Article Text

Abstract
Background In India, cardiovascular events are often diagnosed at lower blood pressures (BP) than in Western countries, questioning whether the actual World Health Organization cut-off points for hypertension (systolic BP (SBP) ≥140 mm Hg and/or diastolic BP (DBP) ≥90 mm Hg) are appropriate in low resource countries.
Methods A large population-based cohort study including 167 331 adults aged 35–90 years, living in a rural area, was followed up during a 7-year mean duration for all-cause mortality and cardiovascular disease (CVD) deaths. At baseline, casual BP was measured, and lifestyle was assessed through a questionnaire. Death rates were calculated according to SBP and DBP, and their association was examined in a multivariate analysis, among all subjects, then stratified by sex and age groups.
Results Forty-five per cent of the study subjects had hypertension. The nadir of CVD death rates was observed at 110 mm Hg for casual SBP and 75–80 mm Hg for casual DBP. In the multivariate analysis, SBP from 120 mm Hg and DBP from 90 mm Hg were significantly associated with risks of ischaemic heart disease and stroke. High SBP and DBP values were greater predictors of mortality in the young age group (34–44 years) than in the old age group (65+ years). SBP was a stronger independent predictor of CVD than DBP.
Conclusions SBP and DBP were associated with CVD mortality at thresholds lower than the current hypertension definition. Measurement limited to SBP alone would be effective in screening for CVD risk in large populations.
- Hypertension
- cardiovascular diseases
- mortality risk
- longitudinal study
- developing countries
Statistics from Altmetric.com
High blood pressure (BP) is a major risk factor for cardiovascular diseases (CVDs) mainly represented by ischaemic heart disease and stroke.1 Ischaemic heart disease kills more than 7 million people each year, while stroke kills 5.5 million.2 CVDs are not diseases of affluent countries only, as 80% of CVD deaths occur in low and middle income countries.3 Except in sub-Saharan Africa, where it ranks second after diseases of infectious, parasitic and nutritional aetiology, CVD is the leading cause of death in the world.3–5 In 2004, in India, 1.5 million deaths from ischaemic heart disease and 800 000 deaths from stroke were estimated, representing 27% of total deaths.2
A meta-analysis of hypertension prevalence in India reported growing time trends of hypertension in both urban and rural populations and in both sexes,6 7 supporting the fact that hypertension is a rising problem in India, while in high income countries, mean BP levels are declining with decreasing prevalence of hypertension, thanks to preventive interventions and effective treatments.6 As a consequence of rising hypertension, a steady increase in CVD rates are observed in India in both urban and rural communities,8 although they are more prevalent in urban areas.9 Moreover, CVD occurs at a younger age than in Western countries.9 10 Murray and Lopez11 estimated that CVD deaths below the age of 70 years represented 22.8% of deaths in high resource countries and 46.7% in low resource countries, of which 52.2% is in India.
The association between BP values and CVD has not been estimated through longitudinal studies in India. Although studies from developing countries reported lower mean BP values than in developed countries,7 12 the current World Health Organization/International Society of Hypertension (WHO/ISH) definition of hypertension is in use, that is systolic BP (SBP)≥140 mm Hg and/or diastolic BP (DBP)≥90 mm Hg and/or use of antihypertensive medications.13 It has been reported that cardiovascular events, and particularly ischaemic heart disease, were often diagnosed at lower BP levels than the actual WHO/ISH cut-off points,12 questioning whether appropriate (and lower) limit values of BP to define hypertension should be used for developing country populations. Longitudinal studies—in measuring BP at baseline and registering cardiovascular events during the follow-up period—would allow estimating BP values associated with increased risk of cardiovascular events and consequently defining proper BP cut-off points for specific populations.
A large population-based cohort study in southern rural India was implemented, assessing the casual SBP and DBP values at baseline. Study participants were actively followed up during a mean duration of 7 years for vital status and cause of death. The aim of the present study was to estimate the prognosis criteria of BP values and to define the systolic and diastolic values associated with increased CVD risks.
Methods
The present study is an ongoing cluster-randomised community-based oral cancer screening trial implemented to evaluate the efficacy of oral visual inspection on oral cancer incidence and mortality. The study, which is described elsewhere,14 15 was carried out in a rural area of the Trivandrum district, Kerala State, India. A total of 191 873 subjects aged 34 years and older were eligible, out of which 167 331 were recruited between 1 January 1996 and 31 December 2004 during three successive screening rounds (87% participation rate).
The study participants are currently being followed up for cancer incidence and mortality. The study protocol was reviewed and approved by both the scientific and human ethics committees of the Regional Cancer Centre, Trivandrum, and the International Agency for Research on Cancer, Lyon, France. A written informed consent was obtained from each participant.
BP was measured during the first two rounds, among 131 881 subjects. We excluded those who stated an age of more than 90 years because of low reliability (n=153) and those with missing information on BP values or extreme systolic (<90 and >250 mm Hg) and diastolic values (<50 and >200 mm Hg) (n=177), which brought the total study sample to 130 551 subjects.
Blood pressure measurement
Casual BP was measured through two readings, using Phases I and V Korotkoff sounds to identify the systolic and diastolic pressures. The first reading was used in all analyses of the present study. Measurements were performed by trained health workers at the subjects' homes, using standard mercury sphygmomanometers used in India with a cuff of 12.5 cm wide and 22 cm long, on the right arm, the subject being in a seated position after a 5 min rest in a comfortable position.
Lifestyle questionnaire
All participants answered a lifestyle questionnaire administered by trained health workers during house visits. Information on sex, age, total monthly household income, level of education, occupation, household assets, medical history of severe diseases, number of permanent household residents, type of house, religion and lifestyle habits on tobacco chewing, tobacco smoking and alcohol drinking were collected. Height and weight were measured to estimate the subject's body mass index (BMI=weight in kilogrammes divided by the square of the height in metres).
Identification of mortality cases and follow-up
Each subject was actively followed up for vital status by field workers through municipal death registers, death records from mosques, churches and social organisations, and during repeated house visits. If medical records were not available, the cause of death was established by interviewing a close family member of the deceased person using a verbal autopsy questionnaire16; these questionnaires were then reviewed by a medical doctor for coding the cause of death according to the International Classification of Diseases—10th revision.
The start of the follow-up was the date of interview. The end of the follow-up was either the date of death, or 31 December 2005, whichever came first.
Outcome was all-cause mortality and CVD mortality (ischaemic heart disease and stroke).
Statistical analysis
The mean SBP and DBP values and the percentage of hypertension were computed according to sex, age, assets and BMI.
Death rates of all-cause, ischaemic heart disease and stroke were estimated. SBP of 110 mm Hg and DBP of 80 mm Hg had the lowest death rates; consequently, the 100–119 mm Hg category for systolic values and 80–89 mm Hg category for diastolic values were used as the reference categories in the multiplicative hazard function models. Relative risks (RRs) were computed using the Cox regression methods, and confidence intervals (CIs) were based on Wald statistics, and were estimated for the SBP and DBP values categories. Risks were adjusted for potential confounding factors, such as sex, age (continuous), education level (illiterate, 1–7 years, 8–10 years, college), income level in rupees (<1500, 1500–3000, 3001–5000, >5000), occupation (blue collar, white collar, business, housewife), standard of living based on household equipment (deprived, moderate, privileged), number of household residents (≤5 and ≥6), house type (thatched hut, tiled hut, concrete), religion (Hindu, Muslim, Christian), BMI (continuous), tobacco chewing status (never, current, past), smoking status (never, current, past) and alcohol drinking status (never, current, past), using the backward selection method. Risks were adjusted for religion because we previously reported that, in the present cohort, current drinkers were more often Christians than Hindus, Hinduism not allowing alcohol intake.17 However, we know that, at a moderate consumption level, alcohol is a protective factor of CVD.
RRs were estimated on total population, stratified by sex and by age groups (34–44, 45–64, 65 years and over). Because of a non-linear association between mortality risks and BP, tests for quadratic trend were performed. RRs of all-cause and CVD deaths as compared with staying alive were calculated using the Statistical Analysis System PHREG procedure.18
Results
The analysis included 130 551 subjects (50 193 men and 80 358 women). The mean age was 50 years (SD, 13 years), the mean SBP value was 131 mm Hg (130 mm Hg in men; 131 mm Hg in women) and the mean DBP value was 85 mm Hg (84 mm Hg in men; 85 mm Hg in women). Hypertension, defined as SBP ≥140 mm Hg and/or DBP ≥90 mm Hg, was present in 44.5% of the study subjects.
Mean values of SBP and DBP and hypertension prevalence did not differ between men and women, but they increased with increasing age, socioeconomic status and BMI (table 1).
Mean values of blood pressure and percentage of hypertension according to different variables
During a mean follow-up of 7 years (970 536 person-years), 11 486 deaths (6362 men and 5124 women) were registered. The common causes of deaths were attributed to ischaemic heart disease (1682 men and 959 women), stroke (641 men and 725 women), cancer (739 men and 551 women) and chronic respiratory diseases (739 men and 529 women). In this cohort, CVD represented 35% of causes of death.
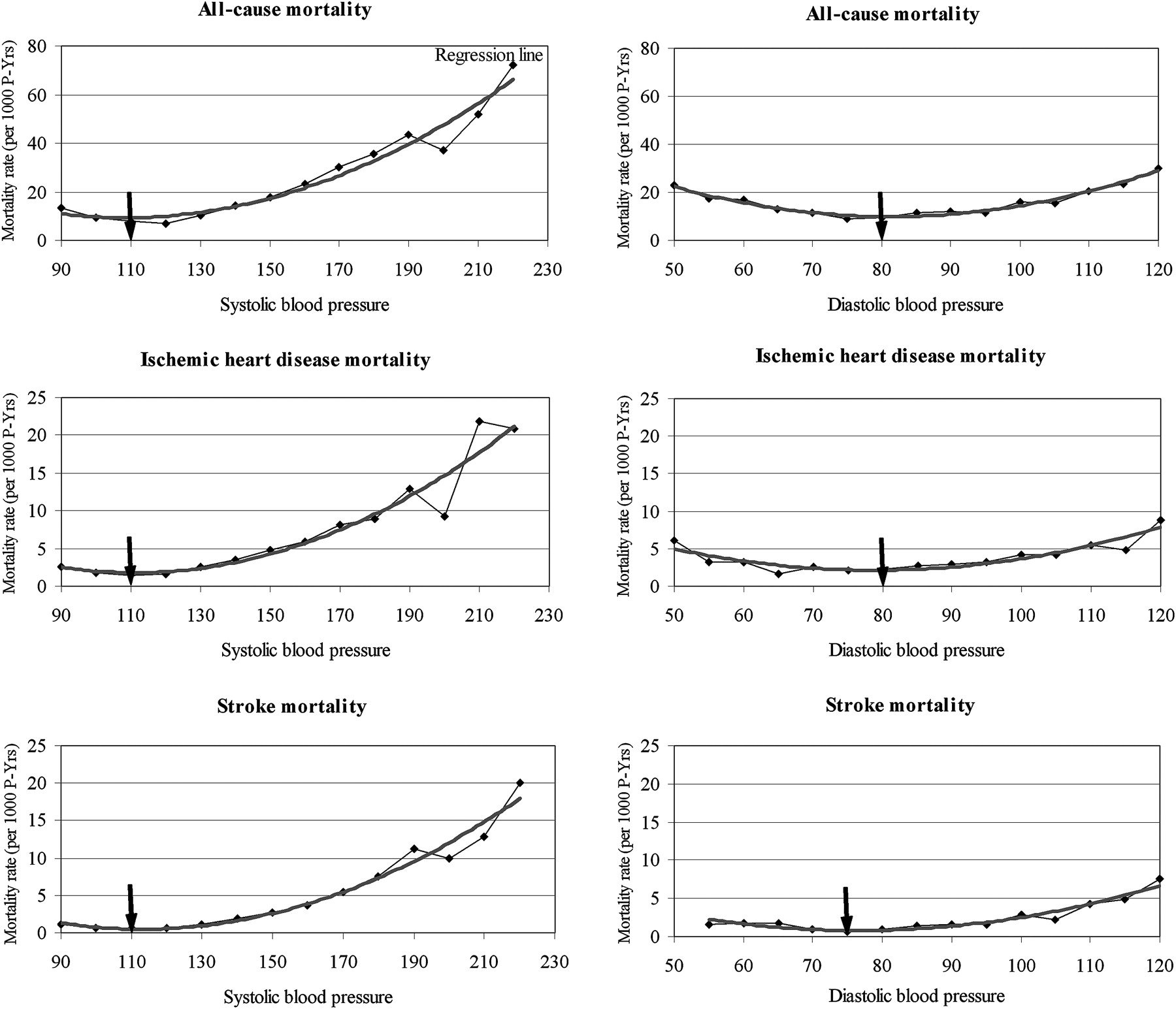
Figure 1 shows the death rates according to SBP and DBP values. For all-cause, ischaemic heart disease and stroke, the three death rates increased with increasing SBP in a J-shaped manner, the lowest rate being at 110 mm Hg. The three death rates showed a U-shaped mode with DBP, the lowest rate being between 75 and 80 mm Hg.

Death rates of all-cause and cardiovascular diseases according to values of systolic and diastolic blood pressures.
Risk of all-cause death increased significantly from 140 mm Hg of SBP and risks of CVD death from 120 mm Hg (figure 2). For an identical SBP value, the risk of dying from stroke was higher than from ischaemic heart disease; as compared with an SBP of 110–119 mm Hg, SBP≥180 mm Hg was related to an RR of death from ischaemic heart disease of 3.06 (95% CI 2.55 to 3.67) and an RR of death from stroke of 5.10 (3.96 to 6.58). The risks of death increased significantly with a DBP exceeding 90 mm Hg, with a greater effect for stroke mortality. As compared with a DBP of 80–90 mm Hg, a BP of 110 mm Hg or higher was associated with a risk for all-cause mortality of 1.77 (1.64 to 1.92). For death due to ischaemic heart disease, the risk was 1.98 (1.70 to 2.30), and for death due to stroke, it was 3.28 (2.72 to 3.96).

{kind=link}
{kind=link}
Relative risks of mortality according to systolic and diastolic blood pressure values. Risks adjusted for age, sex, education level, income level, occupation, household assets, household residents, type of house, religion, BMI, chewing habits, smoking habits, drinking habits.
In a sensitivity analysis, the follow-up period excluded the first year in order to eliminate any extreme BP related to a terminal condition. No change in risk was observed; for SBP<100 mm Hg, the risks of all-cause mortality were 1.20 (0.98 to 1.48) when all follow-up years were included and 1.15 (0.92 to 1.44) when the first year was excluded. Similarly, for DBP <70 mm Hg, the risks of all-cause mortality were 1.07 (0.97 to 1.17) with all follow-up years and 1.03 (0.94 to 1.14) without the first year.
Table 2 presents risks of CVD mortality stratified by sex and age groups. Similar levels of risk were observed in men and women, although in women, the lowest SBP and DBP categories were also associated with increased risk in a U-shaped relationship.
CVD mortality risks according to systolic and diastolic blood pressure values, stratified by sex and age-group
Risks of CVD mortality increased from the category 140–159 mm Hg of SBP in the young age group (34–44 years) and from the 120–139 mm Hg category in the middle age and older groups. A DBP≥100 mm Hg was related to increase risks of CVD mortality, especially stroke in the middle age group. The association between high SBP (≥160 mm Hg) and high DBP (≥110 mm Hg) and CVD mortality was greater in the young age group.
Discussion
In this prospective study of adults living in a rural area of Southern India, casual BP was related to age, BMI and socioeconomic status. CVD represented the highest mortality toll with 35% of total death cases. The nadir of CVD death rates was observed at 110 mm Hg for casual SBP and 75–80 mm Hg for casual DBP. The risks of dying from ischaemic heart disease and stroke started to increase from 120 mm Hg of SBP and from 90 mm Hg of DBP, especially among the middle and old age groups. These values are similar to the findings of a recent extensive meta-analysis that reported increased risks of CVD mortality from an SBP of 115 mm Hg and from a DBP of 75 mm Hg, without any evidence of a threshold.19 High values of SBP were greater predictors of mortality in the young age group (34–44 years) as compared with the old age group (65 years and older). DBP was not a strong independent predictor of CVD mortality as SBP was, especially among the older group.
We report a higher toll of CVD deaths than for all India (27%). This is explained by the high prevalence of hypertension among the southern populations of India.20–26
Our results are opposite to those of the Framingham Heart Study findings, where SBP was a better determinant of CVD with increasing age.27 However, they are in line with the results of two meta-analyses where the association between BP and CVD was attenuated with age.19 28 It is most likely that young and older people differ in terms of determinants for CVD. Mortality from CVD in older people is associated to multifactor predictors such as high BP, dyslipidaemia, diabetes, prolonged tobacco smoking habits, etc with hypertension being one of the determinants. In the young age group, few predictors are involved with CVD mortality, and BP is likely to be strongly linked with a higher attributable fraction than in older people.1
SBP is consistently reported as the best predictor (over DBP) of CVD incidence or mortality in large epidemiological studies such as the Multiple Risk Factor Intervention Trial or the Cardiovascular Health Study in the USA, the Honolulu Heart Program in Hawaii and the British Regional Heart Study in Great Britain.29–32 The present large population-based prospective study in rural India is consistent with Western studies, and it has been argued that measurement limited to SBP alone would be effective in the screening of hypertension in large populations.
High BP is a major treatable and reversible cardiovascular risk factor.12 33 The burden of CVD mortality is decreasing dramatically in high resource countries (50% in Australia and 60% in Japan between 1965 and 1990), although it remains the main cause of death.34 However, the burden of CVD is increasing with the higher socioeconomic level in low resource countries because of the increased prevalence of risk factors and lack of access to preventive interventions.35 36
This study presents a certain number of limitations. First, BP values were based on casual, not ambulatory, BP; it is well known that BP is fluctuant, and subjects may have transiently high BP. On the other hand, BP was measured at the subject's home, in his/her environment when it is usually lower than at the physician's office, with no white-coat effect.23 Second, analysis was based on a single-session measurement, with a possibility of overdiagnosed hypertension.37 Third, although health workers were properly trained to measure BP, we cannot exclude a within-observer error in the BP assessment. Finally, no information on the use of antihypertensive medication was collected, and no lipid profile was measured.
In a low resource country, such as India, death registration is often incomplete. We tried to overcome this problem by actively collecting death information during repeated house visits. These visits significantly amplified the proportion of information on death, as compared with the information obtained from government registries. When medical information was not available, verbal autopsy was used, and the cause of death neared completeness.
Kearney et al projected an increase in the prevalence of hypertensive patients in India by 1.5-fold between the years 2000 and 2025 (128 million men and women in 2000 to 213 million in 2025).38 This increase is anticipated to be associated with a concomitant increase in CVD incidence cases (14 million patients from rural areas and 16 million from urban areas) and CVD deaths over the next 25 years because of increased lifespan, longer exposure to risk factors, inappropriate lifestyles due to industrialisation and urbanisation.9 36
In order to reduce the future CVD pandemics and its huge burden on the healthcare system in India, health education of the populations is needed—such as antismoking campaigns, promotion of physical exercise and a diet low in fat and salted food—as well as national strategies on prevention and screening for hypertension.9 34 39 The use of a single casual SBP value greater than 120 mm Hg observed on several occasions seems an appropriate screening tool in low resource countries where ambulatory BP cannot be assessed.
What is already known on this topic
Hypertension is a strong predictor of CVDs.
Mean BP values observed in India are often reported lower than those from developed countries.
In India, the association between BP values and risk of CVDs has not been estimated through longitudinal studies.
What this study adds
The risk of CVDs increases from systolic values of 120 mm Hg and diastolic values of 90 mm Hg.
SBP is a stronger independent predictor of CVDs than diastolic BP.
Measurement of SBP solely in large populations in field settings may be useful for hypertension screening.
Acknowledgments
This project was supported by a generous grant from the Association for International Cancer Research (AICR) St Andrews, UK, without whose assistance this study would not have been possible. Additional data collection is supported by the Cancer Research UK (CRUK), UK. We are grateful to the study participants and their families, the assistance of the staff of the Panchayath offices, of mortality registries and of the Trivandrum population-based cancer registry. We are also grateful to Professor Shuichi Hatano and Professor Flávio Fuchs for useful comments on the draft and Mrs Evelyn Bayle for editorial work.
References
Footnotes
Funding The Association for International Cancer Research (AICR) St Andrews, UK–the Cancer Research UK (CRUK), UK.
Competing interests None.
Ethics approval This study was conducted with the approval of both the scientific and human ethics committees of the Regional Cancer Centre, Trivandrum and the International Agency for Research on Cancer, Lyon, France.
Provenance and peer review Not commissioned; externally peer reviewed.