Article Text

Abstract
Objectives Previous studies on the association between psychosocial work factors and blood pressure mainly focused on specific occupations or populations and had limited sample sizes. We, therefore, investigated the associations between psychosocial work factors and blood pressure in a large general working population in the Netherlands.
Methods We included 63 800 employees from the Netherlands, aged 18–65 years, with blood pressure measurements and a reliable job code at baseline. Psychosocial work factors (job strain, effort–reward imbalance (ERI) and emotional demands) in the current job were estimated with three recently developed psychosocial job exposure matrices. To examine the associations, regression analyses adjusted for covariates (age, sex, body mass index, education, monthly income, pack-years, smoking, alcohol consumption and antihypertensive medication (not included for hypertension)) were performed.
Results Higher job strain was associated with higher systolic blood pressure (SBP) (B (regression coefficients) (95% CI) 2.14 (1.23 to 3.06)) and diastolic blood pressure (DBP) (B (95% CI) 1.26 (0.65 to 1.86)) and with higher odds of hypertension (OR (95% CI) 1.43 (1.17 to 1.74)). Higher ERI was associated with higher DBP (B (95% CI) 4.37 (3.05 to 5.68)), but not with SBP or hypertension. Higher emotional demands were associated with lower SBP (B (95% CI) −0.90 (−1.14 to −0.66)) and lower odds of hypertension ((OR) (95% CI) 0.91 (0.87 to 0.96)).
Conclusions In the general working population, employees in jobs with high job strain and ERI have higher blood pressure compared with employees with low job strain and ERI. Emotional demands at work are inversely associated with blood pressure.
- occupational health
- hypertension
- blood pressure
Data availability statement
Registration is required to obtain data from the Lifelines cohort study. It is not permitted to deposit the Lifelines data in an open data repository. To obtain data, used in the current study, interested researchers should contact the Lifelines Cohort Study (www.lifelines.nl).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
High blood pressure may disrupt normal physiological function, which may lead to various diseases, such as stroke, coronary heart disease, peripheral arterial disease, chronic kidney disease, dementia, diabetes mellitus and erectile dysfunction.1 A recent study reported that, in 2017, globally, among the Global Burden of Diseases risk factors, high systolic blood pressure (SBP) was the leading risk factor accounting for 10.4 million deaths and 218 million disability-adjusted life-years.2 The mortality rate from ischaemic heart disease and stroke doubles with an elevation of 20 mm Hg SBP or 10 mm Hg diastolic blood pressure (DBP).3
Excess dietary salt, low dietary potassium, overweight and obesity, physical inactivity, excess alcohol consumption, smoking, low socioeconomic status and diabetes are modifiable risk factors for high blood pressure.4 In addition, psychosocial work factors are also considered as modifiable risk factors for high blood pressure.4 Workers may experience various adverse psychosocial conditions at work, like job strain, effort–reward imbalance (ERI) and high emotional demands. These working conditions may elevate blood pressure through stress-induced activation of the hypothalamic–pituitary–adrenal axis and through behavioural mechanisms, for example, poor diet, excess alcohol consumption, low physical activity as consequences of exposure to stressors.
The job demand-control model posits that job strain results from the combination of high psychological job demands and low job control.5 ERI characterises working conditions with a lack of reciprocity between efforts and rewards (eg, income, promotion or appreciation).6 Emotional demands at work refers to work-related tasks that require sustained emotional efforts due to interactional contacts with clients,7 such as dealing with patients with a terminal illness or aggressive customers.8 Previously, some studies suggested that job strain and ERI were associated with high blood pressure9 10 while some other studies found no such association.11 12 Most of these studies mainly focused on specific occupations (eg, hotel room cleaners) or populations (eg, females and patients with hypertension). Further, only very few studies have examined the association between psychosocial work factors that were not measured by individual-level self-reported data and blood pressure.13 Measuring psychosocial working conditions not by self-report by the participants, but by other measures, is important, as reporting bias is a major concern in psychosocial work environment studies.14 Therefore, there is a need for large-scale studies with precise estimates to understand this association better. In addition, nothing is known about the association between emotional demands at work and blood pressure in the general working population.
In this study, we investigated the associations between psychosocial work factors (job strain, ERI and emotional demands estimated with job exposure matrices (JEMs)) and blood pressure among 63 800 active workers in the Lifelines Cohort Study.
Methods
Population
This cross-sectional study was conducted using data from the Lifelines Cohort Study, a large observational population-based cohort study, which started in 2006 and aims to disentangle the role of genetic factors, lifestyle and the environment in the development of chronic diseases and healthy ageing. Residents of the three northern provinces of the Netherlands (Friesland, Groningen and Drenthe) were invited to participate in the study. Three generations of participants were recruited: the index participants (aged 25–50 years) through general practitioners and their family members (partners, parents and parents-in-law and children). The participants of the Lifelines Cohort Study are representative of the general population of the three northern provinces of the Netherlands.15 Recruitment stopped in December 2013 after including 167 729 participants (age range: 6 months to 93 years). The scientific rationale, study design and survey methods of the Lifelines Cohort Study have been described elsewhere.16 In this study, we included ‘active workers’ defined as individuals who held a job at baseline.
Blood pressure and hypertension
At baseline (2006–2013), blood pressure was measured in a quiet room with room temperature, using an automated device (DinaMap, PRO 100V2, GE Healthcare, Freiburg, Germany) after 10 min of rest. Blood pressure was measured every minute during a period of 10 min, and the average of the final three readings was recorded for SBP and DBP. Hypertension was defined as SBP ≥140 mm Hg or DBP ≥90 mm Hg or self-reported use of antihypertensive medication.
Psychosocial work factors
At baseline (2006–2013), job strain, ERI and emotional demands at work were estimated using three JEMs that were recently developed in Denmark. Details of the job strain JEM are described elsewhere.17 18 The construction of the ERI and emotional demands JEMs are provided in online supplemental appendix 1 and online supplemental table 1 and 2. Job strain and ERI were estimated by using predicted probabilities (ranging from 0 to 1) and emotional demands were estimated by the predicted level (ranging from 0 to 4). Higher values indicated a higher predicted probability/level of the psychosocial work factors.
Supplemental material
The three JEMs were linked to the Lifelines Cohort Study according to participants’ self-reported job title, sex and age at baseline. In the Lifelines Cohort Study, the job title was coded according to ISCO-0819 using a Computer-Assisted Structured Coding Tool (CASCOT).20 We converted ISCO-08 into ISCO-88 to incorporate the Danish JEMs in Lifelines. The CASCOT score indicates the probability that the given code is correct (range: 0–100). We selected participants with a CASCOT score ≥60, and all job titles were manually reviewed and, if necessary, recoded to achieve accurate job coding. We used a conversion table to convert ISCO-88 to DISCO-88 codes (Danish version of the ISCO-88). We used the 2005 JEM estimates as our baseline population was recruited between 2006 and 2013.
Covariates
The participants’ age, sex and body mass index (BMI) were taken from the baseline screening. Education, monthly income, smoking status, pack-years of smoking, alcohol consumption and use of antihypertensive medication were extracted from the baseline questionnaires. We included the following Anatomical Therapeutic Chemical codes of antihypertensive medication according to the Dutch Pharmaceutical list: C02 (antihypertensives), C03 (diuretics), C07 (β‐blocking agents), C08 (calcium channel blockers) and C09 (agents acting on the renin–angiotensin system).
Statistical analyses
We performed descriptive analyses for psychosocial work factors, blood pressure and covariates. To investigate the associations between psychosocial work factors and blood pressure, we used linear regression analyses both with and without adjustment for the covariates. For multicategorical covariates (eg, education), we created dummy variables. We conducted logistic regression with and without adjustment for the covariates (except antihypertensive medication) to investigate the associations between psychosocial work factors and hypertension. Psychosocial work factors were initially tested separately. Subsequently, we entered all psychosocial work factors in one model to estimate the independent effect of each psychosocial work factor. Furthermore, we investigated the combined effects of the psychosocial work factors on blood pressure. In doing so, first, we dichotomised each psychosocial work factor into a ‘low’ and ‘high’ group based on the median values. Then we created eight possible combinations: group 1 (all psychosocial work factors are low), group 2 (all psychosocial work factors are high), group 3 (high job strain and ERI, but low emotional demands), group 4 (high job strain and emotional demands, but low ERI), group 5 (high ERI and emotional demands, but low job strain), group 6 (only high job strain), group 7 (only high ERI), and group 8 (only high emotional demands).
A sensitivity analysis was conducted to examine the associations between psychosocial work factors and blood pressure adjusted for covariates in participants who did not use antihypertensive medication. In addition, we investigated the associations across different ISCO groups. SPSS V.25 (IBM Released 2017. IBM SPSS Statistics for Windows, V.25.0) was used for data analysis.
Results
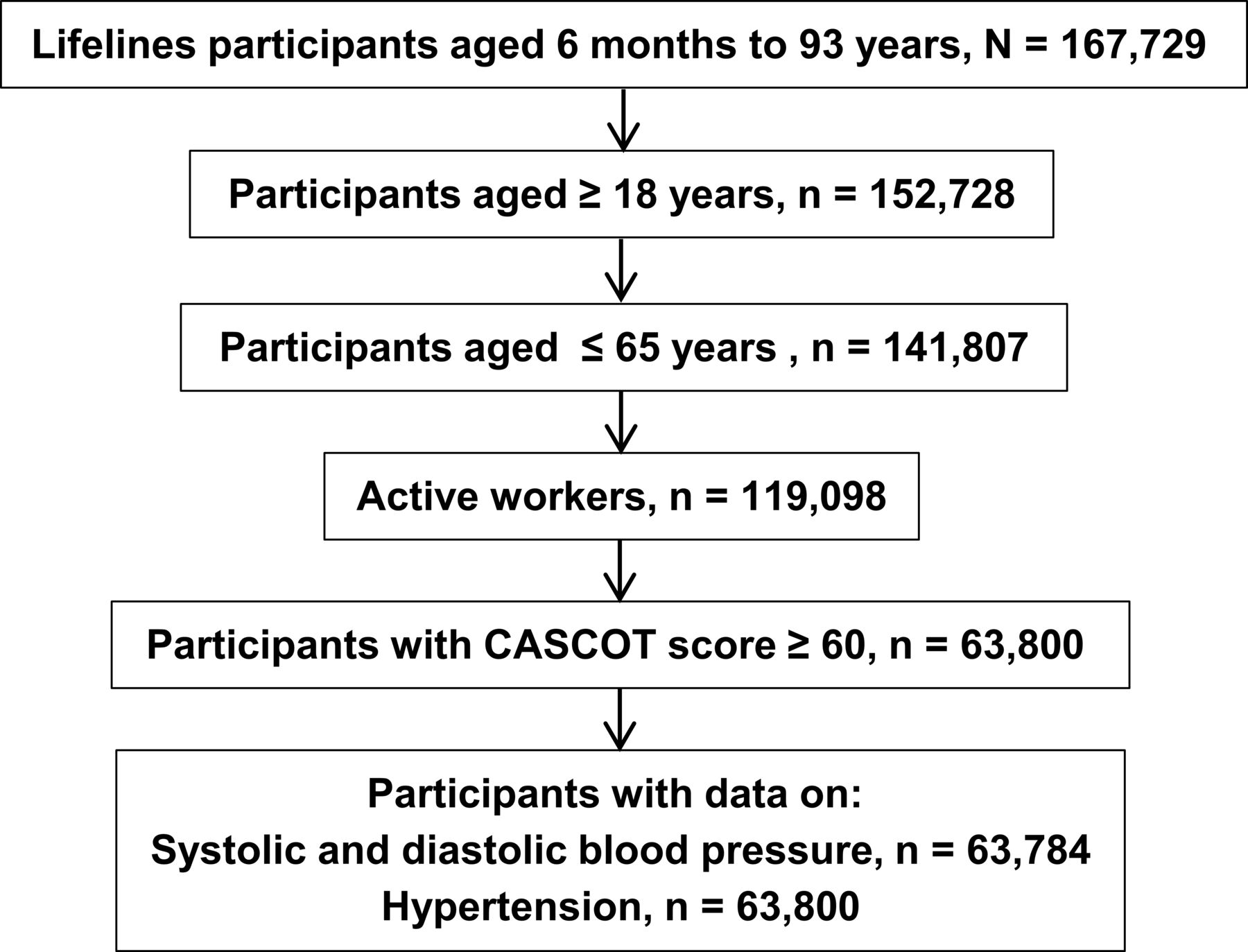
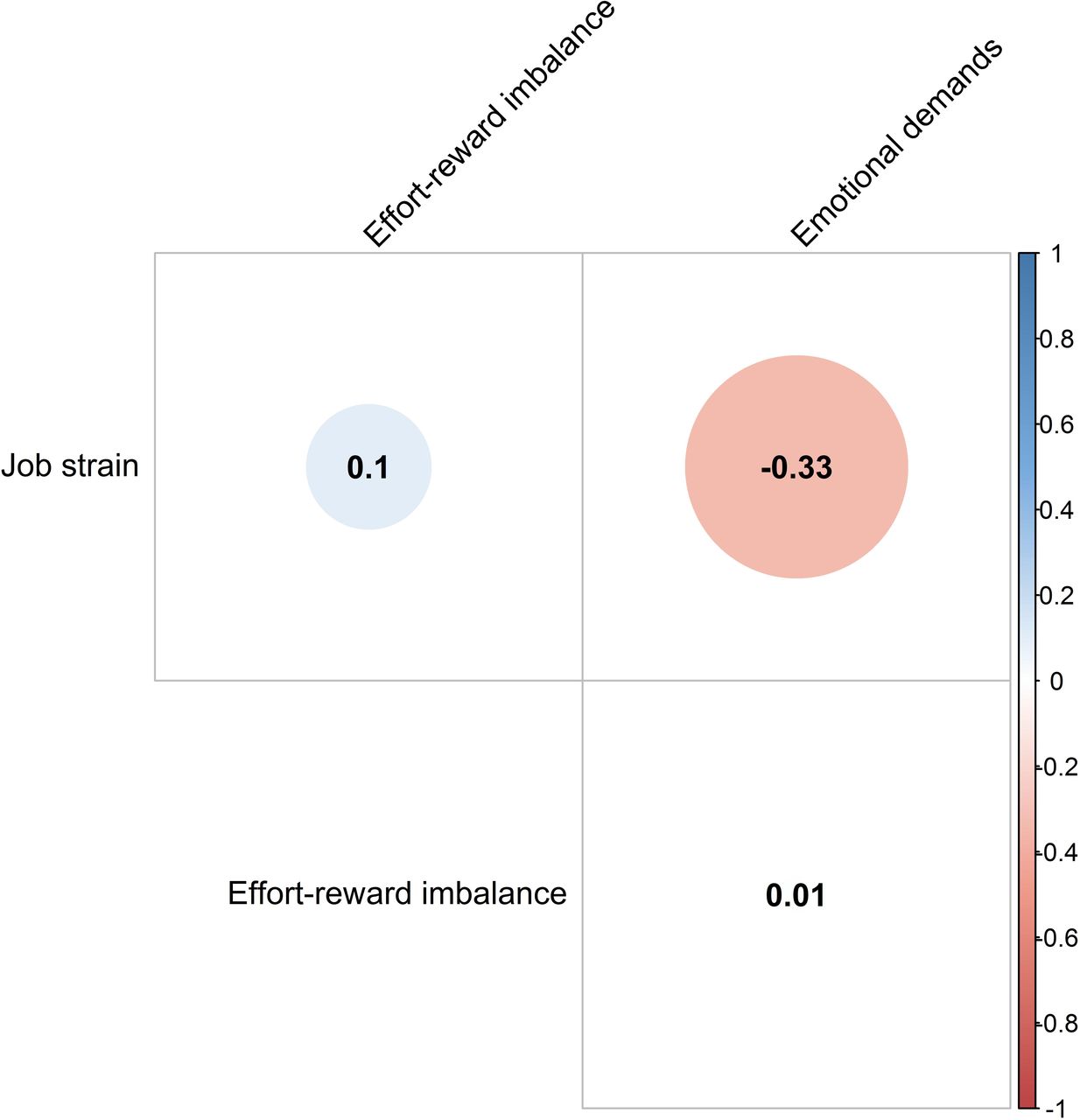
Figure 1 shows the selection of the study population. In the final analyses, we excluded 55 298 active workers with a CASCOT score <60. In the excluded group, there were approximately 6% less females than in the included group (table 1). Furthermore, we observed statistical significant but very small differences in all parameters between the included and excluded groups. The mean age of the study population (n=63 800) was 41.3 years (SD 10.5 years), most participants were female (59.3%), and the mean BMI was 25.7 (SD 4.2) (table 1). Approximately half of the participants had a medium education (52.4%) and a high net monthly income (47.6%). The mean alcohol consumption was 6 g/day (SD 9g/day), the median pack-years in ever smokers was 8 (IQR: 12), and almost half of the participants were never smokers. Approximately 7% of the participants reported using antihypertensive medication. In the entire study population (including participants using antihypertensive medication), the mean SBP and DBP were 124 mm Hg (SD 14) and 73 mm Hg (SD 9), respectively, and the prevalence of hypertension was 19.7%. The Pearson correlation between the psychosocial work factors is shown in figure 2. A negative correlation was found between job strain and emotional demands (r=− 0.33). No substantial correlation was observed between job strain and ERI (r=0.10) and between ERI and emotional demands (r=0.01).

Flow chart towards the final study participants. CASCOT, Computer-Assisted Structured Coding Tool.
Comparison of covariates and blood pressure between included and excluded active workers

Correlogram shows the Pearson correlation between psychosocial work factors.
Association between psychosocial work factors and blood pressure
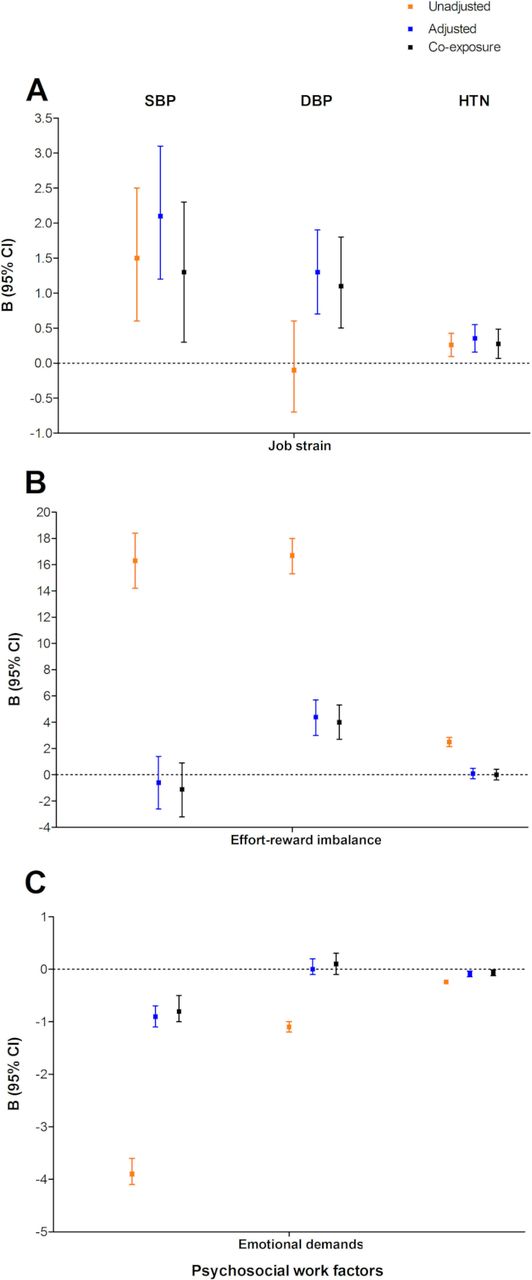
Figure 2 and online supplemental table 3 show the association between psychosocial work factors and blood pressure. In the adjusted models, a higher predicted probability of job strain was statistically significantly associated with a higher SBP (B (regression coefficients) (95% CI) 2.14 (1.23 to 3.06)) and DBP (1.26 (95% CI 0.65 to 1.86)) and with higher odds of hypertension (OR (95% CI) 1.43 (1.17 to 1.74)). A higher predicted probability of ERI was associated with a higher DBP (4.37 (95% CI 3.05 to 5.68)), but no association was found with SBP (−0.61 (95% CI –2.60 to 1.38)) and hypertension (1.09 (95% CI 0.73 to 1.62)). Finally, a higher predicted level of emotional demands was associated with a lower SBP (−0.90 (95% CI –1.14 to −0.66)) and a lower odds of hypertension (0.91 (95% CI 0.87 to 0.96)); no association was found between a higher predicted probability of emotional demands and DBP (0.01 (95% CI –0.15 to 0.17)). In the model with all psychosocial work factors, the risk estimates were comparable and remained statistically significant (figure 3 and online supplemental table 2). In the analyses using the combined psychosocial work factors, participants with high job strain, high ERI and low emotional demands had a higher SBP and DBP, and a higher odds of hypertension compared with participants with low job strain, low ERI and low emotional demands. The combination of high ERI, high emotional demands and low job strain was associated with a lower SBP and a higher DBP. Finally, the combinations of high job strain and high emotional demands (irrespective of ERI) were not associated with differences in blood pressure (table 2).

{kind=link}
{kind=link}
{kind=link}
Associations between psychosocial work factors and blood pressure. For all outcome parameters (SBP, DBP and hypertension) continuous B coefficients and 95% CI are given. The adjusted models (blue) are adjusted for age, sex, BMI, education, monthly income, pack-years, smoking, alcohol consumption and antihypertensive medication (not included for HTN). In the coexposure models (black), the three psychosocial work factors and all covariates are entered into one model. BMI, body mass index; DBP, diastolic blood; HTN, hypertension; SBP, systolic blood pressure.
The association between combinations of psychosocial work factors and blood pressure/hypertension
Sensitivity analyses
The sensitivity analyses among participants not using antihypertensive medication (n=51 231, mean SBP=123 mm Hg, SD (14), mean DBP=73, SD (9)) showed comparable findings with the main results (online supplemental table 4). We observed that the magnitude and direction of the association between psychosocial work factors and blood pressure differs across various working groups (online supplemental tables 5–7).
Discussion
Main findings
In this large population-based cross-sectional study, higher job strain was associated with a higher SBP and DBP, and a higher odds of hypertension. Higher ERI was associated with a higher DBP, while higher emotional demands at work were associated with a lower SBP and a lower odds of hypertension. Analyses including the three investigated psychosocial work factors in one model showed similar findings. Analyses using combinations of psychosocial work factors indicated that high job strain and high ERI were associated with higher blood pressure but the association between high job strain and higher blood pressure was not present in participants who also had high emotional demands.
Association between psychosocial work factors and blood pressure
We found that job strain (measured as a predicted probability ranging from 0 to 1) was associated with 2.1 mm Hg higher SBP, 1.3 mm Hg higher DBP and a 40% higher odds of hypertension per one unit increase in the predicted probability of job strain. A meta-analysis by Landsbergis et al showed that high job strain was associated with a 3.43 mm Hg higher SBP and a 2.07 mm Hg higher DBP compared with no or low job strain.21 In another meta-analysis, Babu et al found a higher odds (1.29, 95% CI (1.14 to 1.48)) of hypertension in workers with job strain compared with workers with no job strain.22 Gilbert-Ouimet et al, in a systematic review, reported deleterious effects of job strain on SBP (ranges: 2–10.2 mm Hg), DBP (ranges: 2–17.97 mm Hg) and hypertension (OR ranges: 1.18–2.90) compared with no job strain.23 Our study further strengthens the existing evidence that job strain is associated with higher blood pressure among active workers. As the risk of cardiovascular diseases (CVDs) increases progressively with each mm Hg increase of blood pressure from levels as low as 115 mm Hg SBP and 75 mm Hg DBP upward among participants aged ≥40 years,3 our results suggest that the potential risk of CVDs will be higher among our current study participants in job groups with a high predicted probability of job strain.
We found that ERI (measured as a predicted probability ranging from 0 to 1) was associated with a 4.4 mm Hg higher DBP, but not with SBP or hypertension. In a recent meta-analysis, Eddy et al reported that participants with ERI had a higher SBP, DBP and prevalence of hypertension compared with participants without ERI.24 Likewise, Gilbert-Ouimet et al reported that ERI was associated with a higher SBP (ranges: 1.86–4.52 mm Hg), a higher DBP (ranges: 1.31–4.17 mm Hg), and a higher odds of hypertension (OR ranges: 1.62–5.77).23 Our study thus strengthens the evidence for an association between high ERI and higher DBP. However, previous studies reported that workers on experiencing ERI had a higher SBP and a higher odds of hypertension,25 which we did not observe in this study. Unlike our study, the study samples of these studies represent a specific occupation or a specific group of employees (eg, white collar).25 In contrast, we examined the association in a large general working population with about 400 different job titles. Furthermore, we used a JEM for estimating ERI which was not used in the previous studies. Another difference concerns the measurement of blood pressure: some studies measured ambulatory blood pressure while others measured on spot blood pressure. These methodological differences, thus, might explain the differences in findings between our current study and the previous studies.
Possible mechanisms linking psychosocial work factors to higher blood pressure may include stress induced by these psychosocial work factors. The biological mechanism of how stress increases blood pressure is unclear. Stress at the workplace increases cortisol secretion.26 27 Hypersecretion of cortisol may result in hardening of the artery wall (known as ‘atherosclerosis’) by developing resistance to its anti-inflammatory properties and by disrupting the negative feedback system of the hypothalamic–pituitary–adrenal axis.28 29 In addition, an increased level of epinephrine and long-term sympathetic activation in response to work stress may contribute to the elevation of blood pressure by fostering atherosclerosis.30 31 Earlier, it was shown that high job demands might enhance the progression of carotid atherosclerosis.31
Another plausible biological mechanism through which psychosocial work factors could increase blood pressure might be stress-induced telomere (DNA–protein complexes that cap chromosomal ends, promoting chromosomal stability) shortening. Stress-induced telomere shortening is associated with cellular senescence (loss of a cell’s power of division and growth) which may accelerate cellular ageing.32 The shortening of telomeres plays an important role in the pathogenesis of atherosclerosis33 34 and a previous study reported that shorter telomere length was associated with a higher prevalence of hypertension.35
Finally, stress induced by psychosocial work factors may increase health-risking behaviour (eg, alcohol abuse, less physical activity, unhealthy diet, sleep disturbance, increased smoking intensity and reduced compliance with medical treatment),36 37 which in turn may increase blood pressure among workers.
Somewhat unexpectedly, we found that participants in occupations with high emotional demands had a lower SBP and lower odds of hypertension. Recent studies found a strong association between emotional demands and diabetes, sleep disorders and arthritis among workers.38 Our study is the first of this kind to investigate the association between emotional demands and blood pressure. More studies are required to disentangle this association.
One possible explanation of our unexpected findings could be that jobs with high emotional demands (eg, nurses, care workers and social work associate professionals) could also be ’rewarding’. For example, social workers may feel positive when someone would overcome his/her difficulties by following their advice. Another possible explanation could be that subjects who are exposed to high emotional demands at the workplace might have coped with or have adapted to the situation. For example, a nurse who encounters dying patients regularly may adapt to the situation in the long run. More studies are warranted to understand the association and its cellular and molecular underlying pathways.
In the analyses including all three psychosocial factors, we observed that the effect estimates remained similar to the effects of the separate psychosocial factors in the adjusted model. These findings indicate that the effect of psychosocial work factors on blood pressure are independent of each other. In the analysis with combinations of different psychosocial work factors, the joint effects of ERI and job strain/emotional demands remained similar and statistically significant which indicates that the effect of ERI on blood pressure is independent of the other psychosocial work factors. However, we observed a counter effect between job strain and emotional demands which nullified their effects on blood pressure. These findings suggest that the stress induced by each psychosocial work factor might have followed different biological pathways in affecting blood pressure. More studies are warranted to understand the cellular and molecular pathways.
Strengths and limitations
In this study, we included a large general working population of 63 800 occupationally active participants. To our knowledge, this is the first study investigating the association between several psychosocial work factors (ie, job strain, ERI and emotional demands) estimated with three recently developed JEMs and blood pressure. The Lifelines Cohort Study contains a large amount of quality data which allowed us to adjust for multiple important confounders. A strength of our study is that, although we only could include 53.6% of the active workers due to having a CASCOT score ≥60 for the automatic job coding, the differences between the included and excluded participants were very small indicating that selection bias is minimal.
The survey-based JEM is a useful tool in estimating occupational exposures in the general working population. A JEM can easily be applied by using job titles in any given population.39 Since these JEMs were developed in Denmark and applied to the Dutch working population, there is no risk of reporting bias. However, differences in regional and cultural work habits between Danish and the Dutch working population might introduce bias. A huge study population would minimise such bias. Even though the psychosocial JEMs are sex, age and period (2005) specific, they do not account for differences in exposure levels observed between individuals with the same reported job—the assumption of homogeneity.40 The same approximate proxy exposure value is used for all participants in the same job, and the true exposure values of each subject will vary randomly about this proxy with a mean equal to it. This error (known as ‘Berkson error’) leads usually to no or small bias in coefficients of linear or logistic regression; however, precision would be lost due to a wider CI.40
For measuring job strain, the use of a JEM is well established.17 18 Only a few studies have examined emotional demands with a JEM but these studies indicate that emotional demands are suitable for JEM analyses.41 To our knowledge, no study so far has analysed ERI with a JEM and more research is needed to establish if ERI can be appropriately be measured with a JEM.
As our study is cross-sectional in design, reverse causation, that is, high blood pressure causing psychosocial working conditions, is possible. Reverse causation would be in particular a concern, if we had measured working conditions by self-report. In this case, it would have been possible that prevalent hypertension and herewith associated health problems may have caused workers to experience their working conditions as more adverse, for example, as more demanding or less rewarding. However, this was not the case in our study, as we measured working conditions not by self-report from the workers, but by job titles. We cannot rule out, though, that prevalent hypertension may have caused some workers to move to a different job and hereby have caused reverse causation, but we do not regard this as very likely. Further, previous longitudinal studies have shown that psychosocial work factors, measured at a specific time point, are predictive of levels and changes in blood pressure later on,42 which indicates that it is more likely that psychosocial work factors influence blood pressure than the other way around.
Implications
Our current findings are relevant from the public and occupational health and clinical perspective. In the general population, reducing 2 mm Hg SBP might result in reducing risks of mortality related to stroke and coronary heart disease by 6% and 4%, respectively.43 A previous study reported that among participants aged 35–64 years, a 2 mm Hg reduction of DBP would result in decreasing risks of stroke and transient ischaemic attacks, and coronary heart disease by 15% and 6%, respectively.44 Thus, a minor reduction in blood pressure by reducing job strain and ERI may prevent a substantial number of CVD-related morbidity and mortality in the general population.
Conclusions
In the general working population, employees in jobs with high job strain and ERI have higher blood pressure compared with employees with low job strain and ERI. Emotional demands at work are inversely associated with blood pressure. Future studies should focus on investigating if there is a prospective association as well. In addition, from a public and workers’ health point of view, multiple-component interventions (eg, change in processes or tools that concern the workload, team meetings to express difficulties and identify solutions, and technical and professional support) should be implemented to reduce psychosocial stress at the workplace as well to reduce blood pressure and the prevalence of hypertension among workers.45 Furthermore, with the continued development of workplace design (eg, remote work, telework and virtual teams), technological job displacement (eg, artificial intelligence and robotics) and work arrangements (eg, alternative work arrangement including contractors and on-call workers), new psychosocial work factors may evolve or are already present.46 Future studies should embrace the life course principles and ever-changing dynamics of the workplace, the work, and the workforce to examine the association between stress-induced by psychosocial work factors and the health consequences.
What is already known on this subject
To date, the association between psychosocial work factors and blood pressure mainly is based on self-reported exposures, specific occupations or populations and limited sample sizes.
What this study adds
Our study included a large general working population and strengthens the evidence that job strain and effort–reward imbalance (estimated with psychosocial job-exposure matrices) are associated with high blood pressure. In contrast to our hypothesis, emotional demands at work are inversely associated with blood pressure.
This research suggests that measures should be taken to prevent or reduce job strain and effort–reward imbalance at the workplace.
Data availability statement
Registration is required to obtain data from the Lifelines cohort study. It is not permitted to deposit the Lifelines data in an open data repository. To obtain data, used in the current study, interested researchers should contact the Lifelines Cohort Study (www.lifelines.nl).
Ethics statements
Patient consent for publication
Ethics approval
The Lifelines Cohort Study was approved by the Medical Ethical Commission (METC) of the University Medical Center Groningen (Reference number-2007/152). All subjects signed written informed consent and all methods were carried out in accordance with relevant guidelines and regulations for human subjects.
Acknowledgments
The authors thank all the residents from Friesland, Groningen and Drenthe, the Netherlands who have participated in the Lifelines Cohort Study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Author contributions All authors contributed to the conception, design, and interpretation of the results. MOF analysed data, produced tables and graphs, and wrote the first version of the manuscript. JMV, HMB, UB, EF, JKS, RER and IM critically reviewed the manuscript, tables and graphs, and supplementary materials. All authors approved the final version of the manuscript.
Funding MOF was supported by the Ph.D. Scholarship programme of the Graduate School of Medical Sciences (GSMS), University of Groningen. The Lifelines Cohort Study was supported by the Dutch Ministry of Health, Welfare and Sport, the Ministry of Economic Affairs, Agriculture and Innovation, the Province of Groningen, the European Union (Regional Development Fund), the Northern Netherlands Provinces (SNN), the Netherlands Organization for Scientific Research (NWO), the University Medical Center Groningen (UMCG), the University of Groningen, de Nierstichting (the Dutch Kidney Foundation) and the Diabetes Fonds (the Diabetic Foundation). EF, JKS, IM and RR were supported by grants from NordForsk (#75021) and the Danish Working Environment Research Fund (27-2017-03).
Disclaimer The sponsors of this study had no role in the design of this study, data collection, analysis and interpretation or in writing and submitting of the manuscript.
Competing interests The corresponding author, HMB, declares (after collecting completed Unified Competing Interest form from all the authors) no support from any organisation for the submitted work, no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.