Article Text

Abstract
Background/aims: Childhood cognition predicts adult morbidity and mortality, potentially working through health behaviours. This study investigates if childhood cognition influences life course (i) non-drinking and (ii) binge drinking and pathways through which this might act—namely, childhood behaviour problems, adult social position and educational qualifications.
Methods: Prospective cohort of British births in March 1958, with information on cognition at 7, 11 and 16 years and alcohol use at 23, 33 and 42 years. Non-drinkers drank “infrequently/on special occasions” or “never”. Binge drinkers consumed ⩾10 units/occasion (men) and ⩾7 units/occasion (women).
Results: Lower cognitive ability increased the odds of non-drinking at each adult survey (for example, for men at 42 years OR 1.52 (95% CI 1.34 to 1.72) per SD decrease in 7-year maths). Associations remained after adjustment for pathway factors (i) behaviour problems, (ii) adult social position and (iii) educational qualifications. Decreased ability rank across childhood (7–16 years) also increased odds of non-drinking at 42 years, but the association operated via pathway factors. Lower 7-year ability elevated the odds of 42-year binge drinking, operating via pathway factors. Declining ability rank across childhood also increased the odds of adult binge drinking; associations operated through behavioural problems, adult social position and qualifications. In women, the decline in risk of binge drinking from an age 23-year peak to 42 years was associated with higher 7-year score.
Conclusions: Poorer childhood cognition was associated with non-drinking and binge drinking up to the early 40s. Associations between childhood cognition and drinking status may mediate between childhood cognition and adult health.
Statistics from Altmetric.com
Childhood cognition, as indexed by IQ-type test scores,1 has been shown to predict adult morbidity2 and mortality risks into the fifth3 4 and even seventh5 6 decades of life. One potential pathway linking childhood cognition with adult health is receptiveness to health behaviour messages (preventive health). More highly educated people tend to engage less often in harmful behaviours, such as smoking and heavy drinking.7 Childhood cognition is associated with adolescent initiation of health behaviours, but its role in persistence is less clear. Two studies report associations between childhood cognition and smoking; participants with higher cognitive ability were less likely as adults to have ever smoked2 and more likely to quit smoking decades later.8 The contribution of childhood cognition to persistence of other behaviours, including alcohol misuse, is unclear. By mid-life both heavy episodic drinking and non-drinking are associated with poorer health than regular lighter drinking.9 Binge drinking in early adulthood is associated with accident and violence-related morbidity and is a current policy concern.10 11 Non-drinkers are reported to have poorer mental12 and physical health,13 although uncertainties remain about the direction of association (this may be confounded to some degree by past drinking history14 and social disadvantage15).
Childhood cognition may directly influence alcohol initiation and persistence, or act as a marker for later qualifications and social position, which in turn influence adult drinking. In Britain and elsewhere, adolescence and early adulthood is the life stage when alcohol use becomes legal, when sensible drinking limits are likely to be exceeded and when average alcohol consumption peaks.16 It is also the stage when highest educational qualifications are achieved. Poorer school performance predicts drinking initiation, increased frequency and higher alcohol consumption17 and heavy drinking between adolescence and early adulthood.18 Thus we might expect cognitive growth throughout childhood, not just at adolescence to influence drinking patterns.
We use prospective data to examine associations between childhood cognitive ability (also referred to here as cognition) and adult binge drinking and non-drinking. To this end we investigate two domains of ability important in daily life—maths and reading. Based on correlations between different factors underlying general ability or “g”, maths and reading are likely to be correlated with “g” but with each contributing additional information.19 We assess whether childhood cognitive development indicated by repeated tests over time—that is, cognitive trajectories, are related to adult binge drinking and non-drinking. Specifically, we investigate whether:
cognitive ability at separate childhood ages influences (i) non-drinking and (ii) binge drinking at different adult ages
cognitive trajectories in childhood influence non-drinking and binge drinking at different adult ages
cognitive trajectories in childhood influence the persistence of binge drinking over time in adulthood
associations between childhood cognition and adult non-drinking or binge drinking operate through their influence on educational level or occupation in adulthood.
METHODS
Study sample
Data are from the 1958 British birth cohort, a prospective population-based study of all births during one week in March 1958 (some 17 000 live births) in England, Scotland and Wales. Participants were followed through childhood to their 40s. At 42 years 11 419 participants responded to the survey (70.3% of the target sample).20 Ethical approval for the 42-year survey was obtained from the North Thames multi-centre research ethics committee.
Measures
Alcohol use Participants were classified as non-drinkers or binge drinkers using self-reported data on usual drinking frequency (ranging from “never” to “on most days”), and amount consumed in the past week at three adult ages; 23, 33 and 42 years. Approximately 5% of participants at each survey reported “never” drinking, but most of these reported drinking on previous surveys. Therefore non-drinkers were defined as those drinking on “special occasions/rarely” or “never”. Total number of drinks was recorded at each survey, separately for wine, beer, spirits and martini/sherry and converted into standard units (1 unit is 10 ml or 8 g ethanol).21 At 42 years, “alcopops” were included to keep pace with changing habits. Total number of units was divided by usual frequency of drinking. Using British guidelines, men consuming ⩾10 units/occasion and women consuming ⩾7 units/occasion were categorised as binge drinkers.
Childhood cognition was indexed by age-appropriate maths tests conducted at school. The age 7 test comprised arithmetic problems of graded difficulty (range 0–10). The 11-year test was a modified version of Vernon graded arithmetic test (range 0–40).22 A maths comprehension test (range 0–31) was constructed at the University of Manchester for the 16-year survey.23 Reading tests at 7, 11 and 16 years were also used.24
Childhood behavioural adjustment, indicated by the Bristol Social Adjustment Guide at age 7 and Rutter scale at age 16, was categorised as normal (bottom 50%), intermediate (37%) or poor (top 13%).25
Social position was grouped by Registrar General classification using (i) father’s occupation at birth (or at 7 years if missing) and (ii) current or most recent occupation at 33 years (or 23 years if missing). Occupational categories were: I&II professional; III non-manual; III manual; and IV&V unskilled manual (no male head of household at birth was grouped with IV&V).
Educational level was represented by qualifications reported at 33 years, categorised as none; <O-level; O-level; A-level; higher qualification, broadly equivalent to no qualifications; <grade 10; grade 10; high school diploma/grade 12; and >high school diploma.
Analyses
Maths scores at 7, 11 and 16 years were approximately normally distributed, but were transformed to z-scores (genders together) allowing the relative position, or rank, of individuals to be compared across the three ages. Coding of z-scores was reversed; a negative z-score corresponds to a high test result and a positive z-score to a low result. We examined graphs of drinking and maths z-scores to investigate the linearity of associations. For aim one we used logistic regression to assess associations between maths z-scores separately at 7, 11 and 16 years, and drinking outcome (non-drinking and binge drinking) at 23, 33 and 42 years. For aim two we investigated the association between individual’s maths trajectories and drinking outcome separately at each adult age. To summarise an individual’s maths trajectory, 7–16 years, we estimated the intercept and slope of the z-scores using repeated measures multilevel models (in MLwiN 2.0).26 In these models, the intercept (level) represents the initial (7-year) z-score, and slope the change in maths rank, 7–16 years. The slope coefficient was multiplied by nine to correspond to the 9-year period. We assumed that change between 7, 11 and 16 years was linear; using three time points a non-linear change could not be reliably estimated. The predicted level and change for maths z-scores were used as independent variables in logistic regression to estimate the odds of non-drinking (or binge drinking) separately at 23, 33 and 42 years. Change in z-score relates to change in rank of ability relative to peers rather than an absolute change. Logistic regression models were adjusted for social position at birth (as a potential confounder) and for behavioural problems at ages 7 or 16 years (as a potential confounder or mediator). For the third aim changes in the associations between level and change in maths scores and binge drinking across adulthood were tested in a repeated measures multilevel model (in MLwiN 2.0). The outcome was binge drinking at 23, 33 and 42 years, and the model included level and change in maths, adult time-point and interactions of (i) time-point with maths level and (ii) time-point with maths change. Finally, to establish whether childhood cognition influenced adult drinking behaviour through its association with later qualifications or occupational position, we performed analyses with and without adjustment for these factors.
Analyses were repeated using reading test scores (ages 7, 11 and 16 years), and the patterns of results were similar to those observed for maths (data not presented).
The samples used in analyses differed, being smallest for 42-year outcomes. To investigate sample representativeness, we compared social class at birth in the original sample (n = 16 969) to the sample with information on maths intercept and slope, social position of origin, 16-year Rutter score, adult qualifications, social class and drinking at 42 years (n = 7400). The original sample included 17.0% in RG classes I&II compared to 19.0% in the 42-year analysis sample; 24.3% were in classes IV&V compared to 21.1% at 42 years.
RESULTS
A substantial minority of men and women were non-drinkers, for example 12% and 23% respectively at 42 years (table 1). Most non-drinkers (87% men and 81% women) at one adult survey reported drinking on at least one other adult survey (data not presented). Prevalence of binge drinking peaked at 23 years declining thereafter, and was about twice as common in men as women: 60% and 36% respectively were binge drinkers for at least one adult survey. Over the 9-year period, 7–16 years, 18% boys and 12% girls improved their maths rank (represented by a negative z-score) ⩾1 standard deviation (SD), whereas 13% boys and 20% girls declined in rank (that is, increased z-score) by ⩾1 SD (table 1).
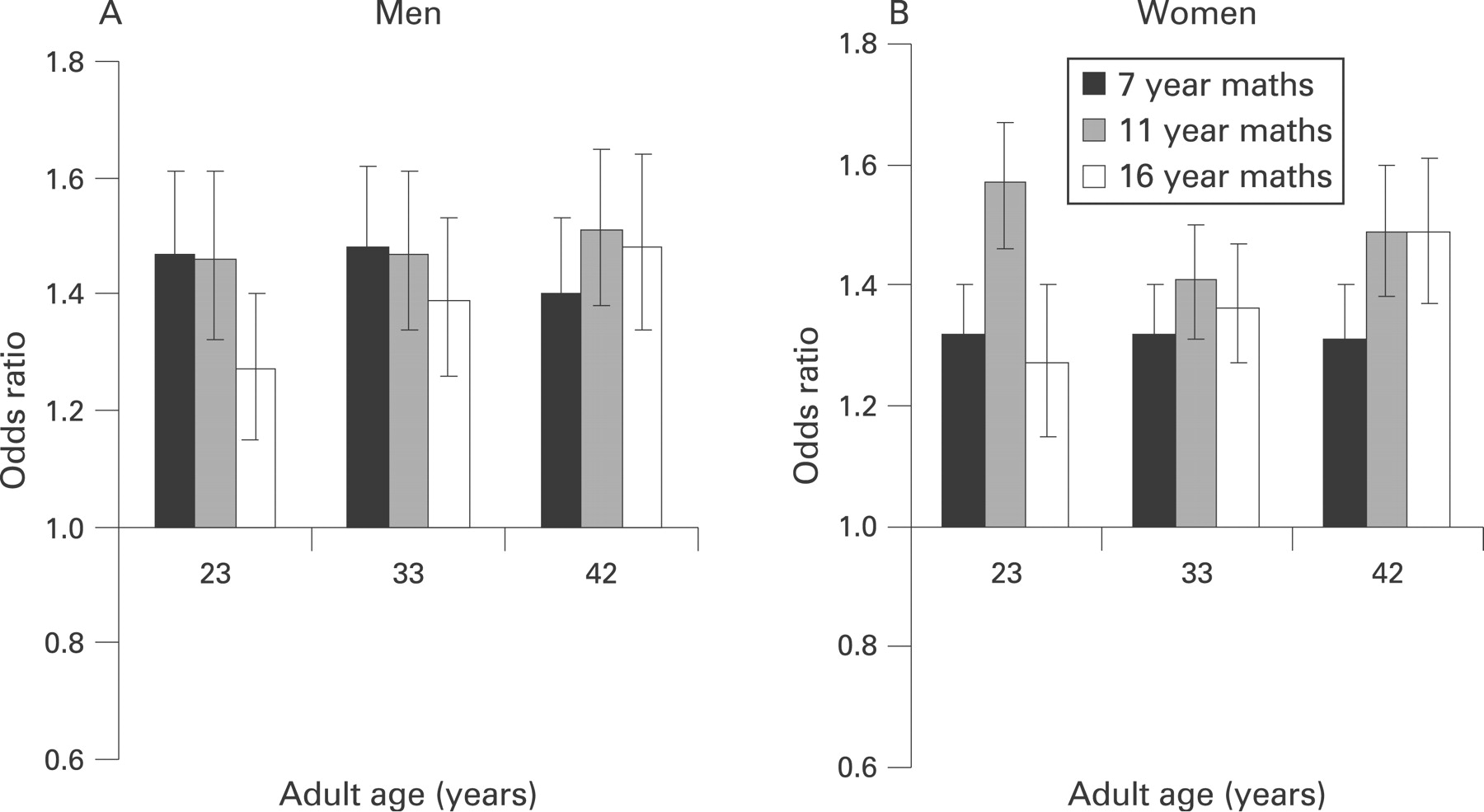
Figure 1 shows significant associations between maths scores at each childhood age and non-drinking at each adult age. The excess in odds of non-drinking associated with 1-SD decrease in maths ability (an increase in z-score) was about 40% for men and varied between 30–60% for women. For binge drinking, among men, there was an excess in the odds of binge drinking of 10–20% associated with a 1-SD decrease in maths ability at 11 and 16 years, but no association with maths at age 7 (fig 2). In contrast, for women, a 1-SD decrease in maths ability at each age was associated with about a 10% reduction in odds of binge drinking at 23 years, no association for 33 years, and 10–40% excess odds at 42 years (fig 2). Table 2 presents odds ratios (ORs) for non-drinking associated with level (z-score at 7 years) and change (to age 16), simultaneously. A 1-SD decrease in initial ability level was associated with an increase of about 50% in the odds of being a non-drinker in adulthood, attenuated on adjustment for social position at birth to, for example, OR 1.41 (95% CI 1.23 to 1.61) for 23-year non-drinking in men (table 2). Adjustment attenuated ORs at ages 23, 33 and 42 years similarly, the greatest attenuation was for non-drinking at 23 years in women: OR 1.47 (1.36 to 1.60) per SD decrease 7-year maths ability attenuated to 1.40 (1.29 to 1.52). Adjustment for behaviour problems at age 7 had a negligible effect on the ORs in table 2, although associations between maths and non-drinking were attenuated on adjustment for 16-year behaviour. An association between 7-year maths and non-drinking persisted after adjustment for adult qualifications and social position but estimates were reduced. Participants whose maths rank declined during childhood had raised odds of non-drinking at age 42, although associations were fully mediated in adjusted models (table 2). Lower initial level and decline in maths rank were significantly associated with lower adult qualifications and social position (data not presented). Analyses presented in table 2 were repeated for “never drinkers” compared to occasional drinkers and more frequent drinkers. Patterns of association were similar to those in table 2, although estimates were slightly weaker with wider confidence limits.


{kind=link}
{kind=link}
Table 3 shows that for men, 7-year maths level was unrelated to binge drinking at 23 and 33 years. While a 1-SD decrease in 7-year ability was associated with a 10% increase in the odds of 42-year binge drinking, this was mediated by adjustment for 16-year behavioural problems, adult qualification level and social position. However changes in rank were associated with binge drinking at all adult ages for men: a reduction in maths rank (7–16 years), increased the odds by 14–24%, attenuating after adjustment for behavioural problems, later qualifications and social position. For women, a decrease in 7-year maths level was associated with a 12% reduction in odds of binge drinking at 23 years, but with a 24% increase at 42 years. Associations attenuated after adjustment for qualifications and social position. A 1-SD decline in maths rank (7–16 years) was associated with a 11–19% increase in odds of binge drinking at 33 and 42 years, but after adjustment for qualifications the association remained significant only at 42 years. For men, neither 7-year maths nor change in rank was associated with changes in binge drinking between 23 and 33, or 23 and 42 years. For women, a multilevel repeated measures model confirmed that relative to those with lower 7-year ability, women with higher 7-year ability were less likely to binge drink at 42 years compared to 23 years. Differences reduced on adjustment for later social position or qualifications.
DISCUSSION
The main finding is that childhood cognition was associated with both non-drinking and binge drinking in adulthood. However there were important variations in the associations observed. In analyses adjusted for childhood behaviour problems, adult social position and qualifications, poorer cognition in early childhood was associated with non-drinking over two decades in early adulthood, in both men and women. Decreasing ability rank across childhood was associated with raised odds of binge drinking at 23 and 33 years in men; in contrast, for women the association was evident at 42 years. Our results indicate that women with lower ability had decreased odds of binge drinking in their 20s, but increased odds in their 40s. To our knowledge this is the first study to examine cognitive trajectories, adult socioeconomic position and drinking behaviours and in this respect adds important information to existing literature. We acknowledge that cognition is one of many influences on drinking behaviour, including macro-level influences such as price and availability, as well as individual-level influences, notably ethnicity, demographic and psychosocial factors.27 Our focus on cognition is justified by the need to understand how the recently documented link between childhood cognition and adult health2 6 arises.
Methodological considerations
This study benefits from prospective data on a nationally representative birth cohort in a cultural setting in a particular location and time where alcohol use is the norm. The long follow-up and repeated cognitive measures extends previous work, firstly, by investigating both level and change in cognitive ability and, secondly, by examining drinking trajectories further into adulthood than most other studies. Other research investigating childhood ability and adult drinking focuses on problem drinking,28 average amount,29 beverage preference30 or alcohol-induced hangovers,31 and does not examine change in cognitive ability, potential confounding by childhood social position and behavioural adjustment or mediation through adult education and occupation. In our study, cognitive trajectories were estimated for participants with incomplete data, although models may be imprecise because only three time-points are available. Results are presented for maths ability, but similar patterns were observed for reading which is unsurprising given that the test scores are correlated and are both likely to reflect underlying general ability. Self-reporting of drinking incurs error, although a quantity and frequency approach with separate questions for different types of beverage improves recall.32 A broad definition for non-drinking (drinking on special occasions or “never”) indicated habitual non-consumption rather than a more restrictive definition “never” having drunk. “Never” drinkers include many past drinkers and the true prevalence of abstention is likely to be exceedingly low in the United Kingdom.33 Nevertheless, results for “never” drinkers showed similar patterns to results for “non-drinkers.” Definitions of binge drinking are debated and are inconsistent across existing literature.11 We defined binge drinking using data on frequency and amount of alcohol use in the absence of direct questions on amount per occasion. While this study benefits from a “usual” drinking frequency measure, the amount consumed is based on the past week and fluctuations in intake will affect identification of binge drinkers.34 Reporting of alcohol intake may be biased in relation to cognition and we cannot discount the possibility that individuals with greater cognitive ability may be more likely to report moderate consumption.
Childhood cognition and adult drinking
We investigate maths ability, which is a key skill in daily life, and in this dataset like many others, maths is positively correlated with reading and general ability measures.35 Our findings that lower childhood ability increased the odds of adult binge drinking builds on evidence that initiating alcohol use is strongly related to educational success or failure: children with lower ability or aspirations are more likely to start drinking.11 36 Associations between lower childhood ability and higher odds of both non-drinking and binge drinking in adulthood were largely independent of social background, even though manual origins are associated both with lower cognitive ability and higher risks of adult non-drinking and binge drinking. Our findings fit with observations of non-linear associations in which adult non-drinkers and heavier drinkers have lower adult ability scores,37 education15 or occupational position.38 Lower ability at each point in childhood was associated with greater odds of non-drinking throughout adult life congruent with reports that non-drinking is more prevalent in less educated and manual social groups.38 39 The association of non-drinking with initial ability persisted through adulthood with no additional contribution of 7–16-year change in cognitive ability. However, associations between binge drinking and initial ability were mediated by later social position and qualifications, whereas associations with change in ability were more consistently observed. Our results agree with a study showing that adult social position mediated an association between lower 11-year IQ and raised risk of alcohol-induced hangovers (a proxy for binge drinking) at age 44–52 in a retrospective cohort.31
It could be argued that behaviour and personality factors confound associations between childhood cognition and adult drinking. Yet, adjustment for 7-year behaviour negligibly affected associations between cognitive ability and non-drinking or binge drinking, suggesting that early behaviour was not an antecedent of cognitive trajectories which in turn influenced adult drinking. However, stronger attenuation on adjustment for 16-year behaviour suggested mediation of associations between cognition and adult binge drinking, and to a lesser degree, for non-drinking. This fits with evidence that initiating binge drinking is more frequent in adolescents with behavioural problems.36
Initial ability at age 7 and changes across childhood may reflect accumulation of subtly different childhood exposures. Initial ability reflects both genetic potential and environmental influences, such as learning experience and social background. Ability trajectories (change relative to peers) will be influenced by changing home circumstances, type of school or engagement with school and may better reflect cumulated childhood experiences.40 Ability trajectories may also be particularly important for longer-term socioeconomic and demographic pathways into adulthood and, interestingly, as demonstrated here, are associated with adult health behaviours.
Persistent binge drinking is important because of health and social harms that accrue to binge drinkers and those around them. For women, higher 7-year ability rank was associated with change in adult binge drinking trajectories (towards non-bingeing). The decreased risk of persistent binge drinking with higher ability operated through adult circumstances. While, for men, change in individual binge drinking trajectories was not affected by early childhood ability or change in ability.
Our results indicate that in some instances there are lasting effects of early ability on adult drinking patterns in addition to the effect of childhood ability on social destinations. Cognitive trajectories influence educational and occupational pathways (higher achieving children are more likely to enter non-manual occupations). Associations between qualifications and occupation with adult health behaviours may reflect circumstances at that life-stage (deriving from work and home conditions—for example, (un)employment, financial problems, social support, partnership and parenthood transitions) or longer term accumulated experiences, attitudes and opportunities.41–43 Individuals with greater cognitive skills are more likely to possess material and personal resources which facilitate healthier behaviours. Social cognitive models of behaviour change propose that intentions, which are shaped by attitudes and norms, are proximate determinants of behaviour change. Studies of health behaviours indicate that specific knowledge of risks associated with certain behaviours is not a good predictor of behavioural change. However self-esteem and perceptions of control over drinking and perceiving many facilitators of drinking are particular predictors of binge drinking.44 If childhood ability is associated with development of self-esteem, attitudes, norms or intentions towards alcohol use, this may provide a pathway between childhood ability and adult drinking. In the United Kingdom social gradients are reported in attitudes and expectancies about health, and these in turn are associated with health behaviours.45
The associations between early ability and later binge or non-drinking suggest that influences from childhood are carried over to persistence of alcohol use in adulthood. In particular, initial level of maths ability was related to non-drinking and change in ability to binge drinking even after adjustment for adult qualifications and social position. A study of Danish men made comparable investigations using IQ in early adulthood: higher risks of adult non-drinking were associated with lower IQ, operating through adult socioeconomic position. IQ was not associated with heavy drinking, although heavy drinking prevalence was low.30
Our study provides insights into associations between childhood cognition and later adult health.2 6 Alcohol consumption may be on the pathway between childhood ability and later health and mortality risks. Our results also have implications for the ongoing debate about the role of alcohol in cognitive decline during adulthood.46 Few studies take account of early cognition and most reported associations between adult ability and alcohol use may be confounded by selection into alcohol use earlier in life rather than effects of alcohol exposure. Associations reported here may be specific to this particular generation of primarily white men and women. It is unclear whether the same patterns will be seen in future generations in different cultural and social settings with, for example, differing levels of social acceptability towards alcohol. None the less, our findings suggest that in contemporary British society, childhood ability contributes to the development of educational gradients in adult drinking and that effects may persist over several decades in adulthood. Thus, with regard to policy development to reduce binge drinking, the vulnerability of groups with poorer cognitive ability will need to be considered alongside evidence about macro-level and other influences.
What is already known on this subject
Initiation of alcohol use is associated with poorer cognitive ability in childhood. Also, adults with higher cognitive ability in childhood are at lower risks for a range of morbidity and mortality outcomes up to the seventh decade of life.
What this study adds
Poorer childhood cognitive ability was associated with higher odds of non-drinking in men and women, separate from effects of adolescent behavioural problems, adult qualifications and social position.
Declining cognitive ability trajectories across childhood were associated with increased odds of binge drinking through adulthood in men, separate from effects of adolescent behavioural problems, adult qualifications and social position. In women, the association of binge drinking with declining ability was accounted for by these factors.
Policy implications
Binge drinking is a current policy concern in several countries, including the UK, with policy interest in both individual and societal level influences. The vulnerability of groups with poorer cognitive ability and slower rates of cognitive gain throughout childhood to adverse drinking behaviour will need to be considered alongside evidence about macro-level and other influences.
Acknowledgments
Data acknowledgement: Centre for Longitudinal Studies, Institute of Education. National Child Development Survey Composite File including selected Perinatal Data and sweeps one to five (computer file). National Birthday Trust Fund, National Children’s Bureau, City University, Social Statistics Research Unit (original data producers). The Data Archive distributor, Colchester, Essex. SN:3148. 1994.
REFERENCES
Footnotes
Funding: BJ is supported by a Joint Medical Research Council/Department of Health Special Training Fellowship in Health of the Public Research. Research at the UCL Institute of Child Health and Great Ormond Street Hospital for Children NHS Trust benefits from R&D funding received from the NHS Executive. The funders did not have a role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Competing interests: None.
Linked Articles
- In this issue