Case history
Case history #1
A 45-year-old southern Chinese man, former smoker with no other significant past medical history, presents with an enlarging right neck mass of 2-month duration. He has no first-degree relatives with a history of any malignancies. Nasopharyngoscopy reveals subtle mucosal irregularity in the right fossa of Rosenmüller. His Eastern Cooperative Oncology Group (ECOG) performance status is 0. Cranial nerve examination does not reveal diplopia or facial numbness. On neck examination an enlarged, non-tender lymph node is noted in the right level 2 region. Endoscopic-guided biopsy of the right nasopharynx is consistent with a non-keratinising, Epstein-Barr virus (EBV)-positive, nasopharyngeal cancer (NPC). MRI shows right nasopharyngeal mucosal thickening without parapharyngeal extension and a 5 cm right level 2 lymph node. There is no skull base or perineural tumour spread. Positron emission tomography/computed tomography shows an 18F-fluorodeoxyglucose-avid bilateral retropharyngeal and right level 2 lymph node metastases. A plasma EBV DNA level is 10,000 copies/mL.
Case history #2
A 50-year-old woman from Alaska with no significant past medical history presents with 2 months of worsening headaches, nasal congestion, and epistaxis. Her father was diagnosed with NPC at age 60 years. Nasopharyngoscopy reveals a friable tumour centred in the left fossa of Rosenmüller and extending across the midline of the posterior nasopharyngeal wall towards the right nasopharynx. Her ECOG performance status is 0. Cranial nerve examination does not reveal diplopia or facial numbness. Neck examination does not reveal any enlarged cervical lymph nodes. Endoscopic-guided biopsy of the left nasopharynx is consistent with a non-keratinising, EBV-positive, NPC. MRI shows a mass centred in the left nasopharynx invading the sphenoid sinus and clivus. There is no perineural tumour spread. PET/CT shows a FDG-avid left retropharyngeal node and no evidence of distant metastatic disease. A plasma EBV DNA level was measured to be 4000 copies/mL.
Other presentations
An asymptomatic neck mass and nasal symptoms (discharge, bleeding, and obstruction) are the two most common first presentations of NPC (seen in 37% and 35% of patients as a first symptom, respectively).[4] Larger NPC tumours can cause Eustachian tube dysfunction and can present as aural symptoms that include unilateral otitis media with effusion, tinnitus, and hearing impairment in one ear (in 19% of patients as the first symptoms). Other symptoms are rarely the presenting symptom of NPC and usually accompany at least one of the previously mentioned symptoms. Nasopharyngeal tumours with perineural tumour spread may present as cranial nerve palsies, most commonly involving the fifth and sixth cranial nerves and manifest as headaches, facial numbness, and diplopia. Furthermore, larger nasopharyngeal tumours extending to the pterygoid muscles may present as trismus. Among people with NPC who present with neck masses, lymphadenopathy in level II is the most common location, which is similar to other head and neck mucosal squamous cell carcinomas.[5][6] However, level V lymphadenopathy in the posterior cervical triangle is also relatively common in NPC, and this pattern of lymph node spread distinguishes NPC from many other head and neck cancers.
[Figure caption and citation for the preceding image starts]: Lymph node groups in the head and neck; the numbers refer to the anatomical levels of the lymph nodesCancer Research UK [Citation ends].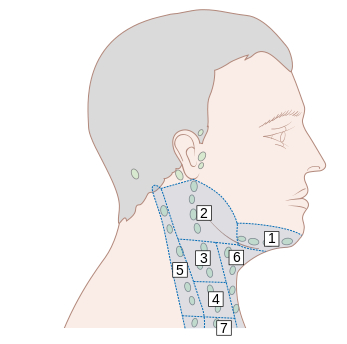
Use of this content is subject to our disclaimer