Article Text

Abstract
Objectives Bone pathologies as detected on MRI are associated with the presence of pain in knee osteoarthritis (OA). The authors examined whether bone attrition assessed on x-rays was associated with pain, stiffness and disability.
Methods The authors analysed x-rays of 1326 knees with OA from 783 individuals participating in the cross-sectional population-based Somerset and Avon Survey of Health. The diagnosis of OA was defined by the presence of osteophytes in anteroposterior (AP) or lateral views. Bone attrition was graded from 0 (no attrition) to 3 (severe attrition >10 mm) and Kellgren and Lawrence (K/L) scores were assigned on AP views. Logistic regression models adjusted for gender, age, body mass index, effusion and K/L scores were used to determine whether bone attrition was associated with pain, stiffness and disability.
Results Pain was reported in 84 knees (74%) with radiographic bone attrition compared with 505 (42%) without bone attrition (adjusted OR 2.22, 95% CI 1.29 to 3.80). The adjusted OR was increased for day pain but not for night pain (p for interaction <0.001). Stiffness was reported for 85 knees with bone attrition (75%) and 437 knees without (36%) (adjusted OR 3.23, 95% CI 1.85 to 5.64). Disability was reported by 40 individuals with bone attrition (50%) and 140 individuals without (24%) (adjusted OR 2.09, 95% CI 1.19 to 3.68).
Conclusions Bone attrition detected on conventional x-rays using a simple cheap technique is strongly associated with the presence of day pain, stiffness and disability in knee OA.
Statistics from Altmetric.com
Introduction
Knee pain is a major public health problem.1,–,3 In older people the cause of knee pain is generally attributed to osteoarthritis (OA).4 However, we know that many people with radiographic changes suggestive of knee OA are not in pain.5,–,7 In addition, knee pain can be due to a number of other pathologies including periarticular problems such as anserine bursitis8 and bone pathologies such as bone marrow lesions.9 Joint pathology has been assessed radiographically in the past.10 However, because of the relatively poor correlation between symptoms and radiographic changes,5,–,7 most investigators now opt to use more sophisticated joint imaging techniques such as MRI.11 12 Alternatively, they have looked for other technologies with which to explore the problem, such as functional imaging of the brain.13 These techniques may provide us with valuable insights into pain mechanisms but cannot easily be used in routine clinical work or in epidemiological studies.
We recently described a simple method with which to assess bone attrition at the knee joint on routine x-rays.14 Bone attrition was defined as a vertical loss of bone volume in the affected condyle. Our data, derived from a cohort with advanced OA of the knee, suggested that bone attrition might be related to night pain.14 Others have found subchondral bone marrow oedema as detected on MRI to be associated with pain in the osteoarthritic knee.9 Using data from the community-based Somerset and Avon Survey of Health (SASH),15 16 we determined whether bone attrition as detected on conventional anteroposterior (AP) x-rays is associated not only with knee pain but also with stiffness and disability.
Methods
Sampling of participants
SASH is a population-based cross-sectional study of 28 080 people randomly selected from 40 general practices in the south-west of England.15 17 After exclusion of 2034 people who had either moved out of the study area, suffered from a severe mental or terminal illness or were deceased, 26 046 people were included in the study.
Screening process
All 26 046 subjects were sent a screening questionnaire comprising questions on general health, utilisation of health services and symptoms of hip and knee disease. Non-respondents were sent two reminders and contacted by telephone if necessary.17 18 We screened people for knee pain using a modified version of the question used in the first National Health and Nutrition Examination Survey:19 ‘During the past 12 months, have you had pain in or around either of your knees (hips) on most days for 1 month or longer?’ Participants who reported knee or hip pain were invited for further examination either at a clinic or by home visit. Examinations were organised into two phases by location of participating practices.
Assessment of symptoms and signs
Examined participants were asked about knee pain, stiffness and disability using the following questions: ‘In the past 12 months, have you had pain in or around your left (right) knee on most days for 1 month or longer during the day?’ (yes/no). This question was repeated for night pain, referring to ‘during the night’. Participants were considered to suffer from knee pain if they reported either day or night pain. ‘In the past 12 months, have you experienced stiffness in or around your left (right) knee on most days for 1 month or longer (yes/no)?’ and ‘How difficult is it for you to go outdoors and walk down the road on your own (not difficult/quite difficult/very difficult/impossible)?’ Disability was not assessed in the first 127 participants who underwent clinical examination during the first phase of the study and considered present if participants indicated that walking was at least ‘quite difficult’. The presence of an effusion in either knee was determined based on clinical examination.
Radiographic evaluation
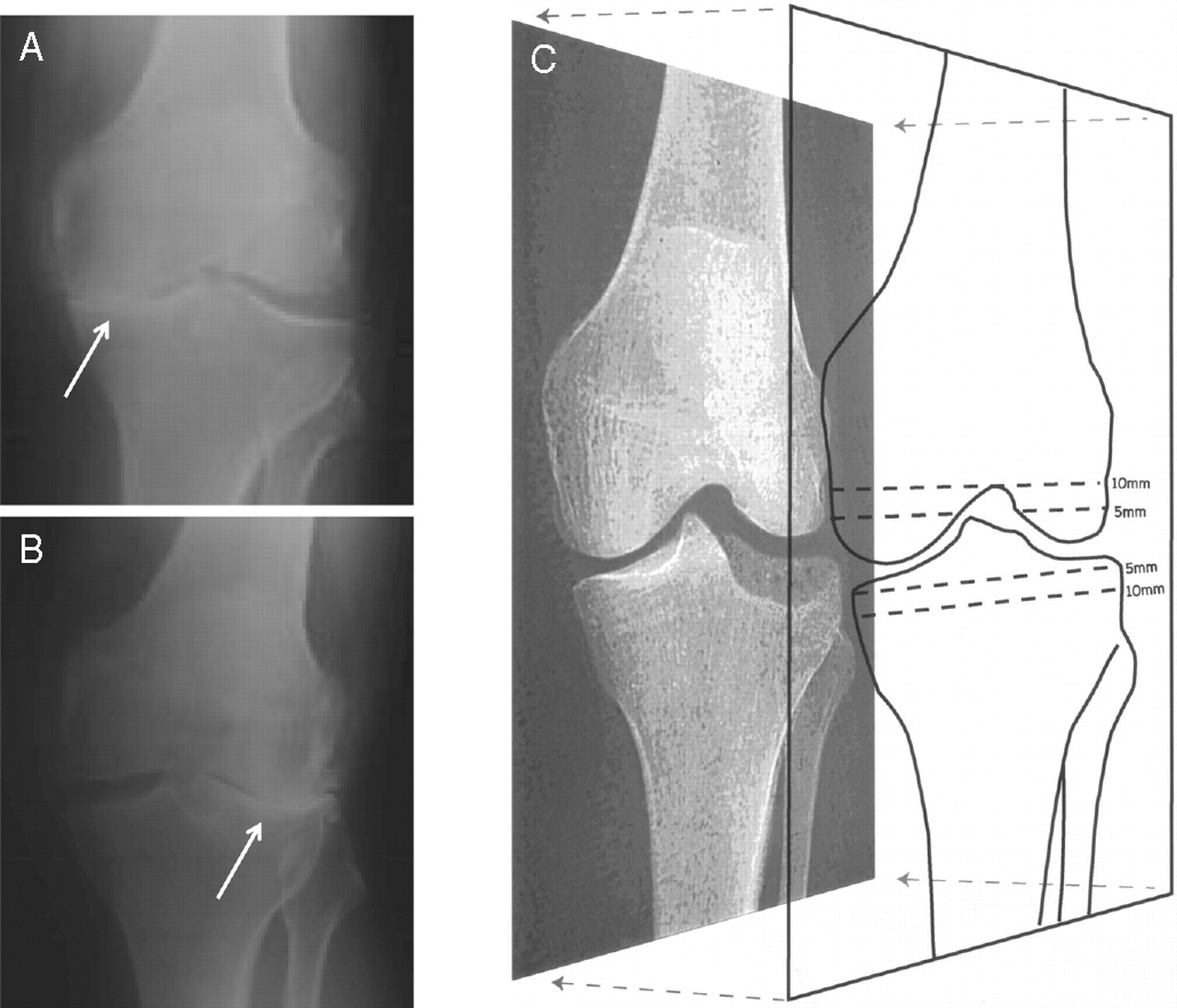
Participants underwent weightbearing AP and lateral x-rays of the knees according to a standardised protocol. For AP views the legs were extended in slight internal rotation. All films were processed and assessed in a blinded manner. We used weightbearing AP knee x-rays that were considered to be normal to develop templates of knee joint contour outlines.14 These could be overlaid onto the knee x-rays of the study subjects to determine the presence of bone attrition, defined as a vertical loss of bone volume in the affected condyle (figure 1). Alignment of the normal contours of the femur and tibia allowed measurement of the extent of bone attrition separately for the femoral condyles and tibial plateaus. Three different template sizes were used for knees of small, medium or large dimensions. As previously described, we graded attrition on a scale from 0 to 3 (0 = no attrition, 1 = attrition of doubtful significance (<5 mm), 2 = definite attrition of a moderate degree (5–10 mm), 3 = severe attrition (>10 mm).14 Using a standard atlas,10 we then rated the worst osteophytes from 0 to 3 (0 = none; 1 = minute; 2 = definite, of a moderate degree; 3 = severe) for both parts of the tibiofemoral joint on AP and lateral x-rayss. OA was defined by the presence of grade 1 osteophytes or higher on AP or lateral views.9 Finally, we assigned Kellgren/Lawrence (K/L) grades of global radiological severity on AP views using a scale from 0 to 4 (0 = no features of OA, 1 = minute osteophytes of doubtful significance; 2 = definite osteophytes, no definite joint space narrowing; 3 = definite joint space narrowing of a moderate degree; 4 = severe joint space impairment).20 One investigator (SR) who was blinded to each participant's clinical information performed a single assessment of all x-rays. A random sample of 30 films was also assessed by one independent observer (PAD). Intrarater agreement was moderate for the semiquantitative grading of bone attrition with a weighted κ value of 0.82 (95% CI 0.61 to 1.00), was high for semiquantitative K/L grading with a weighed κ value of 0.88 (95% CI 0.70 to 1.00) and was high for detection of osteophytes with a κ of 1.00 (95% CI 0.74 to 1.00). Inter-rater agreement was moderate for the semiquantitative grading of bone attrition with a weighted κ value of 0.58 (95% CI 0.39 to 0.78), was moderate for semiquantitative K/L grading with a weighed κ value of 0.81 (95% CI 0.69 to 0.92) and was moderate for detection of osteophytes with a κ of 0.72 (95% CI 0.59 to 0.86).

Different grades of bone attrition. (A) Grade 1 bone attrition (white arrow) of <5 mm of the medial tibia plateau. (B) Grade 2 bone attrition (white arrow) of 5–10 mm of the lateral tibia plateau. (C) Grade 3 bone attrition of >10 mm of the lateral tibia with the overlaid template to outline the joint contour. Broken lines on the template indicate the cut-off points for levels of bone loss. Modified from Dieppe et al14.
Statistical analysis
Analyses were at knee level for the analysis of pain and stiffness and at participant level for disability. Logistic regression models were used based on robust standard errors that accounted for the clustering of knees within participants where appropriate and the association of bone attrition grade ≥1 (pre-specified) with knee pain, stiffness and disability was determined. We estimated crude OR with corresponding 95% CIs and OR adjusted for gender, age, body mass index and overall radiographic severity based on K/L scores and the presence of joint effusion. Analyses were restricted to knees or participants with radiographic knee OA9 with complete covariate information. To explore the impact of excluding knees or participants with missing covariate information, we calculated estimates of the associations of bone attrition with symptoms separately for complete and incomplete datasets. In sensitivity analyses we distinguished between grade 1 and 2 bone attrition. p Values for interaction between estimated OR and extent of bone attrition were derived from the appropriate interaction term in the logistic regression model. We then estimated separately the association of bone attrition with day pain and with night pain using matched pairs logistic regression, which accounted for the correlation between the two pain types within knees. All analyses were performed in STATA 10.1 (Stata Corporation, College Station, Texas, USA).
Results
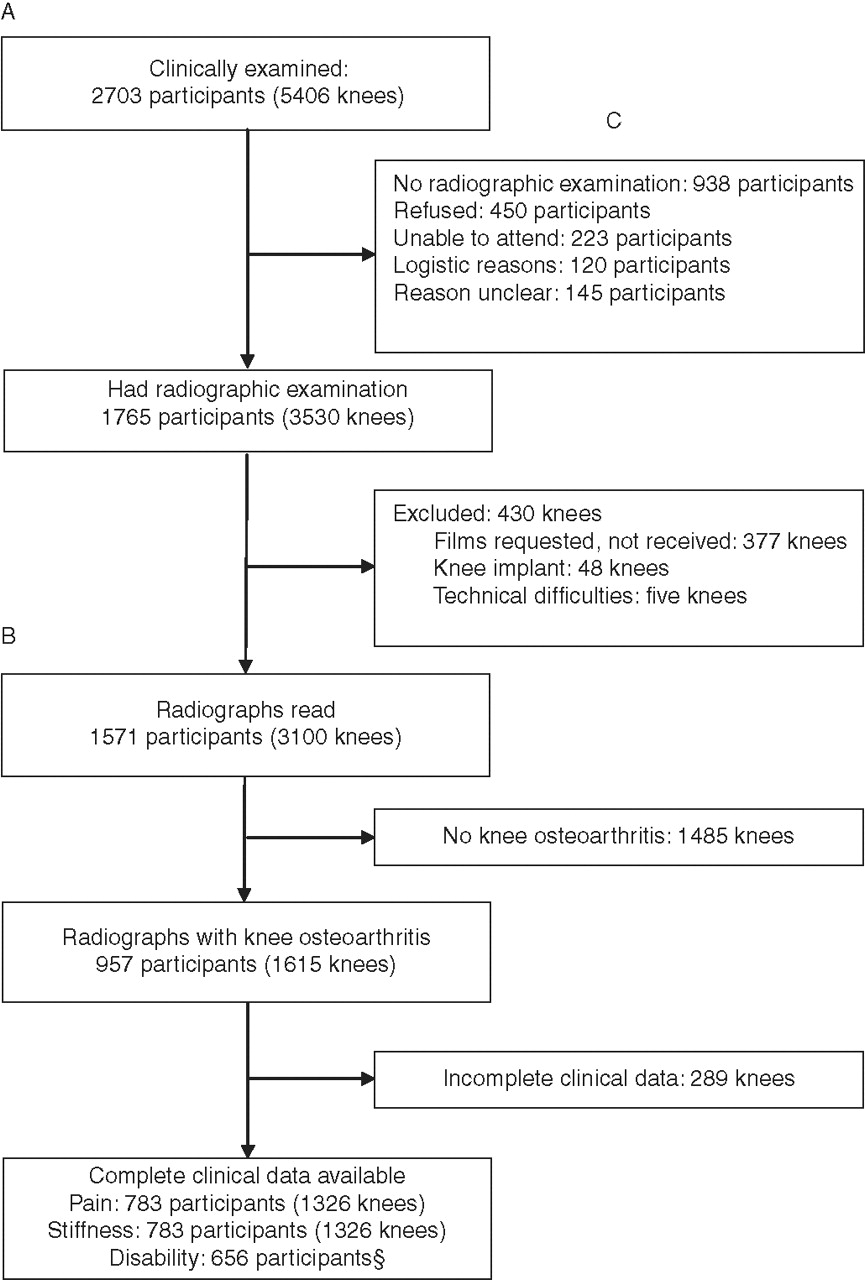
The flow of participants from screening stage to stage of clinical examination was reported previously.15 16 In short, 22 978 individuals responded to the screening questionnaire, 22 217 completed the question on hip pain and 22 379 the question on knee pain. A total of 6416 participants reported hip or knee pain (29%). Of these, 4304 were invited for further examination (67%) and 2703 attended (63%).15 16 Figure 2 shows the flow of clinic attendees through the study; 938 participants did not have a radiographic examination, most frequently because they refused or because they felt unable to attend due to general frailty or comorbid conditions. A total of 3530 knees from 1765 participants had undergone radiographic examination but 430 knees were excluded, most frequently because radiographic examinations performed before the beginning of the study could not be obtained for central reading. Films of 3100 knees from 1571 participants were read and 1615 knees from 957 participants were diagnosed with radiographic OA. Complete clinical data were available for 1326 knees from 783 participants. Disability was not assessed for the first 127 participants with radiographic OA during the first phase, so data on disability was available for 656 participants with radiographic OA (figure 2).

Study flowchart. Note that disability was not assessed in the first 127 participants of the first phase of the study, so only 656 participants contributed to the analysis of disability.
The characteristics of the 783 participants (1326 knees) with radiographic and clinical information are shown in table 1. Participants with bone attrition were on average 4 years older than participants without bone attrition (p<0.001). The 114 knees all had a K/L score ≥2, with a trend towards higher K/L scores in knees with bone attrition as opposed to predominantly low K/L scores in knees without (p<0.001). A total of 270 knees without attrition were assigned a K/L score of 0, with osteophytes only detectable on lateral views. Effusions were detected clinically in 77 knees overall (6%), and the percentages were much the same in knees with and without bone attrition.
Characteristics of participants
Pain was reported in 84 knees (74%) with radiographic bone attrition compared with 505 knees (42%) without bone attrition. Figure 3 shows crude and adjusted associations of bone attrition with pain. In the crude analysis, the odds of pain were 3.92 times higher in knees with bone attrition compared with knees without attrition (95% CI 2.37 to 6.48). After adjustment for age, gender, body mass index, K/L score and the presence of joint effusion, the OR was 2.22 (95% CI 1.29 to 3.80). Figure 4 shows associations separately for knees with small and moderate bone attrition compared with knees without bone attrition. Crude and adjusted ORs were similar, CIs wide and tests for interaction between estimated OR and extent of bone attrition negative. Figure 5 shows separate estimates of the association of bone attrition with day pain and with night pain. In crude and adjusted analyses, ORs were more pronounced for day pain but not for night pain, with positive tests for interaction between estimated OR and type of pain. In the adjusted analysis the OR was increased for day pain (OR 2.37, 95% CI 1.48 to 3.80) but not for night pain (OR 0.94, 95% CI 0.58 to 1.53).

Association between presence of bone attrition and knee pain, stiffness and disability. Analyses of knee pain and stiffness were performed in 1326 knees and analyses of disability in 656 participants. *Analyses were adjusted for gender, age, body mass index, Kellgren-Lawrence score and presence of joint effusion.

Associations of bone attrition with knee pain according to extent of bone attrition. All analyses were adjusted for gender, age, body mass index, Kellgren-Lawrence score and presence of joint effusion. Only one knee with severe bone attrition was included in the study and therefore associations in knees with severe bone attrition could not be estimated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Associations of bone attrition with day pain and night pain separately. *Analyses were adjusted for gender, age, body mass index, Kellgren-Lawrence score and presence of joint effusion.
Stiffness was reported for 85 knees with bone attrition (75%) and 437 knees without (36%). The OR for the association of bone attrition with stiffness was 5.20 in the crude analysis (95% CI 3.09 to 8.75) and 3.23 after adjustment (95% CI 1.85 to 5.64, figure 3). ORs of stiffness were similar for knees with small bone attrition and those with moderate bone attrition, CIs wide and tests for interaction between estimated OR and extent of bone attrition negative (figure 4). Disability was assessed at the participant level and reported by 40 individuals with bone attrition (50%) and 140 individuals without (24%). The OR for the association of bone attrition with disability was 3.11 in the crude analysis (95% CI 1.93 to 5.02) and 2.09 after adjustment (95% CI 1.19 to 3.68, figure 3). ORs of disability were similar for knees with small bone attrition and those with moderate bone attrition, CIs wide and tests for interaction between estimated OR and extent of bone attrition negative (figure 4).
Attendees were more likely than non-attendees to report pain (71% vs 29%), stiffness (68% vs 32%) and disability (58% vs 42%). A total of 1765 attendees with 3530 knees underwent radiographic examination (65%) and films of 3100 knees were read (88%). Those with knee films available were more likely than those without films to report pain (88% vs 12%), stiffness (89% vs 11%) and disability (79% vs 21%). Among participants with knee films, those with complete clinical data were again more likely than those without films to report pain (80% vs 20%), stiffness (81% vs 19%) and disability (78% vs 22%).
Discussion
This analysis of adults aged ≥35 years shows that the presence of bone attrition found on plain x-rays is associated with 2–3-fold increased odds of pain, stiffness and disability. In both crude and adjusted analyses the associations were pronounced for day pain but not for night pain. When the associations were determined separately for grades 1 and 2 bone attrition we found similar increases in the odds of pain, with widely overlapping CIs and negative tests for interaction between extent of attrition and association with knee pain.
The strengths of the study include the large number of people involved, the population-based recruitment of study participants, their transparent pathway to clinical and radiographic examination15 and the fact that the x-rays were assessed by a single observer. However, there are four major limitations to the study. First, it is purely cross-sectional, which implicitly prevents us from drawing any conclusions about the causality of observed associations. Second, pain was only assessed as present or absent at the time at which the x-rays were obtained and we could not determine the association between bone attrition and pain intensity. Third, our analysis is based on individuals experiencing hip or knee pain in the community and cannot necessarily be generalised to other settings. Finally, participants in the study did not undergo MRI examination so we were unable to account for other pathologies including meniscal damage, bone marrow lesions or bursitis. Since subchondral bone marrow lesions are associated with bone attrition in MRI,21 the observed association of bone attrition with pain might be partially confounded by bone marrow lesions undetected on conventional x-rays.
The range of causes for knee pain in adults is large, ranging from local problems such as trauma and arthritis to referred pain from the hip or central pain sensitisation problems.22 The usual diagnosis established as a cause for knee pain in those aged ≥45 years in daily practice is OA,23 which is unsurprising in view of the high prevalence of patients with clinical and radiographic signs of OA.24 However, the association of bone attrition as assessed on conventional x-rays has only been partially explored, and its association with stiffness and self-reported disability has never been addressed to our knowledge. Despite the advent of MRI studies in patients with knee OA to investigate bone pathologies,9 25 26 it is too expensive for routine use and is unlikely to become part of clinical practice in patients with OA in many healthcare settings other than cases of suspected meniscal tears. Our study contributes to widening the focus when interpreting conventional x-rays from exclusive attention to joint space narrowing and osteophytes to a more integrated view which also involves subchondral bone. The approach of using conventional AP x-rays to detect bone attrition14 is cheap, simple and applicable to population-based research and clinical practice.
Pioneering work on the association between bone pathologies and pain was undertaken by Arnoldi et al27 28 in the 1970s and 1980s using intraosseous pressure measurement and other techniques. In the 1990s, bone scintigraphy was used to determine whether subchondral bone activity was related to both pain and progression of OA,29,–,31 providing an impetus to bone research in OA. In the last decade, MRI studies tell a similar story with associations found between bone marrow lesions or bone attrition and knee pain.9 26 32 33 Distinguishing between day and night pain, Hernández-Molina et al32 found an association of bone attrition with day pain but not night pain. In agreement with Hernández-Molina et al32 but contrary to our earlier suggestion that bone attrition could be associated with night pain,14 we found a strong association of bone attrition with day pain but none with night pain in the adjusted analysis. Taken together, a variety of techniques has been used during the last 40 years to explore the association between bone pathologies and pain but, to our knowledge, this is the first study to use conventional x-rays for assessing bone attrition in a large population-based sample and to determine the association of bone attrition, not only with pain but also with stiffness and disability. These three measures of disease severity are likely to be interrelated, and both pain and stiffness may be on the causal pathway between bone attrition and disability. This could be partially addressed by including either of the two measures as independent variables in the logistic regression model. In our study the crude OR for the association between bone attrition and disability of 3.11 (95% CI 1.93 to 5.02) became somewhat less pronounced after adjusting for knee pain (OR 2.75, 95% CI 1.69 to 4.47) and stiffness (OR 2.45, 95% CI 1.50 to 4.02).
MRI studies suggest that many knees with mild radiographic OA without joint space narrowing have some evidence of bone attrition.33 Several interrelated observations deserve further attention. First, malalignment of the knee was found to be associated with the prevalence and incidence of subchondral bone attrition in a compartment-specific manner.34 Second, bone marrow lesions were associated with and predictive for subchondral bone attrition.21 26 Third, subchondral bone attrition was strongly associated with cartilage loss within the same subregion of the knee.35 Taken together, this may suggest a sequential process with overload due to malalignment causing bone marrow lesions first which, in turn, lead to weakening of the subchondral osseous plate and eventual bone attrition and subsequent damage of the cartilage.
There are implications of our findings, both for research and clinical practice. The data suggest that we need to investigate subchondral bone changes as well as articular cartilage when studying the pathogenesis of both joint damage and pain in OA. Bone loss of the sort detected by our method implies serious damage to subchondral bone; this may be a critical feature in the sequential disease process and it may be more important to focus on the subchondral bone rather then the joint cartilage when developing novel potentially disease-modifying drugs for OA.
In conclusion, we found bone attrition detected on conventional AP x-rays using a simple and cheap technique14 associated with the presence of day pain, stiffness and disability in participants of a population-based study of individuals with knee OA.
Acknowledgments
The authors thank all study participants and the partners and staff of participating general practices for their support and interest in the study. The authors are indebted to the whole of the Somerset and Avon Survey of Health research team: Kirsty Alchin, Ros Berkeley-Hill, Jane Brooks, Hilary Brownett, Phil Chan, Clare Cross, Catherine Dawe, Cathy Doel, Jenny Eachus, Helen Forward, Matthew Grainge, Fiona Hollyman, Sue Jones, Helen Moore, Kate Morris, Nicky Pearson, Brian Quilty, Chris Smith, Lynne Smith, Gwyn Williams, Mark Williams and Andrea Wilson; and Allan Douglas and Doreen Cook at Dillon Computing. Finally, we are grateful to our co-investigators, Jenny Donovan, Tim Peters and Stephen Frankel. The Department of Social Medicine is the lead centre for the MRC Health Services Research Collaboration. The authors are grateful to Pete Shiarly for the management and maintenance of the database.
References
Footnotes
-
Funding The Somerset and Avon Survey of Health was originally funded by the Department of Health and the South and West NHS Research and Development Directorate. This work was funded by the Swiss National Science Foundation (grants nos 3233-066377 and 3200-066378) and by the British Arthritis Research Campaign. The funding bodies had no role in the design or conduct of the study; collection, management, analysis or interpretation of the data; or preparation, review or approval of the manuscript. SR is the recipient of a Research Fellowship from the Swiss National Science Foundation (grant number PBBEB-115067) and of an educational grant from the Swiss Society of Rheumatology.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the local research ethics committees of Somerset and Avon and all participants provided written informed consent.
-
Provenance and peer review Not commissioned; externally peer reviewed.