Article Text

Abstract
Heterotopic ossification (HO) is the formation of mature lamellar bone in extraskeletal soft tissues. It was first described 1000 years ago in the healing of fractures, and in relation to military wounds, texts from the American Civil War and World War I refer to HO specifically. It continues to cause problems to injured service personnel; the consequences of wound and soft tissue complications in traumatic amputations pose particular problems to rehabilitation and prosthetic use. While HO is seen in rare genetic conditions, it is most prevalent after joint replacement surgery and trauma. In the civilian setting HO has been commonly described in patients after traumatic brain injuries, spinal cord injuries and burns. Militarily, as a consequence of recent operations, and the characteristic injury of blast-related amputations, a renewed interest in HO has emerged due to an increased incidence seen in casualties. The heterogeneous nature of a blast related amputation makes it difficult for a single aetiological event to be identified, although it is now accepted that blast, amputation through the zone of injury, increased injury severity and associated brain injuries are significant risk factors in HO formation. The exact cellular event leading to HO has yet to be identified, and as a consequence its prevention is restricted to the use of anti-inflammatory medication and radiation, which is often contraindicated in the acute complex military casualty. A systematic review in PubMed and the Cochrane Database identified research articles related to HO to illustrate the military problem of HO and its management, current research concepts and experimental theories regarding HO. This also served as a gap analysis providing the researchers detail of any knowledge deficit in this field, in particular to the military aspects of HO; 637 out of 7891 articles initially identified that referenced HO were relevant to this review.
- PLASTIC & RECONSTRUCTIVE SURGERY
- REHABILITATION MEDICINE
Statistics from Altmetric.com
Introduction
Heterotopic ossification (HO) (Figure 1) is the formation of mature lamellar bone in extraskeletal soft tissues. It was first described in the literature nearly 1000 years ago in the healing of fractures,1 and in relation to military wounds, and complications of amputations, texts from the American Civil War and World War I make specific reference to it.2 To date HO continues to cause problems to the injured service personnel3 ,4 with its consequences posing particular difficulties to rehabilitation5 ,6 and long-term prosthetic use.3

Heterotopic ossification in a transfemoral amputee.
It can be classified into congenital or acquired; the latter usually being associated with trauma. In the military and the civilian settings traumatic brain injury (TBI) and traumatic amputations are recognised risk factors for HO7–9; despite these associations the exact pathogenic mechanism remains elusive.
The prevalence of HO in the military setting is reported to be increasing.10 This is thought to be due to increased survivorship of casualties with more severe extremity injuries seen in recent operations.11 In addition the characteristic mechanism of injury seen in operations in Afghanistan, and the latter stages in Iraq, has been blast from improvised explosive devices (IEDs). Many studies have tried to identify causal factors from the mechanism of injury, management of wounds and complications and the subsequent formation of HO.4 ,9 However with so many variables involved in the formation and treatment of a complex military wound, it is difficult to isolate a single aetiological event.
Due to the injury severity of the casualty, and the complexity and highly contaminated wounds, primary prevention is unlikely to be possible; therefore the military surgeon is left with little in his armoury apart from surgical excision, after the formation of HO. Case series of individual department experiences in the management of HO are seen in the literature10 ,12 but there is no consistent management consensus.
Until recently research and evidence concerning HO has been led by civilian academic departments, however the increased prevalence and functional compromise has driven the military requirement for further work on its aetiology, structure, biology, prevention and treatment. To identify scientific needs and future research directions, a systematic review of literature related to HO was performed.
Methods
We employed ‘PRISMA’ systematic review guidelines; searching the PubMed database for references using the search terms ‘heterotopic’ and ‘ossification’ as keywords, and limiting our search to the last 100 years. Primary and secondary exclusion criteria were then used to filter the results (Table 1) after a secondary filter, further filtering, or the use of additional keywords, was found to over-refine our search and significant articles excluded. Therefore it was felt that further searches should be done manually. Manual strategies employed to establish relevance, in order of hierarchical importance, were (1) Title review, (2) MeSH term review, (3) Abstract review and finally (4) Full article review. A flow chart of the search is demonstrated in Figure 2. Relevant articles were subsequently grouped into related subjects (Table 2).
Filter levels and elements
Relevant article grouping

A flow chart of the review process.
Results
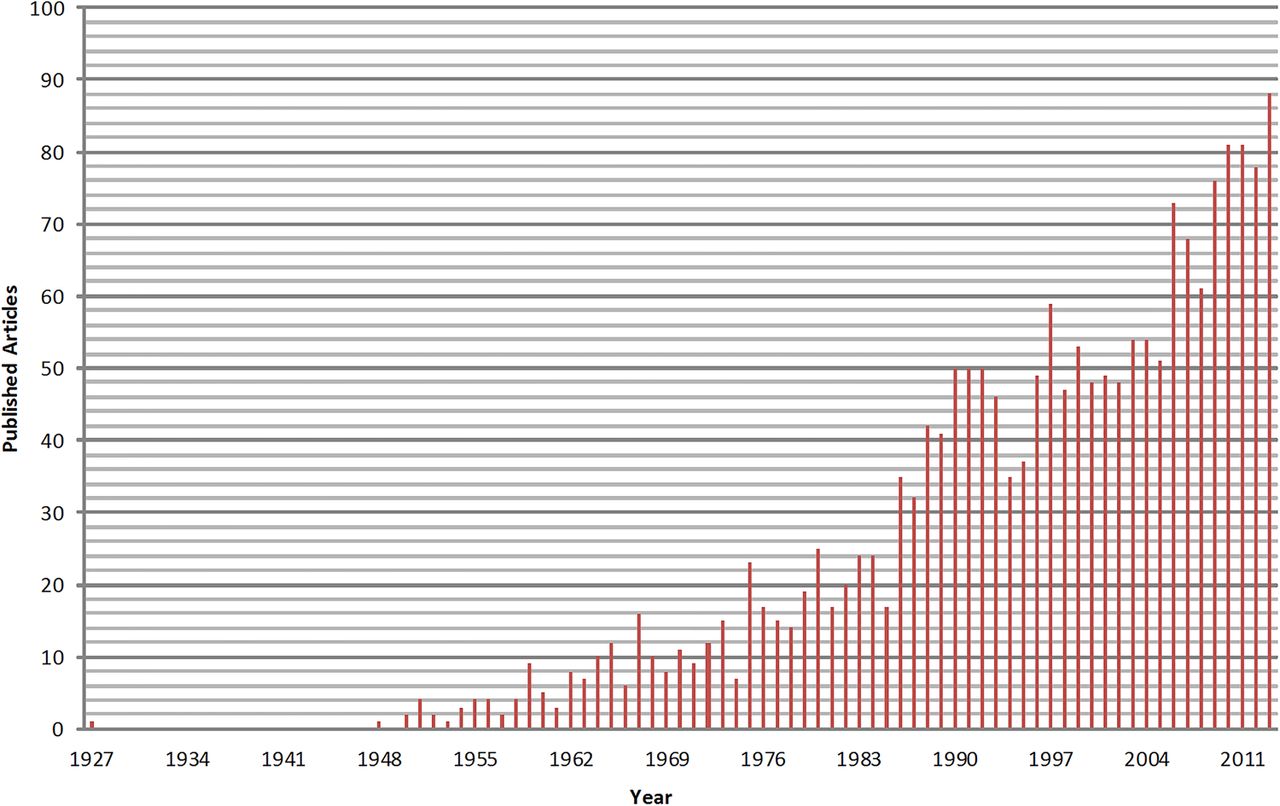
Initially 7891 articles related to HO (Figure 3) were identified which was reduced to 637 after refining the search using the primary, secondary and manual exclusion strategies. The number of articles published in the last 10 years increased from 54 to 88, between 2003 and 2013. Three distinct groups of research were evident, elective surgery, trauma surgery and scientific basis of disease, representing 54%, 25% and 21%, respectively, of the articles published. The most common publication subject was that of HO related to hip arthroplasty (n=218, 34.2%). Only 26 articles were found referring to HO in the military trauma setting.

Numbers of published articles on heterotopic ossification by year.
One limitation encountered in the systematic review was a change in nomenclature of HO. Terms such as ectopic bone formation, myositis ossificans and heterotopic ossification were used interchangeably in history.
Normal bone formation
Prerequisites for bone formation are inductive signalling pathways, consisting of chemical mediators (chemokines and cytokines), including bone morphogenetic protein (BMP), platelet derived growth factors, fibroblast growth factors, prostaglandins (PGs) and interleukins, all of which trigger bone formation; inducible osteoprogenitor cells which are cells capable of being differentiated into bone forming osteoblasts and finally an environment conducive to osteogenesis (a scaffold for the deposition of new bone).7 ,10 (Figure 4) In the normal physiological state these prerequistes exist, together with osteoclast resorption, to allow a slow metabolic turnover of normal bone. This enables the skeletal system to continuously adapt to changes in normal physiological loads, such as growth or increased physical activity

Biological prerequisites for heterotopic ossification.
Scientific basis of disease
Genetics
HO can be divided into congenital (or genetic) and acquired. Acquired causes are by far the most common; however, genetic causes provide evidence of the genetic basis for the formation of HO. Two congenital conditions exist specifically related to the formation of ectopic bone. Fibrodysplasia ossificans progressiva (FOP) and progressive osseous hyperplasia are rare genetic conditions which result in severe disability secondary to extensive bone formation in all soft tissues.13 In FOP the exact mutated gene has yet to be identified and is usually a spontaneous occurrence, but where familial tendency exists it seems to confer an autosomal dominant pattern.14 In the early stages of the disease a lymphocyte-associated mechanism has been identified thereby inferring an inflammatory pathogenic process.15 Geneticists have demonstrated that the expression of BMP-4, an inflammatory mediator, is significantly increased in cases of FOP.16 The downregulation of Noggin, a BMP-4 antagonist has also been shown in FOP.17
An autosomal inheritance pattern is seen in progressive osseous hyperplasia with the heterozygous inactivation of the GNAS1 gene exclusively inherited from the father.18 This results in decreased expression of the stimulatory G protein of adenylyl cyclase, another inflammatory mediator. BMP-4 and stimulatory G protein are associated with bone formation.
Pathological bone formation
The relevance of normal bone formation to pathological bone formation is summarised by Kirsch who states that the molecular mechanisms that are normally found regulating physiological bone formation and turnover are present in pathological conditions of ectopic bone formation in the skeletal system, and extraosseous soft tissues such as cartilage, blood vessels and muscles.19 How this is achieved in the soft tissues of blast related patients is unknown. However, with the release of cytokines and chemokines seen in blast related tissues,20 which are capable of the stimulation of osteogenesis and the recruitment of bone forming units, an inflammatory mediated cellular mechanism is likely. Proinflammatory mediators, platelet derived growth factors,21 fibroblast growth factors,22 transforming growth factor-β,23 insulin-like growth factor I24 and insulin-like growth factor–II,25 epidermal growth factors,26 and PGs27 have all been implicated in osteoblast DNA synthesis and are present in bone matrix. Analysis of wounds further details that certain inflammatory cytokines and chemokines were upregulated as a consequence of high energy penetrating extremity wounds. Serum factors identified were IL-6, IL-10 and human monocyte chemotactic protein-1. Wound effluent proteins upregulated were macrophage inflammatory protein-1α and interferon-γ-inducible protein-10.28 This biochemical evidence suggests that the formation of HO is associated with a systemic and localised hyperinflammatory response to the index injury. Laboratory manipulation of local and systemic cytokines have been proven to influence stem cell differentiation. Progenitor cells from muscle, periosteum and capillaries are capable of differentiation into osteoprogenitor cells thereby providing osteoblast precursors in the generetaion of new bone.29 Further modulation of local stem cells is possible by the intrinsic nature of the local tissue. It has been recently reported that a strict acidic environment is capable of reprogramming pluripotent cells from one cell lineage to another, thereby demonstrating bidirectional manipulation.30 ,31
Experimental models of heterotopic ossification
Urist reported an experimental model of new bone formation after trauma in the 1930s.32 Prior to that Blessig published the ossification of the kidney in response to ischaemia caused by ligation of the renal artery in rabbits. Subsequently the identification, and isolation, of BMPs have allowed controlled osteoinduction within animal soft tissue models.
Broadly speaking three basic models of HO formation are now described33: Trauma-induced animal models; animal osteoinductive models (the interaction of native undifferentiated cells and implanted BMPs) and osteogenetic cell transplantation models.
With the recognition that the formation of HO is related to a blast injury and amputation through the zone of injury, laboratory experiments, including cellular and animal models, have been designed.34–36 A physiological model aims to combine all three basic models of HO formation where the blast wave causes localised injury and ischaemia, amputation results in release of mesenchymal stem cells residing in the bone canal and subsequent inflammation causing the release of inflammatory mediators, including BMPs. The heterogeneous events surrounding HO formation lead to experimental difficulties. Tannous reported good results from a Sprague-Dawley rat animal model, however concerns lay in the delivery of the blast (water column) and relatively low survival rate.36
Elective surgery related heterotopic ossification
Hip arthroplasty
Over the last 50 years, total hip arthroplasty (THA) has become increasingly common in the management of hip arthritis. The formation of HO post surgery is frequently noted20 and its incidence has been reported to range from 8%37 to 90%.38 However, Brooker et al report the incidence of HO resulting in significant disability is limited to those with high grades of HO and demonstrate, using their classification, that it is the final stage of ankylosis (Grade 4) that is most problematic for the patient.39 In the civilian setting the principles of management of HO is that of primary prevention in higher risk patients. The recognised methods of prevention are the use of non-steroidal anti-inflammatory drugs, or cyclo-oxygenase-2 (COX-2) selective non-steroidal anti-inflammatory drug, and radiation therapy.40
Heterotopic ossification prophylaxis
A Cochrane Review, which included 16 Level 1 trials, demonstrated the benefit of regular indomethacin use during THA reporting a 59% reduction in the incidence of HO.40–42 The mechanism of action is via a combined effect of inhibition of mesenchymal stem cells and the suppression of inflammation by the inhibition of PG.43 However it was noted in these articles that the side effects of gastrointestinal ulcers and increased risk of postoperative bleeding were not benign. This has led to a preference for COX-2 inhibitors.
The inhibition of bone growth by radiation was established over 50 years ago.44 Doses in excess of 20 Grays resulted in the suppression of vertebral growth in children. This has been exploited in orthopaedics during THA.45 Preoperative or early postoperative local exposure of 7–8 Grays has been demonstrated to prevent the formation of HO45–47; however the timing is relevant. By the 3rd postoperative day the mesenchymal stem cells have already differentiated, and treatment after this time is ineffective.48
Trauma related heterotopic ossification
Civilian
Post-traumatic HO, traumatic myositis ossificans and myositis ossificans circumspecta are all terms that have been used to define the same problem—that of bone formation outside the skeletal system following trauma. In general the trauma in which HO is formed ranges from muscle sprains and contusions through to open fractures of long bone.49 HO is seen in civilian, as well as military practice; its formation is often subclinical and noted incidentally on radiographs. However, in particular during major trauma, the formation of HO may compromise rehabilitation if formed around large joints or dependent limbs. In the trauma environment, the literature demonstrates that plastic surgeons have referenced, and investigated, that in patients with TBI and spinal cord injury (SCI), HO is a well-recognised phenomenon and its incidence ranges from 10% to 20% of patients suffering a TBI and 20% to 30% of patients with SCI.50–52 Neurogenic HO (NHO) has been demonstrated to have a genetic element; the injury dictating the temporal relation to its formation while the presence of HLA B27 identifying the population at risk of HO.53 The absence of HLA B27 does not preclude the formation of NHO.53 HLA B27 is associated with inflammatory arthropathies such as ankylosing spondylitis and seronegative spondyloarthropathies such as Reiter's disease.54 Despite the fact that a genetic predisposition is present, centrally released humoral factors previously described continue to be shown to drive bone formation.55
Military
HO has been described in history for over a 1000 years56; observed in amputees from the American Civil war,51 World War I2 and the recent conflicts in Iraq and Afghanistan.4 ,28 ,57–59 Contemporary military operations have demonstrated an increased prevalence of HO in military wounds, when compared with civilian counterparts.4 ,51 ,52 The increase in its incidence from veterans serving in the US forces during Operation Iraqi Freedom and Operation Enduring Freedom has resulted in a renewed interest in HO and its extent documented in American and British military literature.4 ,9 The increased prevalence in recent conflicts may be due to increased survivor rates due to enhanced body armour, rapid medical care to the severely injured solider and subsequent increased survivorship, as well as the mechanism of injury, particularly the IED. Specific wound related factors that correlated with the development of HO included impaired healing and bacterial colonisation.28 Disturbance of local microvasculature renders the soft tissues susceptible to HO formation. Localised changes in the arterial supply and reduced oxygen tension render the soft tissues hypoxic and acidic. This favours mineralisation and bone formation as the oxygen tension is recovered through surgery or ventilation.60 ,61 The acidic environment may also be capable of modulating the cell lineage in soft tissues.30 ,31
In recent operations, the incidence of HO has been reported as 60–64%.4 ,58 Box 1 details the factors that, demonstrated in a comparative paper between the UK and USA, place the military casualty at risk for the development of HO.4 It is likely that systematic and local factors come into play in the formation of HO (Figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Interaction of local and systemic factors in the formation of heterotopic ossification.
Current and potential future military issues
With amputees seen from operations in Afghanistan11 and a high rate of HO, rehabilitation may be compromised in this casualty group to a greater extent than previously seen. Significant disability has been reported in casualties from Vietnam with unilateral transfemoral amputations and the majority of bilateral transfemoral amputees in the Vietnam cohort abandoned their prosthetics and rely on a wheelchair for mobility; it was prosthetic related issues that led the patient abandoning a prosthetic.3 ,62
The current management of HO is restricted to operative excision in symptomatic patients who have failed non-operative management such as rest, adjustment of pain medication, selected injections, and nerve ablation of neuromas, socket modification and physiotherapy.10 ,63 Separately published British and American military experience in surgical excision appears similar.58 ,63 Multiple centres in the UK and the USA report the necessity of primary excision of symptomatic HO within the 1st year after injury, combined with indomethacin or COX-2 use. Good functional outcome and no significant recurrence at 12 months after surgery with this approach are seen.59 Additionally, British Plastic and Reconstructive surgeons at the Royal Centre of Defence Medicine described a technique of serial operations to elevate, protect or excise overlying skin and soft tissues to improve the weight bearing surface.63
Required research
Animal heterotopic ossification model
HO formation in rodents has been achieved but included cytokine modulation of the animal.35 The model produced by Tannous et al used local blast to the lower limb and therefore systemic causes of blast related HO were not taken into account.36 However, Alfieri et al describe ongoing work at Walter Reed National Military Medical Center, of a reliable reproducible systemic blast model with open fractures, wound ischaemia, a large zone of injury, an appropriate bioburden and amputations through the zone of injury.58 The required experimental animal model for HO formation is a complex one. However, a reliable small animal model requires validation and to be expanded to larger species. Once established, individual variables, such as blast magnitude and morphology, infection, surgical debridement zones and local biomechanics, can be manipulated to help in the prevention and management of HO.
Cellular level
To date a reliable cellular model of HO formation secondary to blast has yet to be published. Detailed structural evaluation is still lacking in the literature. Limited imaging techniques are described, however, detailed structure of the cortex and lamellar configuration of HO, in comparison with normal bone, is yet to be seen. This would also provide control data to samples retrieved from experimental models.
Military aetiological factors
The comparative study by Brown et al showed significant similarities between the UK and US experiences of wounds and subsequent HO formation in Iraq and the early years in Afghanistan.4 However, the UK data set only included casualties up to 2008. It is well recognised that the modus operandi of the Taliban and insurgents changed at this time to the use of IEDs of greater magnitude.
Muscle ischaemia and necrosis are believed to be related to HO formation.64 Therefore tourniquet related data requires comparison in these subjects and larger subject numbers are required to further evaluate the link to topical negative dressings and HO, that was noted previously.4
Management of HO in military population
Military amputees requiring surgery for wound and residuum related problems during rehabilitation, such as those seen in limbs complicated by HO, are referred from their rehabilitation centre to secondary care specialists for surgical management throughout the UK. This provides an opportunity for data analysis on protocols used and complication/recurrence rates after HO surgery at different centres. Ideally a prospective cohort study in the use of medical and surgical strategies in management of HO should be considered. However, a retrospective comparative multiarm case series would give direction to future research. The timing of HO excision may be the key; as detailed previously, surgery is contemplated when rehabilitation is compromised. However, once risk stratification is analysed, and when HO can be clinically recognised early in its development, surgery may be expedited to prevent rehabilitation delays.
Conclusion
It is likely that HO will continue to compromise the rehabilitation and long-term outcome of the cohort of traumatic amputees from operations in Afghanistan, the magnitude of which, while at present is unknown, is likely to reflect the experience in Iraq and the early stages of Afghanistan. As noted, there remain significant gaps in the understanding of this condition. Work is required in this field to fully understand its pathogenesis from the triggering traumatic event, cellular inception to primary prevention. Understanding the key to unlocking its formation is likely to help its prevention and/or subsequent management.
Casualty factors leading to increased risk of heterotopic ossification (HO)4
Age
Blast mechanism of injury (MOI)
Zone of injury (ZOI) and subsequent amputation
Injury severity score >16
Topical negative pressure (TNP) dressings
Traumatic brain injury (TBI)
Multiple extremity injuries
Number of debridements before closure
References
Footnotes
Contributors DSE: main researcher and author. JCC: research supervisor and guarantor.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.