most deprived fifth of areas over twice as high as for patients in the least deprived.15 McKechnie et al analysed transgender identity and measured deprivation using the Townsend Deprivation Score, which classifies areas differently to the IMD, but the indices are strongly correlated29 and are unlikely to produce substantially different results when populations are aggregated into quintiles (note that neither index measures socioeconomic characteristics at the individual level). However, McKechnie et al assessed all age groups, hence their results are dominated by adults, who are more likely to present directly to healthcare providers without mediation by parents/carers, and for whom socioeconomic variations in health are often more pronounced than for adolescent populations.30 31 The discrepancy in our results may therefore be the result of different characteristics in different age groups, ascertainment bias (higher rates of presentation and diagnosis for more affluent groups offsetting higher underlying prevalence in more deprived groups), and/or net downwards socioeconomic migration in adults experiencing gender dysphoria/incongruence over the lifecourse due to increased risk of unemployment and low income in adulthood.32
With respect to medical treatment, an audit of GIDS clinical pathways reported that 27% of attenders were referred to endocrinologists, of whom 55% were treated with both puberty suppressing hormones and masculinising/feminising hormones and 20% were treated with puberty suppressing hormones only.25 These rates of medical treatment are higher than those recorded by general practices in our study, which may reflect long waiting times to access specialist services that initiate treatment, reluctance by general practitioners to prescribe off-label, or practices not always recording treatments prescribed elsewhere. Prescribing rates for puberty suppressing hormones fell in our sample after 2017, when prevalence of gender dysphoria/incongruence was increasing fastest for 17–18 year olds (who are more likely to have completed puberty and less likely to be prescribed puberty suppressing hormones—see online supplemental appendix C figure A15) and when annual referrals into GIDS started to exceed 2000, resulting in longer waiting times to access the service and subsequent endocrinology assessment. Assessment and prescribing in 2020 and 2021 are likely to have been further affected by the COVID-19 pandemic and the ongoing Bell v Tavistock case,33 which examined the competence of under-16s to consent to treatment with puberty suppressing hormones.
Conclusions
The NHS in England is implementing a series of reforms in response to the Cass Review into gender identity services for children and young people,34 including introducing new service models and collaborative care arrangements.35 Our study provides information on trends in recording of gender dysphoria/incongruence and common co-occurring conditions in primary care, and can help to inform the development of local and national services. These developments should include appropriate support and guidance for primary care services, which will frequently be the first point of contact and will be responsible for coordinating care, often in the context of lengthy waits for specialist assessment. Local support networks will need to be robust as, despite the rapid increase in recorded prevalence over the last decade, gender dysphoria/incongruence remains uncommon under the age of 19 and direct clinical experience for most general practice staff is likely to remain limited.
Levels of observed anxiety and depression have been increasing in children and young people in general over the last two decades for complex and contested reasons,36 37 challenging health, education and social services,38–40 and those experiencing gender dysphoria/incongruence are at particular risk. Future research should address the aetiology, pathways to diagnosis and interactions of these conditions, and explore other mental health issues and adverse social circumstances not examined in this study. Our findings highlight the need to provide comprehensive assessments, which should include screening for co-occurring conditions, of children and young people experiencing gender dysphoria/incongruence when they present to primary care, and where appropriate, for effective, coordinated interventions, supported by timely secondary and tertiary care, to address their wider mental health needs.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data were derived from the Clinical Practice Research Datalink (CPRD) Aurum primary care dataset (https://www.cprd.com/).
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
For helpful comments we would like to thank Karen Bloor, Katherine Checkland, Richard Cookson, Stephanie Lamb, Kate Pickett, David Taylor Robinson and Roger Webb. Any errors or opinions expressed in this publication are those of the authors and not those of any individuals who provided comment.
References
Footnotes
X @swjarvis, @lornafraser10
Correction notice The second author's affiliation has been updated since this paper was first published.
Contributors SWJ, LKF and CEH contributed to the idea generation and protocol development. SWJ and TD prepared the data for analysis, and SWJ performed the statistical analyses. SWJ, LKF, TL, CEH and TD interpreted the study results. TD and SWJ had primary responsibility for writing the manuscript. LKF, TL and CEH also contributed to manuscript writing. All authors critically reviewed the manuscript and have approved the final article. SWJ and TD are responsible for the overall content as guarantors.
Funding The study was commissioned and funded by NHS England to inform the Cass Review into gender identity services for children and young people (https://cass.independent-review.uk/home/publications/final-report/). The research was independent, and neither the funder nor the Cass Review team were involved in the conduct of the study or interpretation of the results.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.