Article Text

Abstract
Background White blood cell count (WBC) is a widely used marker for the prediction of serious bacterial infection (SBI); however, previous research has shown poor performance. This study aims to assess the value of WBC in the prediction of SBI in children at the emergency department (ED) and compare its value with C reactive protein (CRP) and absolute neutrophil count (ANC).
Methods This study is an observational multicentre study including febrile children aged 0–18 years attending 1 of 12 EDs in 8 European countries. The association between WBC and SBI was assessed by multivariable logistic regression, adjusting for age, CRP and duration of fever. Additionally, diagnostic performance was assessed by sensitivity and specificity. Results were compared with CRP and ANC.
Results We included 17 082 children with WBC measurements, of which 1854 (10.9%) had an SBI. WBC >15 had an adjusted OR of 1.9 (95% CI 1.7 to 2.1) for prediction of SBI, after adjusting for confounders. Sensitivity and specificity were 0.56 (95% CI 0.54 to 0.58) and 0.74 (0.73 to 0.75) for WBC >15, and 0.32 (0.30 to 0.34) and 0.91 (0.91 to 0.91) for WBC >20, respectively. In comparison, CRP >20 mg/L had a sensitivity of 0.87 (95% CI 0.85 to 0.88) and a specificity of 0.59 (0.58 to 059). For CRP >80 mg/L, the sensitivity was 0.55 (95% CI 0.52 to 057) and the specificity was 0.91 (0.90 to 0.91). Additionally, for ANC >10, the sensitivity was 0.55 (95% CI 0.53 to 0.58) and the specificity was 0.75 (0.75 to 0.76). The combination of WBC and CRP did not improve performance compared with CRP alone.
Conclusion WBC does not have diagnostic benefit in identifying children with an SBI compared with CRP and should only be measured for specific indications.
- epidemiology
- paediatric emergency medicine
- infectious disease medicine
- paediatrics
Data availability statement
Data are available on reasonable request. Data of this study are available on request from the corresponding author (j.zachariasse@erasmusmc.nl), subject to local rules and regulations.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous systematic reviews have shown poor performance of white blood cell count (WBC) for the prediction of serious bacterial infections (SBI) in febrile children.
The individual studies included in these reviews were single centre, only included a small number of patients and mostly focused on younger children.
WHAT THIS STUDY ADDS
In the febrile paediatric emergency department population, WBC is a significant predictor for SBI.
C reactive protein (CRP) outperforms WBC, and WBC adds little to the performance of CRP in the prediction of SBI.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
WBC does not bring diagnostic benefit identifying children with SBI compared with CRP and should only be performed for specific indications.
Introduction
The initial assessment of febrile children in the emergency department (ED) often includes laboratory markers in addition to history and a physical examination to assess the severity of illness and the risk of a serious bacterial infection (SBI). White blood cell count (WBC) is widely used in the initial assessment of febrile children. It increases as a response to an acute or chronic inflammatory stressor with a maximum 12 hours after onset of symptoms.1 WBC is a relatively simple and fast marker that can be evaluated through a routine blood draw and is included in several international guidelines and decision rules, such as the Goldstein sepsis criteria and the National Institute for Health and Care Excellence guidelines, for the evaluation of febrile children to guide further diagnostics and treatment.2–5 However, previous systematic reviews have shown poor performance of WBC in children.4 6
The continued use of WBC count might be explained by limitations in the current evidence. Existing research is mostly based on children under 5 years of age and does not assess the benefit of WBC to other inflammatory markers, such as C reactive protein (CRP) or absolute neutrophil count (ANC). In addition, diagnostic studies on WBC performance have shown highly variable results.6–8 These studies included a maximum of 500 children and were mostly performed in a single centre.9 10 Therefore, there is a need for a large, multicentre study, assessing the predictive value of WBC, especially in all ages.
The aim of our study was to determine the diagnostic value of WBC for the prediction of SBI in febrile children, compare this with the performance of CRP and ANC and to assess the diagnostic value of WBC in combination with CRP. In addition, we aimed to assess whether high WBC count is associated with specific pathogens.
Methods
This study is a secondary analysis of the Management and Outcome of Fever in children in Europe (MOFICHE) study, which is part of the Personalised Risk assessment in Febrile illness to Optimise Real-life Management across the European Union project.11 12 The MOFICHE study is an observational multicentre study evaluating the management and outcome of febrile children attending the ED and included children aged 0–18 years with fever (≥38.0°C) or a history of fever (within 72 hours before ED visits). This study was performed in 12 EDs in 8 countries: Austria, Germany, Greece, Latvia, the Netherlands (n=3), Spain, Slovenia and the UK (n=3). Characteristics of the participating hospitals were described in a previous study.13 For this study, we included all children with a WBC measurement.
Data collection
The study period was between January 2017 and April 2018, with each centre collecting at least 12 months data. Data for the study consisted of routine clinical data and were extracted from electronic health records by local research teams. The data collected includes patient characteristics, diagnostics and treatment. Focus of infection and cause of infection were retrospectively assigned by the research teams. Focus of infection was categorised into upper respiratory tract infection/ear, nose, throat infection, lower respiratory tract infection, gastrointestinal/surgical abdomen, urinary tract infection, childhood exanthems/influenza-like illness, soft tissue or skin/musculoskeletal, sepsis/meningitis and other (eg, undifferentiated fever and inflammatory illness). The levels of CRP, WBC and ANC were measured, and microbiological cultures were collected at the ED according to routine clinical practice. We analysed these markers continuously as well as with use of the following cut-off points. For WBC. we defined ‘normal’ as a value between 5×109/L and 15×109/L and abnormal as a value below 5×109/L or above 15×109/L. Furthermore, we included the cut-off points 20×109/L, 25×109/L and 30×109/L. For CRP, we defined three commonly used cut-off points: 20 mg/L, 60 mg/L and 80 mg/L. For ANC, cut-off points of 10×109/L, 15×109/L and 20×109/L were used to distinguish normal/low and high values. These cut-off points are mostly used in international guidelines and decision rules.2 3
Outcome measure
The primary outcome measure we used was SBI. SBI was defined as a ‘definite’ or ‘probable’ bacterial infection with a focus of infection in the gastrointestinal tract, lower respiratory tract, urinary tract, musculoskeletal tract, central nervous system or sepsis. This outcome measure was used previously for several other studies within MOFICHE.14–16 The cause of infection was determined using a previously published phenotyping algorithm, which combines clinical symptoms and diagnostic results.12 14 15 Definite bacterial was defined as a positive culture from a sterile site, matching the identified bacterial syndrome. Probable bacterial was defined as a bacterial syndrome with no bacteria identified, with a CRP measurement >60 mg/L.16 As secondary outcome measure, we used only infections with a positive bacterial culture, labelled definite bacterial infections in the phenotyping algorithm.
Statistical analysis
In a descriptive analysis, the baseline characteristics of all the children and the baseline characteristics of the children with a WBC measurement were explored. Univariable and multivariable logistic regression model were used to calculate the association between WBC and SBI. We included WBC as a continuous marker as well as using the predefined cut-off points. We considered age (continuously), CRP (continuously in mg/L), duration of fever (categories <24 hours, 24–48 hours and >48 hours) and ANC (continuously) as important confounders. In the first model, we adjusted only for age (model 1). In the second model, we adjusted for both age and CRP (model 2). In the third model, we adjusted for age, CRP and duration of fever (model 3). In the last model (model 4), we adjusted for either WBC or ANC depending on the predictor used. Additionally, we looked at the association between ANC and SBI. Furthermore, the diagnostic performance of WBC was evaluated with sensitivity, specificity, negative predictive value, positive predictive value, negative likelihood ratio (LR) and positive LR. This was compared with the diagnostic performance of CRP. As an overall measure of performance, we also calculated the area under the curve (AUC) for these markers. Missing values for all confounders were imputed using the MICE package in R. Because CRP was used in the categorisation of the presumed cause of infection, we conducted sensitivity analyses with different outcome measures to assess the robustness of our findings. First, we used all suspected bacterial infections, regardless of CRP value, as the outcome, defined as a definite bacterial infection, a probable bacterial infection or a bacterial syndrome in the original phenotyping algorithm (online supplemental appendix 1). Finally, we assessed if different viral and bacterial pathogens were associated with different levels of WBC. We described and plotted WBC levels (median and IQR) for different viral (influenza, respiratory syncytial virus or other) and bacterial pathogens (any pathogen found more than three times in the study population) and compared these with levels in children with negative viral and bacterial diagnostic tests. All analyses were performed using R V.4.2.1.17
Supplemental material
Results
Baseline characteristics
A total of 38 480 children were included, of which 17 082 had a WBC measurement at the ED. Patient characteristics are described in table 1. The children with a WBC measurement were overall more ill, which is shown by the higher triage urgency level, higher referral rate, more ill appearance and higher admission rate. In the subgroup of children with a WBC measurement, the most common focus of infection was upper respiratory tract infections (42.6%), followed by lower respiratory tract infections (17.3%). In children with a WBC measurement, 1854 (10.9%) were diagnosed with an SBI. CRP was measured in 17 213 children of the total population.
Baseline characteristics of the study population (n=38 480)
Association between WBC and SBI
In a univariable regression model, there was a significant association between WBC >15×109/L and SBI with an OR of 3.5 (95% CI 3.2 to 3.9). After adjusting for age, CRP and duration of fever, the adjusted OR (aOR) remained significant and was 1.9 (95% CI 1.7 to 2.1) (table 2). In a subsequent analysis where ANC was added as a confounder, the aOR for WBC >15×109/L remained significant (aOR 1.4, 95% CI 1.2 to 1.6). WBC <5×109/L did not have a significant association with SBI after adjusting for the confounders (aOR 1.1, 95% CI 0.8 to 1.5). The association between ANC and SBI was comparable (online supplemental appendix 2). The secondary outcome measure, only including culture-proven bacterial infections, resulted in an aOR for WBC >15×109/L of 1.9 (95% CI 1.6 to 2.3) (online supplemental appendix 3).
Association between white blood cell count and serious bacterial infection
Diagnostic performance
In table 3, the diagnostic performance in predicting SBI of WBC, ANC and CRP is described. WBC with a cut-off point of >15×109/L showed a sensitivity of 0.56 (95% CI 0.54 to 0.58) and a specificity of 0.74 (95% CI 0.73 to 0.75). ANC had a comparable accuracy. When assessing higher cut-off points of WBC and ANC, the specificity increased at the cost of a lower sensitivity. When comparing the performance of WBC with CRP, CRP with a cut-off point of >20 mg/L had a better sensitivity but a poorer specificity. Using the cut-off points of CRP >60 and >80 mg/L showed similar to improved sensitivity and specificity compared with WBC. Adding abnormal CRP to WBC improved specificity at the cost of a substantial reduction in sensitivity. Regardless of the cut-off for CRP used, this did not improve overall performance. We also assessed if WBC could be of added value to the group where CRP has a value between 20 and 60 mg/L. This resulted in a sensitivity of 0.77 (95% CI 0.75 to 0.79) and a specificity of 0.77 (95% CI 0.76 to 0.78), and thus only a slight increase in sensitivity at the cost of a substantial decrease in specificity. The diagnostic performance of the secondary outcome measure showed a small decrease in sensitivity and specificity across all the markers and cut-off points (online supplemental appendix 3).
Diagnostic performance of the inflammatory markers
Combining these results in an overall measure of performance, WBC had an AUC of 0.71 (95% CI 0.70 to 0.72). In comparison, CRP had an AUC of 0.84 (95% CI 0.83 to 0.85) and ANC had an AUC of 0.71 (95% CI 0.70 to 0.73).
Sensitivity analyses
In the sensitivity analysis using the broad outcome of all suspected bacterial infections regardless of CRP level, the aOR of WBC remained significant (aOR 1.8 (95% CI 1.6 to 2.0)) (online supplemental appendix 4). Sensitivity decreased in all markers, including CRP, while specificity remained comparable.
Viral and bacterial pathogens
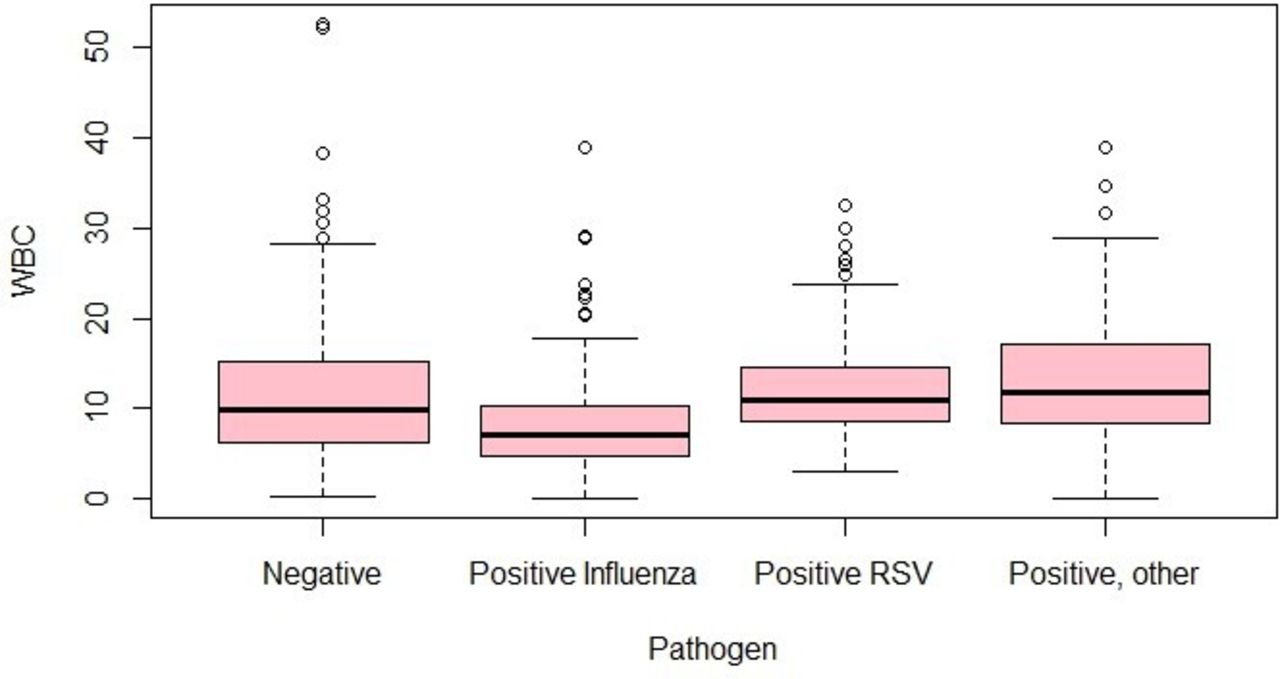
In the viral infections, median WBC value was lowest for influenza (median 7.0, IQR 4.7–10.3), even when compared with children with a negative viral test (median 10.2, IQR 6.2–15.2) (figure 1). Bacterial pathogens had higher WBC counts in general, although notable differences across the different pathogens existed. WBC values were highest in infections with Streptococcus pneumoniae (median 18.3, IQR 9.0–33.5), Neisseria meningitidis (median 17.0, IQR 8.8–24.5), Streptococcus pyogenes (median 14.3, IQR 12.9–16.5) and Haemophilus influenzae (median 14.1, IQR 5.0–27.9) (figure 2).

Levels of white blood cell count for bacterial pathogens (median, IQR). CNS, coagulase-negative staphylococcus (n=23); EC, Escherichia coli (n=20); GBS, group B streptococcus (n=6); HI, Haemophilus influenzae (n=4);NM, Neisseria meningitidis (n=5); SPn, Streptococcus pneumoniae (n=27); SA, Staphylococcus aureus (n=25); Sa, Salmonella species (n=5); SP, Streptococcus pyogenes (n=5); SV, Streptococcus viridans (n=4); WBC, white blood cell count.

{kind=link}
{kind=link}
Levels of white blood cell count (WBC) for viral pathogens (median, IQR). Negative=negative for any viral pathogen (n=897); positive influenza (n=381); positive respiratory syncytial virus (RSV, n=266); positive, other=positive for any other respiratory viral pathogen than influenza or RSV (n=415).
Discussion
This observational study shows that WBC is significantly associated with SBI, even after adjusting for CRP, but that its sensitivity and specificity is only moderate. These results also demonstrate that when CRP is used, WBC adds little to the performance in predicting SBI. ANC shows similar results as WBC and does not outperform its performance. These results are in line with earlier research on this topic, and assessed the added value of WBC to CRP. Previous systematic reviews showed a poor to moderate ‘rule-in’ and ‘rule-out’ value for WBC, which is consistent with the results of this study.4 6 Individual studies included in these reviews were often small and single-centre and mostly focused on children under 36 months of age, with limited evidence in older children and adolescents. Our study adds to the existing literature, because we included a large multicentre cohort of children until the age of 18 years.
An important strength of this study is its multicentre nature and the inclusion of >17 082 children from 12 EDs in 8 countries. The population is broad, includes all ages and all causes of fever, regardless of severity or underlying cause, making the results generalisable to the febrile paediatric ED population. In addition, due to our large cohort, we were able to assess the relatively rare outcome of SBI. Furthermore, a strength of this study is the careful data curation, with manual data collection and extensive data monitoring and data quality checking processes in place, resulting in a complete and accurate database.12
One of the limitations is the outcome measure. Our primary outcome measure, definite or probable bacterial infection, was determined using a phenotyping algorithm based on clinical diagnosis/presentations and includes CRP as one of the parameters. This could potentially influence the results of the analyses related to CRP. Since the primary focus of this article was WBC, which was not a part of this outcome measure, and because the outcome was determined through multiple steps in a well-established and validated phenotyping algorithm, we did not consider this a major bias.12 A secondary outcome measure, only including definite bacterial infections, showed comparable results and provided further support for our results. In addition, we did a sensitivity analysis using a broader outcome measure including all suspected bacterial infections independent from the CRP value. In this sensitivity analysis, CRP remained again a better marker in comparison with WBC and ANC. Another limitation of this study was that WBC was not measured in all children attending the ED. This results in a risk of selection bias and could have influenced our results. We observed that WBC was not measured in the children who were least ill, which represents normal clinical practice in an ED, where WBC is mainly measured in sicker children or in cases where the diagnosis remains uncertain. Therefore, we believe our results are a good representation of the real-world value of WBC in clinical practice. The same holds for CRP for which a similar percentage was missing. Furthermore, due to the limited amount of individual bacterial pathogens, we were not able to analyse these results further than the descriptive analyses. The last limitation is that these data were collected in 2017 and 2018, which only includes a prepandemic period. The pandemic has shown changes in infectious disease in children and could influence the value of WBC. However, we do not expect these changes to have significantly changed the association between WBC and SBI.
Implications for clinical practice and future research
In the ED, doctors use diagnostic markers to deal with diagnostic uncertainty in febrile children. A diagnostic marker in these settings should be relatively fast and have a good rule-in or rule-out value for SBI. We have shown that CRP outperforms WBC in rule-in and rule-out value. Furthermore, adding WBC to CRP adds little to the predictive performance of CRP alone. In practice, WBC does not have diagnostic benefit in identifying children with an SBI and should only be measured for specific indications or if CRP is not available. In addition, CRP appears to be the preferred biomarker for clinical prediction models related to febrile children. It will be an interesting topic for future studies to assess the change in performance when CRP instead of WBC is added to existing prediction rules. Importantly, our research illustrates that WBC and CRP are still not sufficient as markers to effectively rule-in and rule-out SBI. Therefore, research on new biomarkers to recognise children at risk for an SBI is still needed.
Data availability statement
Data are available on reasonable request. Data of this study are available on request from the corresponding author (j.zachariasse@erasmusmc.nl), subject to local rules and regulations.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by all the participating hospitals: Austria (Ethikkommission Medizinische Universitat Graz, ID: 28-518 ex 15/16), Germany (Ethikkommission Bei Der LMU München, ID: 699-16), Greece (Ethics Committee, ID: 9683/18.07.2016), Latvia (Centrala medicinas etikas komiteja, ID: 14.07.201 6. No. Il 16-07-14), Slovenia (Republic of Slovenia National Medical Ethics Committee, ID: 0120-483/2016-3), Spain (Comité Autonómico de Ética de la Investigación de Galicia, ID: 2016/331), The Netherlands (Commissie Mensgebonden onderzoek, ID: NL58103.091.16), UK (Ethics Committee, ID: 16/LO/1684, IRAS application no. 209035, Confidentiality advisory group reference: 16/CAG/0136). No informed consent was needed for this study. In all the participating UK settings, an additional opt-out mechanism was in place.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @CarrolEnitan, @BennoKohlmaier, @ejlim8, @rgnijman
Contributors All authors contributed to the conception and design of the study and the interpretation of the findings. NK performed the analyses and wrote the first draft of the manuscript. CV, CDT and HAM provided insights on data analysis and oversaw the writing of the paper. UvB, EC, ME, MvdF, JAH, BK, ML, EL, IM, FM-T, RGN, MP, IR-C, AR, MT, DZ and WZ provided clinical contributions and insight on data collection. All authors commented on previous versions of the manuscript, and read and approved the final manuscript. JMZ accepts full responsibility for the finished work and the conduct of the study, had access to the data and controlled the decision to publish as the guarantor.
Funding This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement no. 848196. The research was supported by the National Institute for Health Research Biomedical Research Centres at Imperial College London, Newcastle Hospitals NHS Foundation Trust and Newcastle University.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. For the remaining authors, no sources of funding were declared.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.