Article Text

Abstract
Context Readmission to hospital for heart failure is common after recent discharge. Remote monitoring (RM) strategies have the potential to deliver specialised care and management and may be one way to meet the growing needs of the heart failure population.
Objective To determine whether RM strategies improve outcomes for adults who have been recently discharged (<28 days) following an unplanned admission due to heart failure.
Study design Systematic review and network meta-analysis.
Data sources Fourteen electronic databases (including MEDLINE, EMBASE and PsycINFO) were searched to January 2012, and supplemented by hand-searching relevant articles.
Study selection All randomised-controlled trials (RCTs) or observational cohort studies with a contemporaneous control group were included. RM interventions included home telemonitoring (TM) (including implanted monitoring devices) with medical support provided during office hours or 24/7 and structured telephone support (STS) programmes delivered via human-to-human contact (HH) or human-to-machine interface (HM).
Data Extraction Data were extracted and validity was assessed independently by two reviewers.
Results Twenty-one RCTs that enrolled 6317 patients were identified (11 studies evaluated STS (10 of which were HH, while 1 was HM), 9 studies assessed TM, and 1 study assessed both STS and TM). No trial of implanted monitoring devices met the inclusion criteria. Compared with usual care, although not reaching statitistical significance, RM trended to reduce all-cause mortality for STS HH (HR: 0.77, 95% credible interval (CrI): 0.55, 1.08), TM during office hours (HR: 0.76, 95% CrI: 0.49, 1.18) and TM24/7 (HR: 0.49, 95% CrI: 0.20, 1.18). Exclusion of one trial that provided better-than-usual support to the control group rendered each of the above comparisons statistically significant. No beneficial effect on mortality was observed with STS HM. Reductions were also observed in all-cause hospitalisations for TM interventions but not for STS interventions. Care packages generally improved health-related quality-of-life and were acceptable to patients.
Conclusions STS HH and TM with medical support provided during office hours showed beneficial trends, particularly in reducing all-cause mortality for recently discharged patients with heart failure. Where ‘usual’ care is less good, the impact of RM is likely to be greater.
- HEART FAILURE
- EBM
Statistics from Altmetric.com
Introduction
Heart failure (HF) is a major and increasing public health problem worldwide. HF is associated with increased levels of morbidity, mortality and reduced quality-of-life (QoL), particularly among patients aged over 60 years.1 HF imposes an increasingly heavy burden on healthcare systems, most of which can be attributed to repeated hospital admissions.2 The highest risk period for rehospitalisation is the first few weeks after discharge,3 with up to 24% of patients being readmitted within 12 weeks.4 Although multidisciplinary HF disease management programmes decrease hospitalisation rates and improve clinical outcomes,5–8 access may be limited by geographical or funding-related barriers.9 ,10
Early patient remote monitoring (RM) may be one way to meet the growing needs of the HF population. RM approaches include structured telephone support (STS) and home telemonitoring (TM). STS may be delivered via human-to-human contact (HH) or human-to-machine (HM) (interactive response system) interface; while TM may involve remote patient-initiated transfer of physiological data, and/or automatic data transfer from cardiovascular implanted monitoring devices. Two recent systematic reviews and meta-analyses suggested that HF-care packages, which include a RM component, have beneficial effects on mortality and hospitalisation.11 ,12 However, since the publication of these reviews, several new RM studies have become available, including some showing a lack of clinical benefit.13–15 Conversely, the initial findings from the UK Whole Systems Demonstrator trial, which included over 3000 patients, found significant clinical benefits of RM for various conditions including HF.16
With increasing pressure on acute hospital beds from HF, strategies to facilitate early discharge and reduce unplanned readmissions are paramount to improve patient outcomes and resource use. This review updates two existing reviews11 ,12 and determines whether home TM or STS strategies improve outcomes for adult patients who have been recently discharged from hospital after acute HF exacerbation.
Methods
Data sources and searches
Fourteen electronic databases including MEDLINE, EMBASE and PsycINFO were searched. The search strategy used free text and thesaurus terms and combined HF-related synonyms with terms for RM (see online supplementary table S1). No language restrictions were used. However, as the current review updated two previous systematic reviews,11 ,12 searches were limited by date from 2008 (last search date from earlier reviews) to January 2012. Searches were supplemented by hand-searching reference lists of relevant studies and contact with experts in the field.
Study selection
Initially, all titles were examined by one reviewer. Citations that clearly did not meet the inclusion criteria were excluded. Then, all abstracts and full text articles were examined independently by two reviewers. All randomised controlled trials (RCTs) or observational cohort studies with a contemporaneous control group were included. Eligible studies included adult patients diagnosed with HF who had been recently discharged home (≤28 days) from an acute care setting. RM interventions included: (1) Home TM using patient initiated external electronic devices or cardiovascular implanted monitoring devices, with remote transfer of physiological data to the healthcare provider (2) STS including regular telephone contact between patients and healthcare providers and reporting of symptoms and/or physiological data. The comparator was standard postdischarge multidisciplinary care. The main outcomes included all-cause mortality, all-cause rehospitalisation, HF-related rehospitalisation, days in hospital, health-related QoL and patient-rated intervention acceptability.
Data abstraction and assessment of methodological quality
Data relating to study design, methodological quality and outcomes, were extracted by one reviewer into a standardised data extraction form and independently checked for accuracy by a second. Since this was an update of two previous reviews,11 ,12 all relevant data was extracted from the reviews, and cross-checked for accuracy with the original papers. Where necessary, additional data was extracted from the original papers or in cases of missing information, study authors were contacted. Study quality was assessed according to criteria based on Verhagen et al,17 for RCTs and by Wells et al,18 for observational studies.
Data synthesis and analysis
Data were tabulated and discussed in a narrative review. A network meta-analysis (NMA) of the following outcomes was deemed appropriate: all-cause mortality, all-cause rehospitalisation and HF-related rehospitalisation. NMA was conducted using Bayesian Markov chain Monte Carlo methods, and implemented using WinBUGS V.1.4.3.19 A random treatment effects model was fitted to the data to allow for the possibility of between-study statistical heterogeneity in treatment effects. Differences in response rate between studies due to variation in duration of follow-up were accounted for using a complementary log-log link function. This link function assumes that the parameter being analysed is the event rate (ie, hazard) from an exponential survivor function and that the treatment effect is the (log) HR. The model's convergence to its posterior distribution was assessed using the Gelman-Rubin convergence statistic.20 ,21 Total residual deviance was used to formally assess whether the statistical model provided a reasonable representation of the sample data. In a well-fitting model the residual deviance is expected to be close to the number of data points. Results of the NMA were reported in terms of the HR and 95% credible intervals (CrI) relative to the control intervention. The posterior median of the between–study SD together with the 95% CrI was also presented. To account for potential heterogeneity in intervention effects between studies, the posterior predictive distribution for the HR of a new study was also presented. The intention was to use meta-regression to explain any heterogeneity in the effects of the interventions between studies. However, due to limited data on relevant study-level covariates, meta-regression was not performed.
Results
Trial flow
Figure 1 summarises the process of identifying and selecting relevant literature. Of the 3060 citations identified, six new RCTs13 ,15 ,22–25 met the inclusion criteria and were added to the 15 trials26–40 from the previous systematic reviews.11 ,12 No trials of cardiovascular implanted monitoring devices or observational studies met the inclusion criteria as these were all conducted on outpatients with chronic HF.

Study flow chart.
Study and patient characteristics
Full study details are presented in table 1. All studies were published between 1999 and 2011. Eleven studies evaluated STS (10 of which were HH,24 ,26 ,28 ,31 ,34–39 while 1 was HM),13 nine studies assessed TM,15 ,22 ,23 ,25 ,27 ,29 ,32 ,33 ,40 and one study assessed STS and TM.30 Almost all the studies used different measures and devices as part of the STS and TM interventions. STS programmes generally included regular telephone contact between patients and healthcare providers and incorporated education and monitoring of signs and symptoms of worsening HF. TM programmes generally used patient-initiated external electronic devices with daily remote transfer of physiological data from the patient to the healthcare provider. In most TM studies, medical support was provided during office hours (9:00–17:00, Monday to Friday). One study provided medical support 24 hours a day, 7 days a week (24/7),33 and one provided support 7 days a week, 365 days a year (though not 24/7).32
Summary of study and patient characteristics
Data were obtained from various countries and regions including Europe, North America and South America. Follow-up duration ranged from 3 months24 ,28 ,34 ,40 to 15 months.30 Two studies initiated the intervention outside the specified period of 28 days (within 30 days13 or within 6 weeks).30 For both of these studies, it was assumed that most patients would have received the intervention within 28 days from discharge. Commercial funding was reported by 10 studies.15 ,22 ,23 ,25 ,30 ,32 ,34 ,36 ,38 ,40 Sample sizes ranged from 34 patients28 to 1653 patients,13 with mean participant age ranging from 57 years29 to 78 years. 27 The percentage of male participants ranged from 46%37 to 99%.39 One trial was restricted to patients with left ventricular ejection fraction (LVEF) <35%,32 three trials to LVEF ≤40%,26 ,30 ,34 and one trial to LVEF <45%.24 No LVEF inclusion criterion was reported in 16 studies.13 ,15 ,22 ,23 ,25 ,27–29 ,31 ,33 ,35–40
Quality assessment
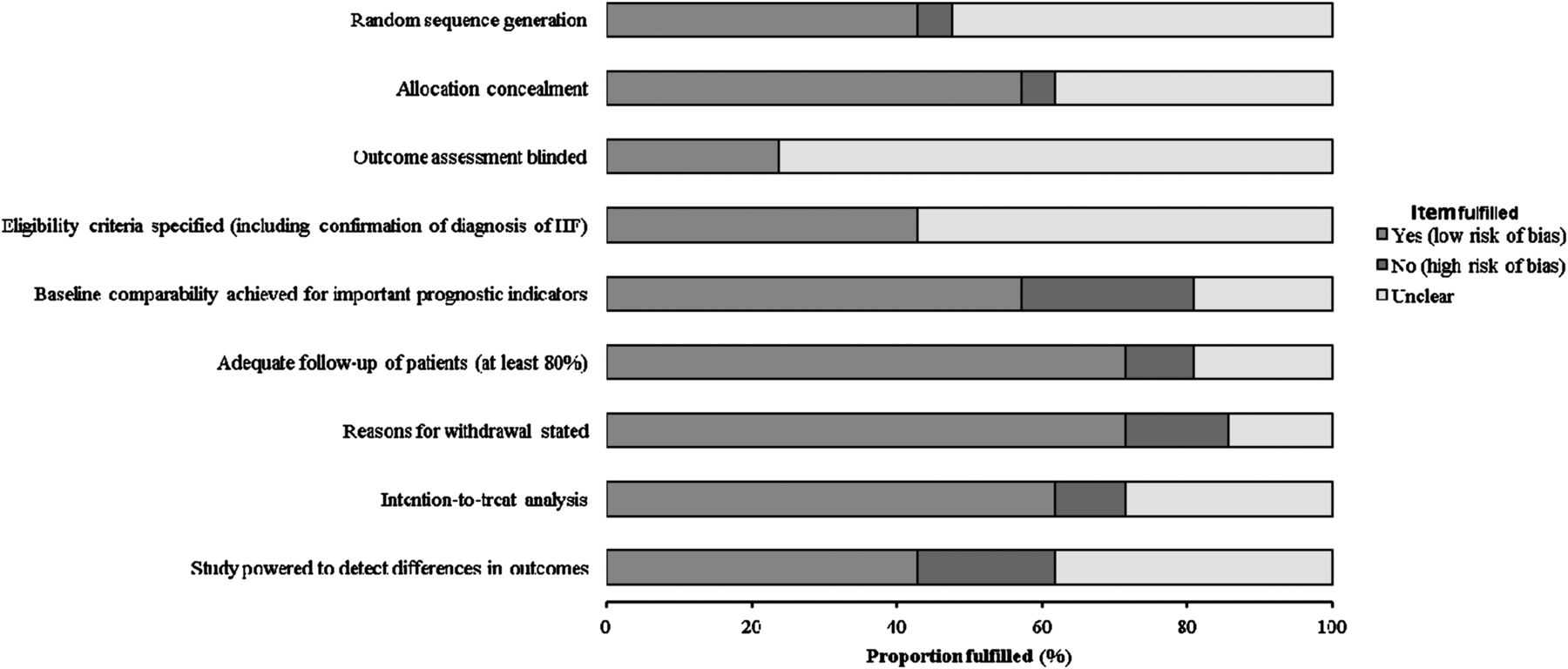
Figure 2 and online supplementary table S2 summarise the methodological quality of the included studies. Generally, nine studies performed well,13 ,22 ,23 ,26 ,30–32 ,37 ,38 receiving a positive assessment of at least six out of nine quality items. The most frequently identified potential sources of high bias concerned baseline comparability of prognostic factors (24%), adequate statistical power (19%) and reporting of numbers and reasons for being lost to follow-up (14%). A high number of publications poorly described the following aspects: random sequence generation (52%), allocation concealment (38%), blinding of outcome assessment (76%) and intention-to-treat analysis (29%). Although all studies specified eligibility criteria for study entry, the majority (57%) poorly described the definition and confirmation of HF diagnosis.

Methodological quality graph: Review authors judgments about each methodological quality item as percentages across all included studies. HF, heart failure. Access the article online to view this figure in colour.
Quantitative data synthesis
Figure 3 presents the network of evidence. Twenty-one studies comparing different pairs or triplets of interventions provided information on at least one of the outcomes being analysed. One study28 was excluded from the NMA because there were no events in each intervention arm and hence it provided no information about intervention effects.41 A sensitivity analysis was performed excluding data from Dar et al,22 (Home-HF trial) because it provided better-than-usual support and optimal medical treatment to patients in the control group. The 6 month mortality rate in the usual care group (5.5%) was substantially lower than would be expected in an HF cohort receiving care outside the context of a clinical trial (ie, between 13% and 21%).42 The inconsistency of the data with the rest of the trials was supported by the statistical analysis, which showed that the model including this study was not a good representation of the data from the study. Data included in the base-case NMA is provided in online supplementary table S3. For each outcome, the NMA provided an adequate fit to the data, with a residual deviance of 42.87 (40 data points) for all-cause mortality, 36.85 (33 data points) for all-cause hospitalisation and 22.18 (23 data points) for HF-related hospitalisation.

{kind=link}
{kind=link}
{kind=link}
Network diagram of different remote monitoring (RM) programmes versus usual care in recently discharged patients with heart failure (HF)a.
All-cause mortality
Table 2 summarises all-cause mortality data for the NMA of RM compared with usual care. TM interventions with medical support during office hours or 24/7 were associated with mortality reductions of 24% (HR: 0.76, 95% CrI: 0.49, 1.18) and 51% (HR: 0.49, 95% CrI: 0.20, 1.18), respectively, while STS HH was associated with a 23% reduction (HR: 0.77, 95% CrI: 0.55, 1.08). However, the results for TM 24/7 should be treated with caution due to the poor methodological quality of the only study in this network.33 No beneficial effect on mortality was observed with STS HM. The between-study SD was estimated to be 0.34 (95% CrI: 0.03, 0.75) suggesting mild to moderate heterogeneity in treatment effects between studies. A sensitivity analysis was performed excluding the Home-HF study22 (table 3). The between-study heterogeneity was considerably reduced. The interventions exhibiting the greatest effects were TM 24/7 (HR, 0.49; 95% CrI: 0.26, 0.88), TM during office hours (HR, 0.62; 95% CrI: 0.42, 0.89) and STS HH (HR, 0.75; 95% CrI: 0.59, 0.96).
All-cause mortality, all-cause hospitalisation and HF-related hospitalisation in recently discharged patients with HF: Posterior distribution for the HRs relative to usual care (random effects)
Sensitivity analysis excluding Dar et al:22 Posterior distribution for the HRs relative to usual care (random effects)
All-cause hospitalisation
TM interventions with medical support during office hours or 24/7 were associated with 25% (HR: 0.75, 95% CrI: 0.49, 1.10) and 19% (HR: 0.81, 95% CrI: 0.33, 2.00) reductions in all-cause hospitalisation respectively, whereas neither STS HM (HR: 1.06, 95% CrI: 0.44, 2.53) nor STS HH (HR: 0.97, 95% CrI: 0.70, 1.31) showed major effects (table 2). The between-study SD was estimated to be 0.38 (95% CrI: 0.13, 0.74), indicating small to moderate heterogeneity in treatment effects between studies. A sensitivity analysis excluding the Home-HF study22 (table 3) showed similar results with the greatest effect observed with TM with medical support provided during office hours (HR, 0.67; 95% CrI: 0.42, 0.97).
HF-related hospitalisation
There were no major effects on HF-related hospitalisation for STS HM (HR: 1.03, 95% CrI: 0.66, 1.54) or TM with medical support during office hours (HR: 0.95, 95% CrI: 0.70, 1.34). However, STS HH (HR: 0.77, 95% CrI: 0.62, 0.96) was associated with a 23% reduction (table 2). The between-study SD was estimated to be 0.11 (95% CrI: 0.00, 0.42) indicating little heterogeneity in treatment effects between studies. A sensitivity analysis excluding data from the Home-HF trial22 found similar results (table 3).
Length of stay
Six studies comparing STS to usual care reported length of stay.13 ,34 ,36–39 Only Tsuyuki et al,38 reported a statistically significant reduction in the length of hospital stay among the STS group (average: 6.6 vs 11.0 days, p<0.001). Two TM studies reported length of stay data,22 ,40 and found no significant between-group differences at 180 days (17 vs 13; p=0.99)22 or in the 1st year post-discharge (7.13 vs 6.71; p=not significant).40 The study which compared STS and TM to usual care reported no significant differences in the length of hospital stay between groups during 240 days of follow-up (p=not significant for all comparisons).30
Quality-of-life
Three STS studies reported significant improvements in physical (p=0.03)26 and overall measures (p<0.001) of QoL.28 ,39 One STS study found no significant differences between groups in either general or disease-specific QoL measures.37 Four TM studies measured QoL,22 ,27 ,32 ,40 two of which reported significant improvements in generic (SF-36 health perception, p=0.04627; SF-36, p<0.0540) and disease-specific measures (Minnesota Living with Heart Failure Questionnaire (MLHFQ), p=0.025).40 Goldberg et al32 observed improvements in QoL, although none of the differences reached significance (MLHFQ, p=0.22; SF-12, p>0.05; Health Distress Score, p=0.57). Similarly Dar et al22 found no significant differences between groups in either the MLHFQ (p=0.6) or the EQ-5D (p=0.5) measure over 6 months’ follow-up.
System acceptability and patient satisfaction
Five studies reported RM adherence,13 ,22 ,26 ,29 ,32 which ranged from 55.1%13 to 84%26 for STS and 81%29 to 98.5%32 for TM. Cleland et al30 reported overall acceptance of 91.2%, and a 96% satisfaction rate. Riegel et al36 and Laramee et al34 reported higher satisfaction among STS than usual care patients (both, p<0.01). Kielblock et al33 reported very high satisfaction, with 57% rating the TM ‘very good’, and the remaining 43% rating it ‘quite good’. Woodend et al40 reported satisfaction scores of between 92 to 97 out of 100 on a 10-item checklist. Scherr et al25 reported early termination of their study because an increasing number of patients were unable to operate the TM equipment, with 12 participants (10%) failing to transmit any readings, and a further 4 requesting early termination.
Discussion
This systematic review and NMA showed that RM interventions were generally associated with beneficial effects in reducing mortality and all-cause rehospitalisation in recently discharged patients with HF; however, these were statistically inconclusive. A sensitivity analysis, which excluded one trial that provided better-than-usual support to the control group,22 significantly enhanced the treatment effect, particularly in reducing all-cause mortality. Although data were limited, care packages which included STS and TM generally were associated with improved health-related QoL and were acceptable to patients.
The direction and magnitude of these results are broadly consistent with those of previous meta-analyses,11 ,12 but go beyond them, because the network technique allows dissection of the RM interventions into four broadly distinctive management modalities. In addition, this review included only a well-defined population of acute patients (RM initiated ≤28 days postdischarge), whereas existing reviews11 ,12 included people with acute and stable HF. In the more recent TIM-HF study (n=710), Koehler et al,14 failed to show any significant benefit of a TM system (where physician-led medical support was available 24/7); however, this study was excluded from the present review as it recruited patients who generally had very mild symptoms and no recent hospitalisation (eg, average duration of HF was approximately 7 years), thus, reflecting a different patient population from the current review.
HF is a complex illness, and optimal management requires regular patient monitoring. However, financial and organisational strain on healthcare systems frequently prevents timely monitoring. This can lead to reliance on patient help-seeking, which often occurs when it is too late to prevent hospitalisation. Recruiting the help of HF specialist nurses to visit the patients in the crucial first few weeks after discharge has been shown to reduce rehospitalisation rates.43 However, it may not be possible to meet the demands of the expanding population of patients with HF with physical contact from health professionals. Increasingly it is recognised that RM may enable a multidisciplinary team to input to the care decisions for more patients without the need for more staff members—an approach that is appealing to the funders of healthcare. Although our results suggest RM may be a helpful way to meet these needs, its importance is likely to be limited in people with well-controlled HF, or where high quality care currently exists. Indeed, this is the likely explanation for the lack of effect of RM on mortality in the Home-HF study, which provided better-than-usual support to patients in the control group.44 Thus, the implementation of RM could be adding to the quality of care, which results in the desired outcomes. When interpreting the results of RM it is important to consider how the control group was managed.
It is also important to highlight that RM does not impact on the course of HF unless the monitoring dictates an action. These actions are the reasons for changes in the outcomes analysed in this review. RM is part of a comprehensive package of care that includes education and empowerment of the patients, early warning of deterioration, access to health professionals’ advice and moral support, and pharmacological intervention. RM interventions therefore reflect complex healthcare strategies and are not limited to simple data-gathering. The complexity of any RM package should be considered when interpreting the outcomes of the systematic review, so that a reduction of mortality or a reduction of hospitalisation are not solely attributed to one format of RM intervention or another, but to the whole system of care that is being provided as a package.
There are a number of limitations to this review. RM interventions were heterogeneous in terms of monitored parameters and HF selection criteria. Some trials were underpowered to detect the primary outcome, and did not report outcome assessor blinding. Furthermore, few trials reported results in such a way as to enable assessment of intervention effect modifiers. Consequently, uncertainties remain around determinants of patient responsiveness, suitability of different systems, and ‘active ingredients’ of RM interventions. Few studies had greater than 6 months’ follow-up, so the duration for which RM would continue to confer benefits is also uncertain. RM usually builds on self-monitoring, with evidence that it can help educate patients about which symptoms and signs are most important, and what measures can be taken to restabilise the syndrome.45 The extent to which this happens is not usually reported by the studies. The content of RM interventions was often poorly described, making it difficult to understand exactly what was provided. Moreover, due to the differences in the selection criteria of the included studies (eg, LVEF and New York Heart Association), the generalisability of the treatment effect is unclear. Although several studies that were included in the NMA evaluated interventions in relatively small groups of patients, this may introduce bias. Small studies are usually less precise than larger studies, and published small studies tend to exhibit bigger effects as a consequence of publication bias.46 ,47 Small studies tend also, on average, to be of lower quality so that sample size is a proxy for study quality. While acknowledging the potential limitation in including such studies, excluding them may also introduce bias. The statistical model assumed that hazards and relative intervention effects were assumed to be constant over time; nevertheless this is better than assuming that study duration has no impact on the data. In addition, few tools existed to evaluate which patients did or did not have strong support from partners and carers, which may have impacted on the intervention effects.
In summary, although the effectiveness of RM varied widely according to the type of system used, STS HH and TM with medical support provided during office hours showed beneficial effects, particularly in reducing all-cause mortality for recently discharged patients with HF; however, these effects were statistically inconclusive. Where ‘usual’ care is below average or suboptimal, the impact of RM is likely to be greater. Given the complex nature of RM interventions, further research should seek to examine the ‘active ingredients’ of RM and qualitative research on patient and their partners or carers’ experiences of RM may be useful to understand45 ,48 the processes by which RM works. Future RM studies should include formal cost-effectiveness modelling and publish data to enable identification of subgroups that benefit most.
Acknowledgments
We would like to thank Gill Rooney, Project Administrator, ScHARR, for her help in the retrieval of papers and in preparing and formatting the paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Footnotes
-
Contributors AP was responsible for conception and design. RW developed the search strategy, undertook searches and organised retrieval of papers. AP and TG were responsible for the acquisition, analysis and interpretation of data. JWS and JW provided statistical support, undertook the network meta-analyses and interpreted the data. AA-M, AB, JGFC and MRC helped interpret data and provided a methodological, policy and clinical perspective on the data. AP and TG wrote the drafts of the manuscript which were subsequently revised and approved by all authors. AP coordinated the review and is the guarantor.
-
Funding This project was funded by the UK NIHR Health Technology Assessment programme (project number: 09/107/01) as part of a larger review on ‘Home telemonitoring or structured telephone support programmes after recent discharge in patients with heart failure.’ Visit the HTA programme website for more details http://www.hta.ac.uk/project/2351.asp (PROSPERO registration number: CRD42011001368). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the UK Department of Health’
-
Competing interests JGFC has a financial interest in the companies who manufacture external electronic devices or cardiovascular implanted monitoring devices for home telemonitoring systems included in this review. JGFC is Chief Medical Officer on an EU/FP7 grant (HeartCycle) that includes Philips and Medtronic, providers of telemonitoring equipment. JGFC is also in receipt of research support from Philips and has consulted and received research funding from Bosch and General Electric who have interests in this area. MRC has received research grants from Honeywell HomMed, Philips, Medtronic, Boston Scientific, Medtronic and St Jude Medical for the assessment of remote monitoring in patients with heart failure, and has provided consultancy advice to Bosch, Medtronic, St Jude Medical, Boston Scientific and General Electric who have interests in this area. He owns no stocks or shares in any such company. AB has no conflicts related to this paper, but is a consultant to various pharma and device partners and has acted as a lecturer, scientific and clinical trials advisor to numerous partners and recruited to commercially sponsored and NIHR sponsored clinical trials. He owns no shares or stocks in companies related to this work.
-
Provenance and peer review Not commissioned; externally peer reviewed.